
Abstract
BACKGROUND:
Research suggests that the effect of short bouts of stretching on muscle strength and ROM gains depends on the total stretching volume.
OBJECTIVE:
We assessed the effects of short bouts of static passive (SSS) and contract-relax (SCR) stretching on range of motion (ROM) and muscular strength.
METHODS:
Twenty volunteers performed two stretch protocols in a randomized order on two separate days, using the SSS and SCR techniques. Maximal ROM was tested prior to (pre-S), immediately after (post-I) and 10 minutes after (post-10) the stretch protocol. Maximal isometric voluntary contraction (MVC), isokinetic concentric peak moment (F-PM) and angle of peak moment (F-PMa) in the knee flexors, and concentric flexion/extension PM ratio (F/E) were measured and evaluated before (pre) and after (post) the stretch protocol.
RESULTS:
Both stretching techniques showed significant time-effects (pre vs post-I and post-10) but no interaction effects (time
CONCLUSIONS:
Short-stretch techniques have trivial and small effects on loss of strength, increase the ROM for at least 10 min and slightly decrease the concentric F/E ratio. Using SSS could create some risk of hamstring injuries.
Keywords
Introduction
Stretching immediately prior to exercise has been claimed to decrease results in performance tests that require isolated force or power, and during the warm-up period, stretching has been shown to decrease several muscular performance variables [1, 2, 3].
However, the dose-response relationship between stretching and decreased muscle strength is still unclear. In addition, the procedures carried out during experimental protocols are not normally representative of stretching bouts during normal athletic warm-up procedures, as the former are usually more time-consuming [4].
The observed impairment may be related to a number of factors. Among these, stretch-induced strength loss is dependent on the specific muscular activation used for measuring strength loss, the muscle length at which strength is measured, the stretch intensity and stretching technique applied [5, 6, 7, 8], and the duration of the stretch [9].
Recent studies suggest that short-duration static stretching (SSS) prior to strength testing does not result in any significant reduction in muscular strength when the duration of the stretch is
Other reports showed that static stretching (
It appears that stretches of short duration do not provide sufficient stimulus to elicit performance impairments following a dynamic warm-up [20] or when followed by dynamic stretching [21]. However, SSS protocols seem to increase the ROM and they could be as effective as longer duration stretches [22].
Contract-relax stretching is a proprioceptive neuromuscular facilitation technique (PNF) that involves an isometric contraction in the target muscles while in a stretched position, and upon relaxation, the stretch is either maintained or increased to a greater range of motion. The contract-relax stretch technique appears to generate greater or similar overall strength losses compared with static stretching [23, 24], possibly due to higher muscle relaxation and subsequently increased muscle compliance [27]. However, self-administered PNF of short duration (5 s) does not appear to change the maximal voluntary contraction force [25].
Stretching and maximal muscle performance relationships have recently been questioned in narrative reviews [6, 12] and one systematic review [11]. This review revealed that while some studies have reported significant losses in lower limb muscle groups, others did not, and that overall, 50% of the findings indicated that no detrimental effects on strength were likely when the static stretch duration was 30–45 s, with the pooled estimate of the changes (
The aim of this study was to analyse the acute effects of similar short-duration stretches and stretch tolerance dosages in two stretch techniques – short-duration static passive (SSS) and short-duration contract-relax (SCR) – in terms of their effect on maximal ROM and isometric and isokinetic muscular strength in knee flexor and extensor muscles.
