
Abstract
BACKGROUND:
Interventions using Pilates and whole body vibration (WBV) have been conducted in postmenopausal women, aimed at increasing muscular strength and quality of life; however, some results are contradictory.
OBJECTIVE:
To compare the effects of Pilates vs. WBV on isokinetic muscle strength and quality of life in postmenopausal women.
METHODS:
Fifty-one (51) women were randomly assigned to the following groups, Pilates (
RESULTS:
96.1% of participants completed the follow-up. The Pilates was superior (
CONCLUSIONS:
Pilates is an alternative intervention superior to WBV when the goal is linked to the strength of the knee flexor muscles.
Introduction
Women experience hormonal alterations in the postmenopausal period due to the rapid decline in estrogen levels [1]. In this period, the ovulatory cycle ceases, coinciding with important physiological alterations typical of the aging process [2], which potentiates the appearance of negative effects on health, such as a decrease in muscular strength [3] and impaired quality of life [4].
Among the ways to mitigate or reverse these factors, we highlight the regular and systematic practice of physical exercises [5]. An emerging exercise option that has been investigated in relation to its benefits for postmenopausal women is the Pilates exercise [6, 7]. This technique works through progressive muscular endurance exercises and has been shown to be effective for increasing muscular strength [8, 9, 10, 11, 12, 13, 14, 15] and improving quality of life in older women [7, 15, 16, 17]. A meta-analysis study of the effects of Pilates on different health outcomes in older adults, identified that the method promotes significant improvement in muscular strength and quality of life [18]. However, other studies have shown that Pilates may not increase muscular strength [19] or contribute to improvement in different domains of quality of life in older adults [20]. These conflicting data may be related to the duration of intervention [19], or the absence of a control group [20], which compromises the level of evidence.
Another technique that has demonstrated different benefits for health outcomes in women during the postmenopausal period is whole body vibration (WBV) [21, 22]. Studies have shown that WBV may increased muscular strength [23, 24, 25] and improved quality of life in older adults [26, 27], however, some studies did not observe benefits of this technique on muscular strength [28, 29] or quality of life [30]. A systematic review and meta-analysis [22] concluded that WBV provides significant effects on dynamic knee extension strength and isometric leg extension strength in older adults when compared to no intervention but no differences when compared to other physical exercise modalities. However, WBV did not increase isometric knee extension strength when compared to no intervention or other forms of exercise [22].
Unlike conventional modalities of physical exercise, in WBV the individual remains standing on an oscillatory plate, which transmits mechanical vibrations throughout the body [31]. Several studies have compared WBV with different forms of physical exercise interventions on variables related to muscular strength [25, 32, 33, 34, 35]. In the majority of these studies, WBV was not found to be significantly different from conventional exercises that provide muscular strengthening when taking into consideration the peak isokinetic torque of knee extensors [25, 32, 35], and may be more effective in increasing the strength of the ankle flexors [34], or less effective when considering the strength of the upper limbs [33].
A controversy in the interventions involving WBV is the different parameters that can be used to modify the intensity of the vibrations, such as frequency, magnitude, and time of exposure [31]. Furthermore, the majority of studies performed up to now have prescribed strengthening exercises for the lower limbs during WBV [24, 25, 33, 34, 35, 36, 37], which raises doubts as to whether the effects on muscular strength were due to the mechanical vibrations or performance of muscular strengthening exercises. In addition, the low quality of evidence limits confidence in reported observations.
No studies have been found that compared Pilates and WBV, and there are few studies of good methodological quality that compare these modalities with no intervention. Therefore, the objective of this study was to examine the effects of six months of Pilates exercise compared to WBV and no treatment controls on the peak isokinetic torque of the extensor and flexor muscles of the knee in postmenopausal women. As a secondary objective, we sought to identify the effects of the techniques on the quality of life of this population.
Method
This study was a randomized controlled clinical trial (registered at www.clinicaltrials.gov on May 7, 2016: NCT02769143), which followed the CONSORT recommendations. The intervention lasted six months and involved 51 postmenopausal women (who had experienced menopause for at least one year), subdivided into three equally sized groups. All the participants were able to practice physical exercise, were aged between 40 and 70 years, and lived in the city of Jacarezinho, state of Paraná, Brazil. The present study followed the ethical norms established by the Declaration of Helsinki (1975, revised in 1983) and was approved by the Human Ethics Committee of the Northern University of Paraná, Brazil (opinion 1,032,182). All participants signed a Free and Informed Consent Term.
