
Abstract
BACKGROUND:
Dynamic stretching (DS) and ballistic stretching (BS) are similar stretching methods, but the differences between them are unclear.
OBJECTIVE:
To examine the immediate effects of unilateral hamstring DS and BS on straight leg raise (SLR), knee flexion range of motion (KF-ROM), and KF and knee extension maximal isokinetic peak torque (KF-MIPT and KE-MIPT) of the bilateral limbs.
METHODS:
Twelve healthy adult men performed four sets of 2 min each of non-stretching, DS, or BS of the right lower extremity. Bilateral SLR, KF-ROM, KF-MIPT, and KE-MIPT were measured pre- and post-intervention; a three-way (intervention
RESULTS:
The SLR of the stretched limb (
CONCLUSION:
DS and BS had slightly different effects on ROM, and neither affected muscle strength; thus, combining the techniques during warm-up might be helpful.
Introduction
Warming up before exercise is essential for better performance and injury prevention [1]. Among the different techniques for warming up, static stretching (SS) has been particularly popular and has been known to increase the range of motion (ROM) and improve muscle strength [2]. However, recent systematic reviews have indicated that prolonged SS harms exercise performance [3]. In contrast, dynamic stretching (DS), which involves repetitive controlled and voluntary movements without keeping the muscles in the stretched position [4], demonstrated increased ROM without decreasing muscle strength, indicating that it is a suitable warm-up method [5]. Some reasons for this effect include sport-specific similarity [6], increased muscle temperature due to muscle contraction [7], and increased nervous system excitation or antagonist muscle inhibition [8, 9]. However, few previous studies showed that DS does not affect ROM or exercise performance [10, 11]; thus, its effects are still controversial. The reason for this seems to be the ambiguity in the definition of DS. Ballistic stretching (BS) is a stretching method similar to DS, but previous studies have defined it as “dynamic” [12] and “ballistic” [13], and the two are often confused.
DS corresponds to BS in terms of repetitive muscle-stretching movements. However, DS is voluntarily controlled, whereas BS is a passive and uncontrolled movement, and they are different stretching methods that should be distinguished [14]. DS is believed to increase muscle temperature [7], while BS may be advantageous for increasing ROM. Magnusson et al. [15] reported that the mechanism of ROM increase by stretching is mainly due to increased stretch tolerance. Uncontrolled muscle stretching beyond the ROM, as in BS, may affect stretch tolerance because of the greater sensation of the stretch experienced by the participant. Thus, although DS and BS are similar stretching methods, there may be some differences in their underlying mechanisms, and their effects on ROM and muscle strength are expected to be different. However, few reports directly compare the two methods, and many points remain unclear.
Recently, it was reported that stretching affects not only the intervention muscles but also the contralateral limbs or non-local muscles (crossover effect of stretching). Behm et al. [16] examined the reciprocal stretching effects on the upper and lower limbs for 5 min (30 s
Therefore, this study investigated the effects of DS and BS on the ROM and muscle strength of the stretched and contralateral limbs (non-stretched limbs).
Methods
Participants
The participants were 12 healthy adult men (age, 21.2
Design
This study utilized a within-subject randomized crossover study design to investigate the effects of DS and BS on SLR, knee flexion ROM (KF-ROM), knee flexion maximal isokinetic peak torque (KF-MIPT), and knee extension MIPT (KE-MIPT) of the stretched limb and contralateral limb (Fig. 1). Non-stretching (NS), DS, and BS were performed over 3 days. Each test day was 24 h apart, and the order of interventions was randomized.