Methods
Partcipants
Twenty healthy recreationally active male sports science students (age 21.92
Timeline with the assessments at baseline, intervention and post-test within an experimental session.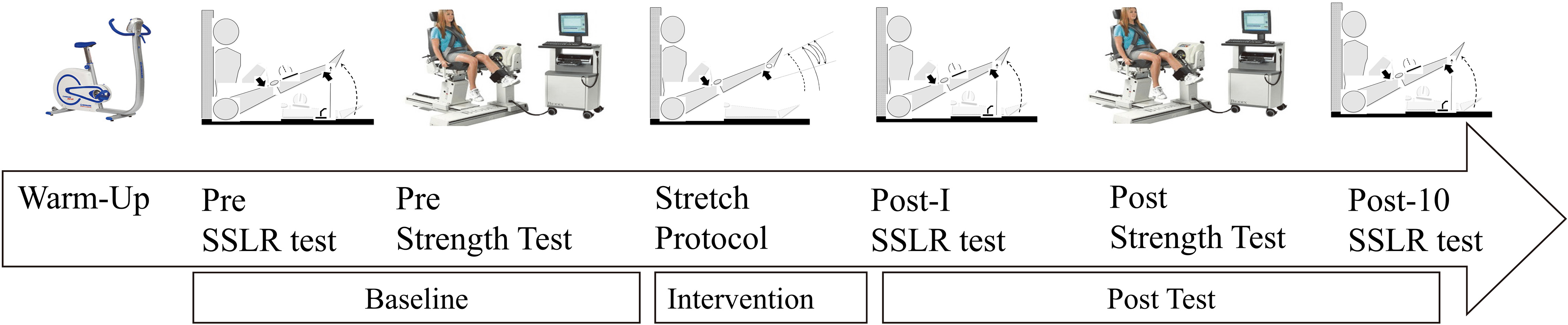
All participants carried out both experimental stretch protocols (separated by 24 h) and their intra- and inter-stretch techniques were compared. Each participant completed a 5 min warm-up at 50–60 W (between 60–70 RPM) using a stationary cycle ergometer (Monark Ergomedic 828E), a pre-ROM assessment, pre-stretching strength tests, the stretch protocol, an immediate post-ROM assessment, post-stretching strength tests and a 10 min post-ROM assessment (Fig. 1).
Peak moment, angle at peak moment in maximal isometric contraction, concentric maximal muscular voluntary exertion and conventional concentric knee flexor-knee extensor ratios at higher peak moment angles in the knee flexor and extensor muscles were measured using an isokinetic device (Cybex Norm, Lumex, Ronkonkoma) for strength tests. The maximal passive hip flexion angle-ROM (stretch test) was evaluated using a seated straight leg raise test (SSLR), and was evaluated prior to (pre-S), immediately after (post-I) and 10 min after (post-10) each stretch protocol (Fig. 1). Stretch techniques and use of the dominant or non-dominant leg were randomized for each subject. The stretch protocol was performed using the SSS stretch technique and 24 h later performed using the SCR technique with the other leg and in the same position and vice versa.
Instrumentation and measurements
ROM assessments
To estimate the passive resistive moment in hip flexion ROM (musculotendinous passive stiffness; MTS) we used a seated straight leg raise test (Fig. 2A). After the warm-up and prior to the first strength test, each participant was placed in the rest position and the same investigator applied the corresponding stretch protocol. To avoid pelvic tilt when stretch was applied to a leg, the other leg was flexed and fixed, and the back of the head, upper back and the points of the ischial bones were in contact with the wall and the floor respectively when the movement was executed. The leg being tested was stabilized and restrained to avoid any knee flexion when slowly raising the leg. To ensure a similar intensity of stretch, each participant indicated the correct maximal stretch position (by saying “stop”) when they reached the threshold for their individual POD. For the correct stretch amplitude position (similar intensity) each subject was placed in the same region using the Visual Analogic Scale pain ruler (VAS) (Schlenker Enterprises Ltd, Lombard, USA), independently of the ROM achieved in the previous set.
