
Abstract
BACKGROUND:
Some disabled persons especially those with Down syndrome have cardiorespiratory disorders that negatively influence their daily life. Strength training for respiratory muscles may positively affect daily life of such disabled persons.
OBJECTIVE:
The purpose of the study was to investigate the effects of inspiratory muscle training on respiratory functions and respiratory muscle strength in individuals with Down syndrome.
METHODS:
Sixteen individuals were enrolled and divided into experimental (
RESULTS:
Significant pre-post changes were found in the respiratory functions and respiratory muscle strength of the experimental group (
CONCLUSIONS:
Inspiratory muscle training is likely to have a positive effect on respiratory functions and respiratory muscle strength in individuals with Down syndrome.
Introduction
Almost every living organism needs oxygen to maintain life activities. The respiratory system, which supplies oxygen to the body plays an important role in determining the performance level at work. A healthy respiratory system increases the productivity of the people by making them more active and efficient [7].
The respiratory muscles must be strong and flexible for an individual to be productive in daily life and during exercise [27]. To improve their strength the respiratory system provides increased levels of inhaled oxygen and modifies the contraction of the muscles [12]. The diaphragm is the most important and largest muscle that helps in respiration. Strength training for respiratory muscles positively affects an individual’s life. This training is more important for disabled persons, especially those with Down syndrome who have cardiorespiratory disorders [21].
Exercise performed for strengthening of the respiratory system may enhance their strength and endurance [32]. It can help individuals with getting rid of problems such as dyspnea in individuals with chronic obstructive pulmonary disease (COPD). Inspiratory muscle training provides multiple benefits such as increased muscle endurance, high quality of life, and increased muscle strength [15, 17]. These benefits can also apply to individuals with Down syndrome with a significant improvement in parameters such as respiratory muscle strength, endurance, and respiratory functions.
Studies have shown the positive effects of respiratory muscle training on respiratory functions and respiratory muscle strength in healthy individuals [8, 33], patients with COPD [22, 25, 28], paraplegia [37], muscular disease [34], neuromuscular disease [5], asthma [31], and multiple sclerosis [35], and athletes [33]. However, no study has investigated the effects of inspiratory muscle training on individuals with Down syndrome (IwDS) who present with some congenital respiratory problems such as flattened nasal bridge, shortened and narrowed ear canals, large protruding tongue, small mouth, shallow hypopharyngeal dimensions, abnormal lung growth and airway malacia [38, 39, 40, 41]. These factors cause vital respiratory problems along with lack of respiratory muscle tone and strength [38, 42]. We hypothesized that inspiratory muscle training would have a positive effect on respiratory muscle strength and respiratory pulmonary function in IwDS, hence this study.
Methods
Participants
In total, 16 individuals with Down syndrome were enrolled (Table 1). A priori test with GPower 3.1 program was used for determining the number of participants. The aim of the study was explained to the participants and their parents before beginning the study, following which a voluntary consent form was signed by them. The participants, with their parents, visited the laboratory three times. Before the training period, the first visit included familiarization with the exercise and measurement protocol. In the second and third visits, pre- and post-test were, respectively, performed. The study was conducted in accordance with Helsinki Declaration, and approval was obtained from the Gaziantep University Clinical Research Ethics Committee.
Descriptive parameters of the subjects (experimental;
9, control;
7)
Descriptive parameters of the subjects (experimental;
BMI; body mass index, MEP maximal expiratory pressure; MIP maximal inspiratory pressure; FVC forced vital capacity; FEV1 forced expiratory volume in one second; PEF peak expiratory flow; PIF peak inspiratory flow; MVV maximal voluntary ventilation; VC vital capacity; TV tidal volume; IVC inspiratory vital capacity.