Summary of study design. ROM: range of motion. MIPT: maximal isokinetic peak torque.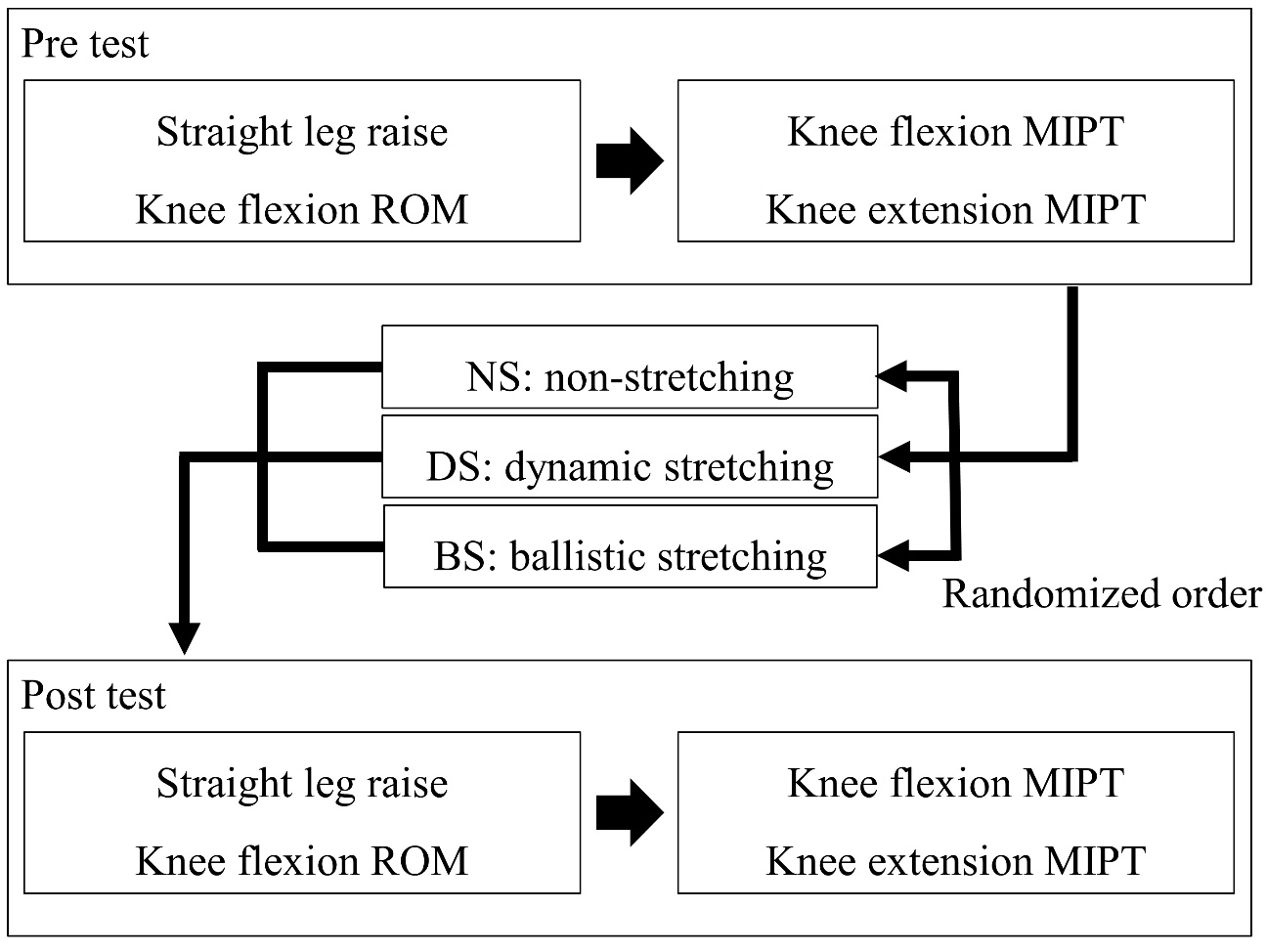
Pre-testing was conducted in the following order: SLR, KF-ROM, KF-MIPT, and KE-MIPT. Thereafter, NS, DS, or BS was performed. The post-test was measured in the same order as the pre-test. In all interventions, post-tests were spaced 30 seconds apart.