Seated straight leg raise test (SSLR) (A) and stretch techniques intervention protocol (B). Wide black arrows show the positions selected to stabilize and restrain knee joint movement and avoid knee flexion when slowly raising the leg in both the SSLR and stretch protocols. Wide white arrow indicates the leg’s direction against resistance offered by the examiner in the SCR stretch technique.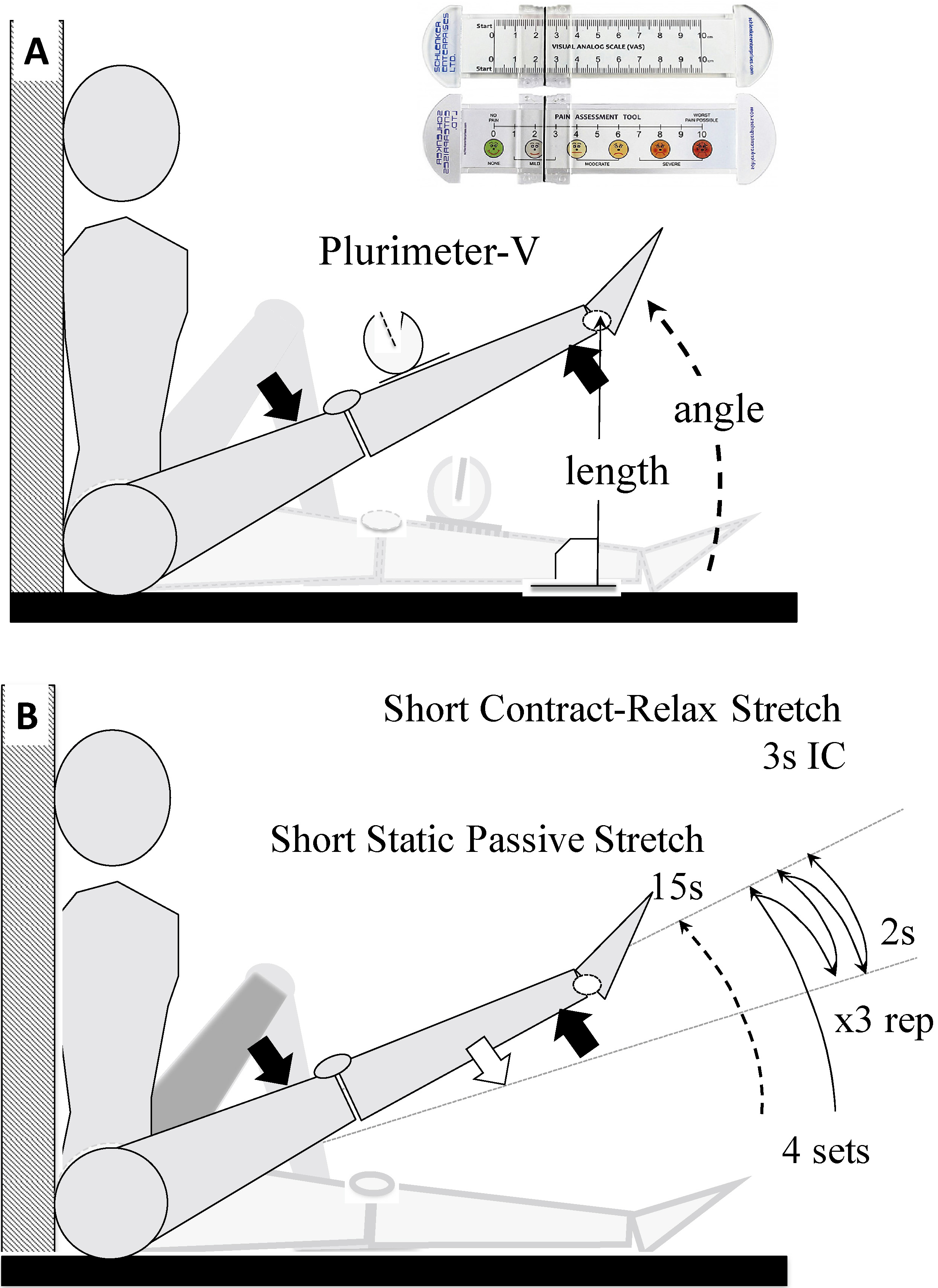
The ROM angle was measured twice with an analogue inclinometer (Plurimeter-V, Dr Rippstein, Zurich, Switzerland), placed 15 cm from the kneecap, on the tibia. The plurimeter was set to 0
After the warm-up, maximal isometric voluntary contraction (MVC) and peak moment (PM) in isokinetic concentric (CON) mode were measured before each stretch protocol and 5 min after completing the stretching manoeuvre. The participants were seated on the dynamometer with the body stabilized by straps around the pelvis, chest, leg and ankle to avoid compensation. Because the strength tests were very simple in terms of neuromuscular coordination, the participants did not require a separate familiarization session. However, during the strength-test preparation time, they carried out one isometric attempt for 2 s while being shown their correspondence with the strength-isometric curve graph generated on a monitor, thus receiving not only verbal but visual feedback information. A 45 s rest was provided after this preliminary attempt, before beginning the measured strength-test. During the test the participants were instructed to keep their arms crossed in front of their chest. Participants were verbally encouraged to give maximal effort during the protocol and they were given visual and positive verbal feedback about the moment-time curve during individual contractions.