This study was designed as a controlled pre- and post-test procedure. Participants were randomly divided into two groups with block randomization technique as experimental group (
Inspiratory muscle training protocol
The experimental group performed the inspiratory muscle training program for 5 days a week for a month. The participants breathed 30
Respiratory muscle strength measurement
Electronic respiratory pressure meter (Pocket Spiro MPM-100, Medical Electronic Construction R&D, Brussels, Belgium) was used for MIP and MEP calculation according to the 2002 guidelines of the American Thoracic Society and European Respiratory Society. For MIP measurement, participants performed maximal expiration, immediately following which they were asked to perform maximal inspiration for 1–3 s. For MEP measurement, the participants performed maximal inspiration, following which they were immediately asked to perform maximal expiration for 1–3 s. The measurements were repeated until the difference between the best two measurements was 5 cmH
Pulmonary function measurements
The pulmonary function was evaluated using a spirometer (Pocket Spiro USB-100, Medical Electronic Construction R&D, Brussels, Belgium). Slow and forced vital capacity tests were selected and measured according to the 2002 guidelines of the American Thoracic Society and European Respiratory Society. Variables such as forced vital capacity (FVC), forced expiratory volume in one second (FEV1), FEV1/FVC, peak expiratory flow (PEF), peak inspiratory flow (PIF), maximal voluntary ventilation (MVV), vital capacity (VC), tidal volume (TV), inspiratory vital capacity (IVC) were recorded using pulmonary function test [20]. Subjects performed twice all of respiratory function measurements, and we have recorded the measurement with higher data.
Statistical analyses
SPSS 22.0 (SPSS Inc., Chicago, IL, USA) program was used for statistical analysis. Values were represented as minimum, maximum, mean, standard deviation, standard error, and 95% confidence interval, and significance was set at 0.05. Shapiro–Wilk test was performed to assess normality, and 2
Analysis of changes in respiratory muscle strength parameters (Mean
SD)
Analysis of changes in respiratory muscle strength parameters (Mean
Table 2 shows the analysis of changes in respiratory muscle strength parameters of the participants. The results showed that MEP significantly changed post-test in the experimental group. Furthermore, in terms of percentage difference between the groups, the change in MEP in the experimental group was significant compared with that in the control group. MIP, which is another respiratory muscle strength parameter, showed a significant change post-test. Furthermore, in terms of percentage difference between the groups, the change in MIP in the experimental group was significant compared with that in the control group (Fig. 1).
Percent changes in the respiratory muscle strength and respiratory function parameters of groups. MEP maximal expiratory pressure; MIP maximal inspiratory pressure; FVC forced vital capacity; FEV1 forced expiratory volume in one second; PEF peak expiratory flow; PIF peak inspiratory flow; MVV maximal voluntary ventilation; VC vital capacity; TV tidal volume; IVC inspiratory vital capacity; SD standard deviation. 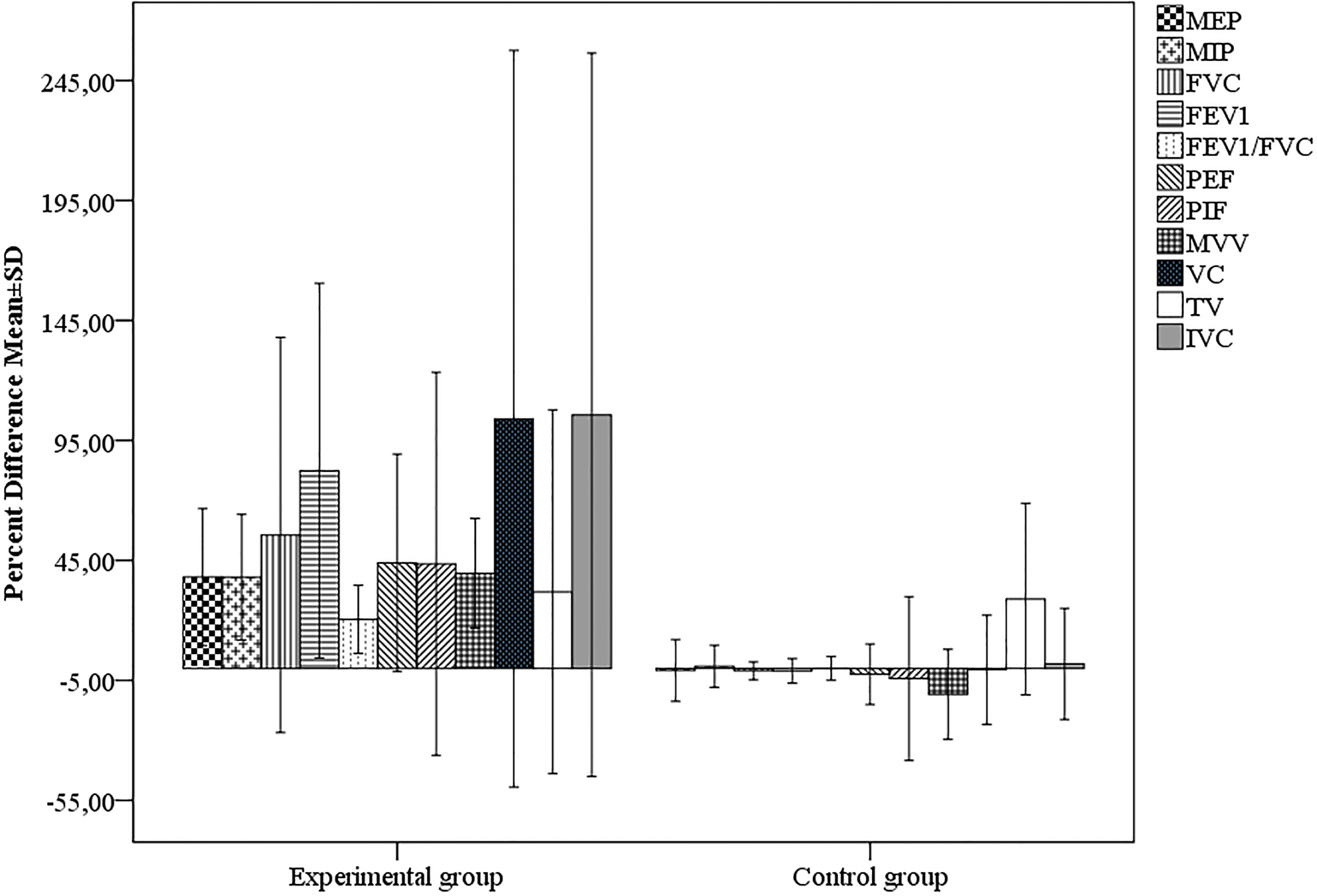
Table 3 shows the analysis of changes in respiratory function parameters of the participants. Except in TV, there were significant changes in all respiratory function parameters, mean differences and percent differences (Fig. 1).