Intervention
Figure 2 illustrates all stretching interventions in this study. The examiner instructed the participants to keep the back straight, move the body forward without flexing the knees, and then return to the first position when a 70%–90% discomfort in the hamstrings was felt. BS was performed by one examiner (T.I.) by bouncing hip flexion, and the examiner instructed the participants to keep the back straight and legs relaxed. The stretching duration for both DS and BS was 8 min (2 min
The setup for all stretching interventions in this study. A: Non-Stretching. B: Dynamic stretching. C: Ballistic stretching.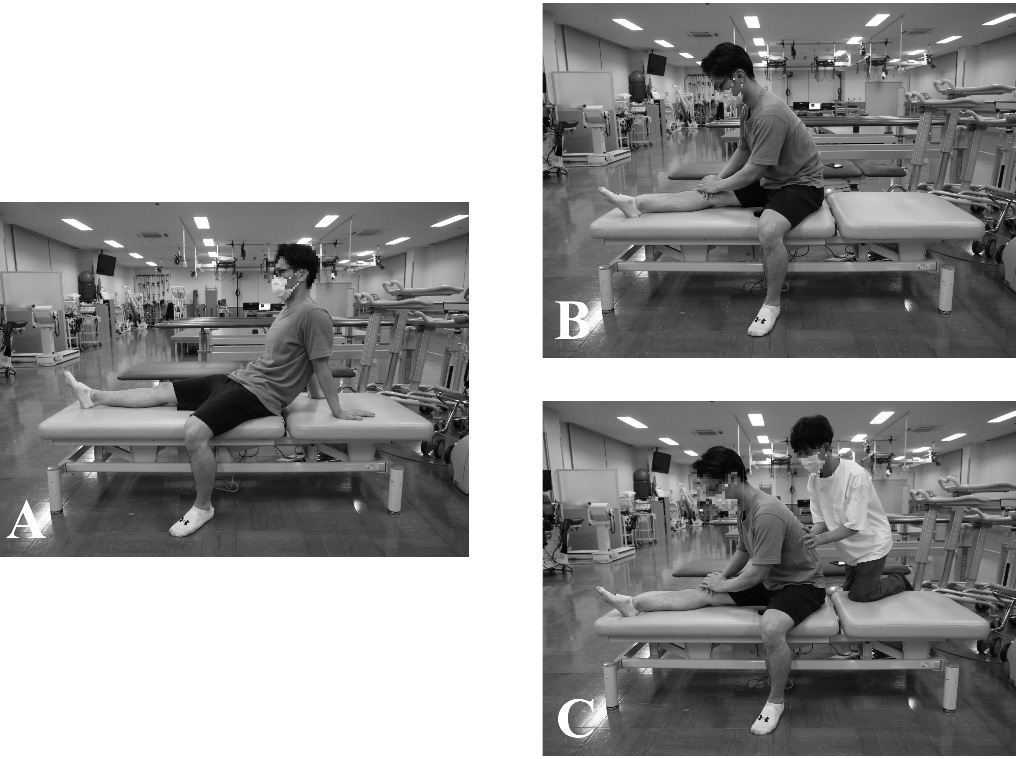
The setup for measuring range of motion and strength in this study. A: Straight leg raise; B: Knee flexion range of motion; C: Knee flexion maximal isokinetic peak torque (MIPT), and knee extension MIPT.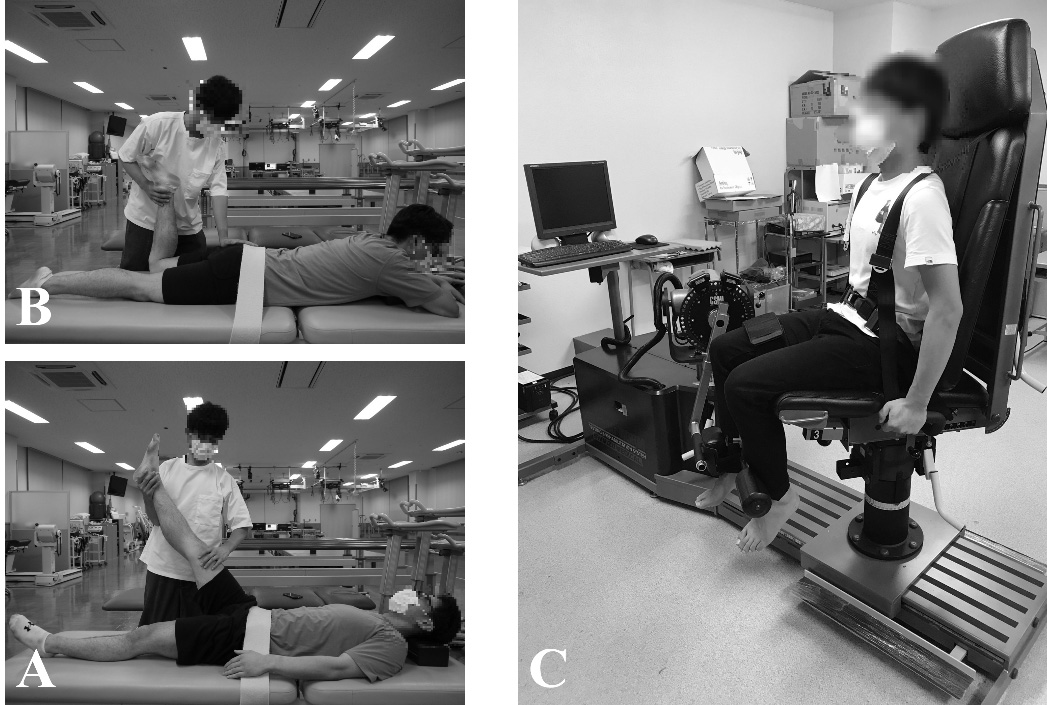
Figure 3A and B illustrate the setup for the ROM measurements in this study. SLR and KF-ROM were measured as stretching of the hamstrings and quadriceps muscles, respectively. The SLR test was performed according to the method of Pedro et al. [19]. The participant was placed in a supine position, and the pelvis was