Isometric MVC flexion (F-MVC) was measured at 30
Stretch technique dosage regime
The maximal passive hip flexion angle-ROM (stretch test) was evaluated using the SSLR test, and was evaluated prior to (pre-S), immediately after (post-I) and 10 min after (post-10) each stretch protocol. Stretch techniques and use of the dominant or non-dominant leg were randomized for each subject (Fig. 2B). The stretch protocol was performed using the SSS stretch technique and 24 h later performed using the SCR technique with the other leg and in the same position and vice versa. We used similar times under muscular tension, with two stretching techniques: SSS and SCR. The end of ROM was always increased using the same stretch tolerance dose to the point of discomfort (POD) with a VAS. Each stretching period lasted 3 min (1-min stretch-dose plus 2-min rest between sets) as measured with an MD1-003 Digital Stopwatch (Super A Scientific Co., Ltd, Zhejiang, China). A VAS using a 10 cm horizontal line with “no pain” and “worst pain possible” as the anchor points at each end, and a numbered scale from 0 to 10 on the reverse (hidden from the participant), with a clear PVC indicator slider, was used to assess participants’ stretch tolerance in left and right leg ROM tests [26]. The VAS score was collected immediately (
Static passive stretch (SS) technique
From a seated straight leg raise position, the subject’s leg was elevated to a maximal passive hip flexion ROM with the knee straight, from rest to the individual’s POD, and held in this position for a specified period of time with a sustained force. In our protocol, the dose for the SSS was 4 sets
Test-retest relative and absolute reliability in strength and stretch test variables
Test-retest relative and absolute reliability in strength and stretch test variables
Test-retest absolute reliability was measured by the standard error of measurement (SEM), which was expressed in relative terms through the coefficient of variation (CV), whereas relative reliability was assessed by the intraclass correlation coefficients (ICC) at 95% Confidence Interval (CI) calculated with the one-way random effects model. F-MVC and E-MVC: Maximal isometric voluntary contraction in Knee Flexors and Knee Extensors respectively.
From a seated straight leg raise position, the subject’s leg was elevated to a maximal passive hip flexion ROM with the knee straight, from rest to the individual POD. In this position, the participant performed 4 sets of maximal isometric contractions for 3 s, lowering the leg against resistance offered by the examiner, relaxing for 2 s between attempts. Each set, using the SCR, involved 3 contract-relax cycles, and a rest period of 30 seconds was provided between sets (4 sets
Statistical analyses
Values are reported as mean
The chances that the true values for each condition were beneficial/better, unclear or detrimental/worse for performance were calculated. The chances of beneficial/better or detrimental/worse effects were assessed qualitatively as follows:
Results
In this study, the acute effects of short stretches on isometric and isokinetic muscular strength were investigated in 20 participants using SSS and SCR stretch techniques. Table 1 shows the test-retest reliability of the scores. The ICC and CV values show an acceptable reliability in all measures.
In ROM assessment, a correlation in VAS scores was found between pre-S vs post-I (
There was a high correlation between angle and vertical length for estimated ROM in the SSLR test (range between 0.86 and 0.97;
Differences in both static passive and contract-relax short-duration stretch techniques before and after each stretch and strength protocol
Differences in both static passive and contract-relax short-duration stretch techniques before and after each stretch and strength protocol
Intra-group significant differences with respect to pre-test:
The results relating to the percentage decrease in passive resistance to stretch (estimated as ROM changes) and performance variables before and after stretch treatment are shown in Table 2. Intra-group differences were observed. The ROM showed statistically significant differences and increased from pre-S to post-I and post-10 in both SSS and SCR stretch techniques. Statistically significant differences were not found in the changes between post-I and post-10 in any SSS (
Statistically significant differences in pre-post stretch techniques were obtained in the following cases: F-PM, F-PMa and concentric F/E ratio (
The aim of the present study was to examine the acute effects of two different short-duration stretching protocols on the isometric and isokinetic strength of knee flexor and extensor muscles.
In the present study, the final ROM increased by 23.2
Although previous work suggests that the time-course for the decrease in musculo-tendinous stiffness may be dose-dependent for more practical stretching durations of 2 to 8 min [9], in this study, using only 3 minutes of stretching intervention for each technique, the relative magnitude of the decrease in passive resistance to stretch showed no differences between stretch techniques.