Analysis of changes in the respiratory function parameters (Mean
The aim of this study was to investigate the effect of inspiratory muscle training on respiratory functions and respiratory muscle strength in individuals with Down syndrome. Due to training, significant improvements were observed in the strength parameters (MEP and MIP) as well as in the respiratory functions; all respiratory function parameters, except TV, showed a significant pre-post change. The latter finding may be associated with lack of change in the respiratory frequency.
The effects of inspiratory muscle training on respiratory muscle strength have been studied [4, 10, 16] but not in individuals with Down syndrome. An earlier study has shown that inspiratory muscle training is effective for improving inspiratory muscle strength, endurance, and exercise capacity of patients with COPD [36]. Recent studies on the effect of inspiratory muscle training on respiratory functions in patients have reported significant improvements in respiratory functions after training [5, 8, 31]. In this study, the inspiratory muscle training positively affected respiratory functions. The significant change was due to the fact that this training improves respiratory muscle function by enhancing the contraction and relaxation capacity of these muscles [33].
The improvement in respiratory functions may be explained by increased respiratory muscle strength but may have also occurred due to decreased stiffness in the respiratory muscles, increased nerve conduction velocity, increased contractility, altered power-acceleration correlation, and increased metabolic enzyme activation in the respiratory muscles [13, 24, 26, 29]. Skeletal muscles control a number of vital factors during breathing. These vital factors are entirely related to airway and thorax movements [19]. Due to the increased respiratory muscle strength, the respiratory function parameters also improved as reflected by the increased airway performance [11]. At the same time, the improvement in respiratory functions may be attributed to the positive effects of strengthening of respiratory muscles on respiratory mechanics [18].
Recent studies have reported that the respiratory training or respiratory rehabilitation has a positive effect on respiratory functions, especially in patients [2, 3, 9, 25]. Our study demonstrate that respiratory functions significantly change due to increased respiratory muscle strength as a result of 4 weeks of training.
The findings and interpretation of the present study are limited both by the small sample size and the great difficulty in matching experimental and control groups. Children with Down syndrome show a wide range of the functional performance handicaps, growth features, and pubertal development according to gender [43, 44, 45, 46]. From this perspective, gender, as a variable, is another limitation of the present study.
In conclusion, inspiratory muscle training may be effective for improving respiratory functions and respiratory muscle strength in individuals with Down syndrome, This improvement likely results from the positive effects of increased strength of respiratory muscles on respiratory mechanics.
Footnotes
Acknowledgments
The present study was supported by grants from Gaziantep University as scientific research project (BSY.YLT.17.04).
Conflict of interest
The authors declare no conflict of interest.