fixed with a Velcro strap placed over the superior anterior iliac spine to avoid posterior pelvic tilt. The examiner aligned the axis of the goniometer with the axis of the hip joint. The fixed arm was aligned with the trunk, and the movable arm was aligned with the femur. The examiner passively flexed the hip joint until the participant reported maximum discomfort (POD) in the hamstring. During the test, the knee joint was held in full extension and the hip joint in an intermediate internal and external rotation position. The ankle joint of the lower extremity was kept in the maximum plantar flexion position to avoid excessive stress due to stretch on the nerve.
KF-ROM was performed according to the procedure by Lin et al. [20]. The participant was placed in the prone position, and the axis of the goniometer was aligned with the center of the lateral femoral epicondyle. The examiner then aligned the fixed arm along the greater trochanter of the femur and aligned the movable arm on the lateral malleolus of the ankle. From there, the participant’s knee joint was flexed until the examiner’s passive movements reported maximum discomfort (POD), and the angle at that time was measured. When the hip joint was flexed along with the knee flexion, the pelvis was fixed with a Velcro strap to avoid compensation by lumbar kyphosis.
Stickers were placed on the anatomical indices that served as landmarks in both SLR and KF-ROM. The angle of the goniometer was recorded in 1
MIPT
The setup for the MIPT measurements is depicted in Fig. 3C. MIPT was measured in the hamstrings and quadriceps using an isokinetic muscle force measurement device (Cybex NORM; Henley Healthcare, Cybex International, Inc., Medway, MA, USA). The angular velocity was set at 60
Statistical analysis
Representative values are presented as mean
Pre- and post-changes in straight leg raise in the stretched and contralateral limbs in three stretching conditions. 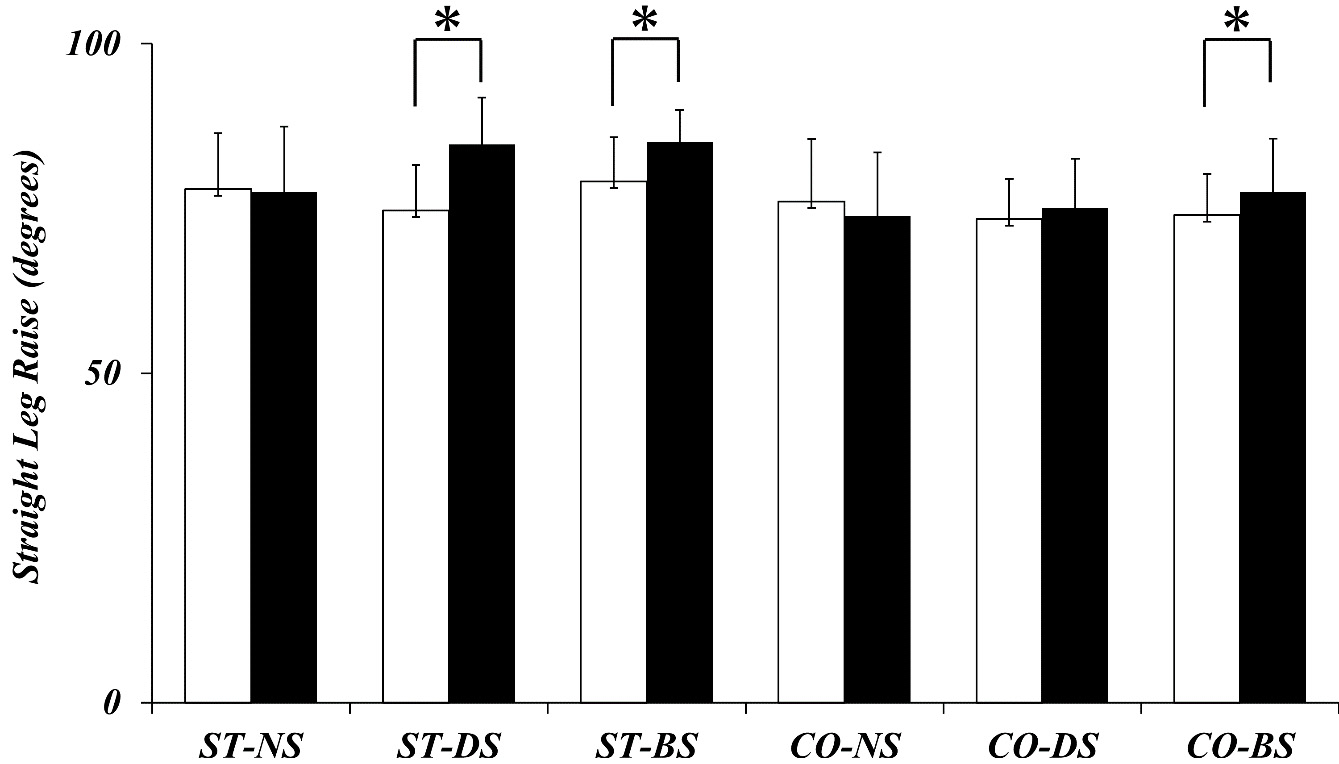
SLR
The results of SLR are shown in Fig. 4. A significant main effect for time [
Pre- and post-changes in knee flexion ROM in the stretched and contralateral limbs in three stretching conditions. 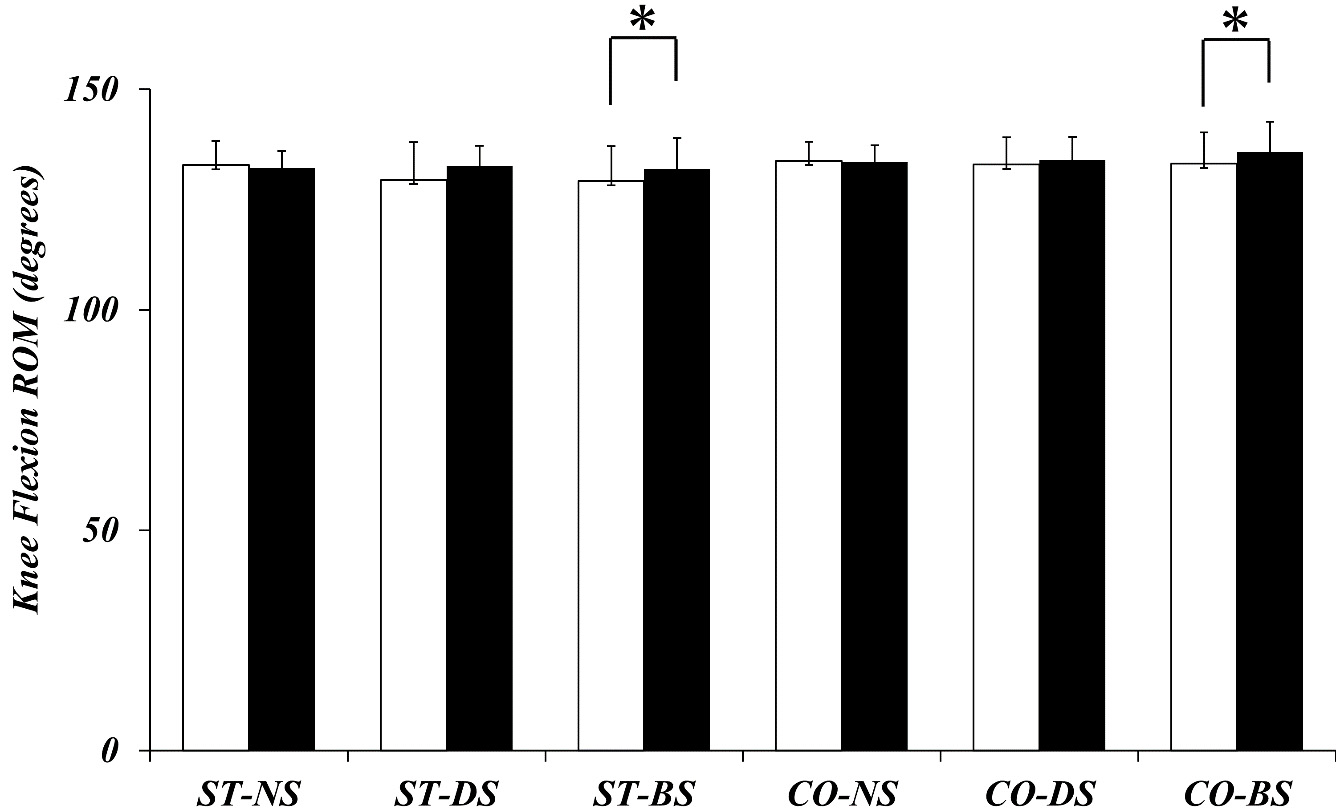
Pre- and post-changes in knee flexion maximal isokinetic peak torque (Nm) in the stretched and contralateral limbs in three stretching conditions
NS: non-stretching. DS: dynamic stretching. BS: ballistic stretching. Nm: newton meter.