Stretch-induced strength loss in F-PM was found to be significant, with a decrease of 3.0
Our findings contrast with studies that used static or contract-relax stretch techniques with similar or more time under tension and found no changes in musculo-tendinous stiffness, and no compromised maximal muscle performance [11, 15, 17]. Possibly the magnitude of change in ROM pre and post an SSS protocol that promotes a stretch-induced and likely trivial concentric strength loss could be due to a minor modification in the material behaviour of the aponeurosis-tendon system, by stress relaxation and/or plastic deformation, creating a more compliant muscle tendon unit or/and central nervous system inhibitory mechanism [34]. The stretch-induced isometric strength loss generated by a short SCR protocol could perhaps be explained more by fatigue due to specific isometric muscular activation. However, the magnitudes of relative changes in F-MVC and F-PM were relatively small in terms of effect size (likely negative and trivial, respectively). In addition, the isometric and isokinetic moment in the SSS protocol and the concentric isokinetic moment in the SCR stretch protocol were unaltered. In this study the acute effect of short stretching (15 s) and intervention (3 min total stretching protocol) on SSS and SCR stretching techniques appears to be a decrease in strength variables. However, the likely trivial effects of the change suggest similarity in the results of this study with others, which found no changes in maximal muscle strength, with similar or more time under tension in both stretch techniques.
It is likely that given the magnitude of the changes, after 10 minutes the stretch-induced isometric strength losses are overcome, as shown in studies of the gastrocnemius medialis muscle [32] and counter-movement height performance [35]. Previous research found that 4
The stretch protocols generated an alteration in angle-moment relationships (length-tension relationships) with a decrease of 8.8
If the F-PMa in both SSS and SCR protocols occurred earlier, a possible explanation could be that the stretching results in a slight rightward shift in the length-tension curve, suggesting that an acute lengthening of the muscle with stretching did occur, so that strength decreased at short muscle lengths and increased at long muscle lengths. This muscle length-dependent effect is consistent with previous work on static stretching [23, 26] and contract-relax stretching [23]. Thus, despite a small stretch-induced strength loss with both stretch protocols there seemed to be an increased extensibility of the musculotendinous unit, which may contribute to reducing the susceptibility to strain injury [38, 39].
However, our results show that the relative change in F/E ratio was significantly reduced by 4.2
These findings suggest that even static stretching and smaller time-stretch interventions may affect the conventional or mixed F/E ratios, as found in previous reports using greater time-doses of static stretch [19, 42]. However, the F-PM reduction is produced at a lower angle in SSS, which decreases the F/E ratio and could be a risk factor for hamstring injuries.
The present study had several methodological limitations. First, there was no control group. Given the small (but significant) changes between both protocols, there was no way to determine whether the changes occurred only because of the stretching protocols. Second, the decrease in musculo-tendinous stiffness was not measured, and was instead estimated indirectly from the decreased peak force and/or increased ROM. A decrease in viscoelastic properties promoted by stretching reduces musculo-tendinous stiffness and hence muscles’ capacity to produce force. It would have been interesting to re-measure the ROM at 15, 20, 25 and 30 minutes post-stretch to outline a precise time-course of the intervention-induced effects. Third, in our study, strength tests were only conducted twice (pre-post) and we did not measure the time to total restoration of baseline values. For the ROM, it would have been very useful to determine the evolution of latency in decrease-retain-increase effects. Fourth, ROM, stretch technique and performance should have been assessed for both legs in each subject, randomizing the dominant leg and the technique to obtain complete information for each subject. Fifth, the testing should have included sprint, squat and/or jump performance tests, to allow a comprehensive analysis of the specific influence of each stretch-dose and technique on realistic athletic performance.
In conclusion, the results of the present study show that both SSS and SCR stretching techniques, with short stretch-time doses, produced an immediate increase in ROM that was retained for at least 10 min. There was also a significant but likely trivial and likely negative loss of strength performance in F-PM and F-MVC with SSS and SCR stretch techniques, respectively. Both techniques slightly but significantly modified the angle-torque relationships but only SSS generated a likely relative effect on conventional isokinetic flexion/extension ratios. A decrease in the performance of isokinetic tests should not necessarily be extrapolated to indicate a decrease in athletic performance, especially when the magnitudes of changes are trivial or likely negative, as shown by a small effect size.
Footnotes
Acknowledgments
No funding was received for this study and there was no conflict of interest. The authors are grateful to Said Ahmaidi and Thierry Weissland for the invitation to use the APERE EA-3300’ Laboratory of UFR des Sciences and STAPS, at Jules Verne University of Picardie (Amiens, France) and for their helpful advice.
Conflict of interest
The authors declare no conflicts of interest.