Pre- and post-changes in knee extension maximal isokinetic peak torque (Nm) in the stretched and contralateral limbs in three stretching conditions
NS: non-stretching. DS: dynamic stretching. BS: ballistic stretching. Nm: newton meter.
The results for the KF-ROM are shown in Fig. 5. A significant main effect of time [
MIPT
KF-MIPT and KE-MIPT did not show significant main effects or interactions (Tables 1 and 2).
Discussion
This study examined the immediate effects of different unilateral hamstring stretching techniques, specifically DS and BS, on SLR, KF-ROM, KF-MIPT, and KE-MIPT of the stretched and contralateral limbs. The results of this study showed that DS increased the SLR of the stretched limb but did not have a crossover effect on the contralateral limb. However, BS increased SLR and antagonist KF-ROM of the stretched limb and showed a crossover stretching effect that increased SLR and KF-ROM in the contralateral limb. It is also notable that neither DS nor BS caused significant changes in KF-MIPT or KE-MIPT in either the stretched limb or the contralateral limb.
Previous studies have shown that both DS and BS increase ROM [5, 13, 14, 23]. However, only a few studies directly compared the two techniques in terms of their ability to enhance exercise performance. Furthermore, most studies did not focus on the difference between the voluntary component of DS and the passive component of BS. Thus, it was unclear which technique was more effective in increasing ROM. A review by Opplert et al. [14] that summarized the acute effects of DS and BS also indicated the rate of increase in ROM after stretching was 4.46%–9.4% for BS compared with 21.6%–32.2% for DS, suggesting that DS has a greater effect in increasing ROM than BS. This study differs from previous studies in various stretching factors, such as intensity, amplitude, speed, and frequency. Therefore, it is not easy to make a simple comparison. However the current study, with the same intensity based on the POD, saw no significant difference between DS and BS, but the increase in ROM was greater in DS than in BS.
In this study, DS had no crossover effect on the contralateral limb and non-local muscles, whereas BS increased SLR and KF-ROM of the contralateral limb and KF-ROM of the stretched antagonist muscle. Chaouachi et al. [17] reported that unilateral hamstring SS and DS increased SLR without altering the strength and EMG activity of the contralateral limb muscles. Similarly, in this study, neither DS nor BS altered the strength of the contralateral limb. However, the crossover effect of increasing the ROM of the contralateral limb was only observed in BS. Several reasons for this can be postulated considering the results of previous studies. The first could be the different stretching intensities used between DS and BS. In the study by Chaouachi et al. [17], the stretching intensity of DS was set as the “POD,” and the crossover effect of ROM was observed. The present study set the stretching intensity at 70%–90% of the POD, which was lower than that in Chaouachi’s study. Therefore, the results of this study were presumed to be different from that of previous studies even though the same DS technique was used. Additionally, the fact that the crossover effect of ROM was observed only in BS, which involved passive and uncontrolled stretching by the examiner, may be because the subjective intensity of BS was higher than that of DS, which utilized voluntary and controlled stretching by the participant. It has been reported that BS increases muscle tension because it stretches the muscle to a point that exceeds the ROM [24], making it appear as a high-intensity stretching technique. Additionally, several previous studies showed that a higher intensity of stretching was more effective in increasing ROM [25, 26, 27]. Therefore, the increase in ROM by stretching may depend on the intensity. Although there is a difference between this and previous studies regarding the increase in ROM of the contralateral limb, the difference in stretching intensity may be responsible for the crossover effect in this study. Second, it was inferred that there was an improved tolerance to stretching. The mechanism of increased ROM is linked to a decrease in stiffness of the muscle-tendon unit and an increase in tolerance to stretching, i.e., the so-called stretch tolerance [14]. The increase in ROM in the non-stretching area seems to be primarily due to stretch tolerance since no direct stretch stimulus was applied [16, 17, 18]. Since BS is a passive and uncontrolled stretch, the stretching sensation experienced by the participants was more intense, and stretch tolerance may have been involved. Therefore, it could be possible that the crossover effects of increased ROM in the contralateral limb and stretched limb antagonist muscles were observed only in BS because of the differences in the effects of stretch intensity and tolerance.
No significant changes in KF-MIPT and KE-MIPT were observed in both the stretched and contralateral limb during either DS or BS. The result that DS does not change the muscle strength of the stretched limb is consistent with a systematic review [5]. However, the effect of BS on performance is still controversial. In the review by Opplert et al, it was suggested that BS might harm performance because passive and uncontrolled movements generate a large amount of tension in the muscle [14]. Conversely, it seems the accumulation of muscle tension by BS may help improve muscle strength by releasing elastic energy during subsequent voluntary movements [28]. Although it is impossible to mention the effect of BS on muscle strength and its mechanism in this study, BS set at an intensity of 70%–90% of the POD did not change the muscle strength. During warm-ups in sports, it is also important to consider whether stretching affects the muscle strength of non-stretched muscles. As in previous studies [16, 17], no change in muscle strength was observed in the contralateral limb for both DS and BS in this study. Therefore, it is suggested that both DS and BS may be used as stretching methods that satisfy the conditions suitable for warm-up without affecting the muscle strength of both the stretched contralateral limbs.
The clinical implication of this study is that both DS and BS at 70%–90% intensity of the POD to the hamstrings proved viable as warm-up methods because they increased ROM without decreasing the strength of the stretching muscles. DS may have a slight advantage over BS in increasing the ROM of the stretching muscles, although there is room for further investigation in additional studies. BS is a beneficial warm-up in that it acts on the ROM of a broader range of muscles, increasing the ROM of the stretching and antagonist muscles and the contralateral limb. Therefore, DS and BS may have different effects, and the combination of these techniques may be desirable in rehabilitation and sports clinical practice.
There are some limitations to this study. First, this study did not measure any aspect of the mechanism of stretching. Therefore, any discussion of the mechanism is speculative and uncertain. This point requires careful cross-checking with previous studies and verification by additional studies. Second, the crossover effect of BS may be too small to be considered a significant effect. A previous review estimated that a change of more than 6
Conclusion
This study demonstrated that DS and BS have different effects on the stretched and contralateral limbs. DS of the unilateral hamstrings increased the SLR of the stretching limb. In contrast, BS increased not only the SLR of the stretching limb but also the KF-ROM of the stretching limb and the SLR and KF-ROM of the contralateral limb, indicating a crossover effect spilled over to the non-stretching muscles. It was also found that neither DS nor BS affected the strength of the stretching and non-stretching muscles. The results of this study suggest that both DS and BS are practical warm-up techniques to increase ROM without decreasing muscle strength and that they may have different effects with different characteristics.
Author contributions
CONCEPTION: Taisei Inoue and Katsuhito Nagano.
PERFORMANCE OF WORK: Taisei Inoue.
INTERPRETATION OR ANALYSIS OF DATA: Taisei Inoue and Katsuhito Nagano.
PREPARATION OF THE MANUSCRIPT: Taisei Inoue.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Katsuhito Nagano.
SUPERVISION: Katsuhito Nagano.
Ethical considerations
This study was approved by the Ethical Review Committee of Nittazuka Medical Welfare Center (approval no: Nittazuka Ethics 2019-59). Written informed consent was obtained from all participants.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors would like to thank Fukui Health Science University for providing the research environment and Dr. Hideaki Matsuo and Dr. Hiroaki Naruse of the University of Fukui Hospital for their efforts in the critical revision of this study.
Conflict of interest
The authors have no conflicts of interest to report.