Recruitment and participants
Participants were recruited in May 2016 through posters made available in public places, newspaper adverts, the radio, internet news sites, and leaflets left in medical clinics and health facilities, all with local coverage. The sample calculation was performed in the Bioestat 5.3 program (Mamirauá Institute, Amazonas, Brazil), taking into account the values of isokinetic muscle strength (Nm.) of the knee extensors, at the angular velocity of 60
The inclusion criteria were a) post-menopausal, clinically confirmed, for at least 12 months; b) not practicing physical exercise for at least six months; c) agreement not to practice another type of exercise during the research; d) ability to perform activities of daily living without assistance [38, 39]; e) presentation of a medical release indicating fitness for exercise; and f) score
The exclusion criteria were a) musculoskeletal dysfunctions in the spine or lower limbs in the previous six months; b) fracture in the vertebral column or in the lower limbs after 40 years of age; c) prosthesis in the lower limbs or implants in the vertebral column; d) secondary causes of loss of bone mass; e) other metabolic bone diseases or diseases that affect bone metabolism; f) history of cancer in the previous five years; g) vascular alterations, epilepsy, or seizures; h) arrhythmia; i) the use of a pacemaker; j) eye disease affecting the retina; k) cardiorespiratory diseases; l) diseases of the neuromuscular system; m) labyrinthitis or vertigo; n) hospitalization in the previous six months for surgical reasons; o) thyroid alteration; p) smoking; q) frequent use of alcoholic beverages; r) use of supplements based on calcium or vitamin D, isoflavone, medication to increase bone mineral density or to increase muscle mass in the previous 12 months; and s) inability to tolerate WBV for five minutes.
All participants included in the present study were instructed to maintain their usual routines, as well as their daily physical activities (e.g., domestic duties, paid work) and nutritional habits. They were also instructed not to take any medication or supplement that could influence muscle mass or bone mass.
Evaluation of muscular strength
To evaluate the muscular strength of the knee extensors and flexors, an isokinetic dynamometer (Biodex System 4.0, Biodex Medical Systems, Shirley, NY, USA) was used. All procedures were performed by an independent evaluator, not directly involved in the research project, experienced in isokinetic evaluations, and blind in relation to the allocation of participants in each group. The equipment was calibrated prior to the test according to the manufacturer’s standards. Preceding the test, the participants performed a five-minute warm-up on a vertical exercise bike, using a light load (25 watts) and comfortable speed (50 rotations per minute). Subsequently, the evaluator positioned the participant in the equipment, with the hip joint making an angle of 120
The axis of rotation of the dynamometer arm was aligned with the lateral epicondyle of the femur of the dominant lower limb. The site of force application was positioned approximately two centimeters from the medial malleolus. Belts were attached to the trunk, pelvis and thigh to avoid compensatory movements [41]. After brief familiarization with the equipment and range of motion, the participants performed the knee extension and flexion movements (concentric/concentric) at the angular velocity of 60 degrees per second (60
Evaluation of quality of life
To evaluate the quality of life, the Brazilian version of the SF-36 questionnaire was used [43]. This questionnaire consists of 11 questions and 36 items, subdivided into eight components (domains), represented by physical functioning (10 items), role-physical (four items), bodily pain (two items), general health (five items), vitality (four items), social functioning (two items), role-emotional (three items) and mental health (five items). The first four domains assess physical health, while the last four assess mental health. Participants receive a score for each domain, ranging from 0 to 100, with 0 being the worst score and 100 being the best [44]. The questionnaire was applied by an evaluator not directly involved with the study and blinded in relation to the allocation of the participants in each group.
Pilates exercise – Protocol 1 and 2
Pilates exercise – Protocol 1 and 2
After the evaluation of muscular strength and quality of life, participants were randomized to three groups by a researcher who was not part of the study team. The random numbers were generated by software (randomization.com), which distributed the participants to either Pilates group (PG), Vibration group (VG) or Control group (CG), with 17 participants in each. The researcher who performed the randomization sealed the opaque envelopes containing group allocation details and gave them to the principal investigator who was blind to group allocation. The participants, in a blinded manner, individually received the envelopes containing their name. After breaking the envelope seal, the participant and principal investigator checked group allocation.
Intervention
The interventions occurred three times a week, on nonconsecutive days, for six months (78 sessions), starting in June 2016, in a private clinic located in the city of Jacarezinho, Paraná, Brazil. The experimental groups (PG and VG) were supervised by two professionals with experience in Pilates and WBV. As the intervention included physical exercise, it was not possible to blind the participants or the professionals responsible for the interventions.
Pilates group
The first session of the PG was used to familiarize the participants with the technique, providing an explanation of the correct execution of each movement and the principles of the method. The following equipment was used to perform the exercises: Cadillac, Reformer, Ladder Barrel, Wall Unit, Chair, Spine Corrector and Small Barrel (ISP, Cascavel, PR, Brazil). Twenty-one strengthening and stretching exercises were selected for the main body segments: a) lower limbs b) flexors, extensors, and lateral flexors of the trunk; and c) upper limbs. Two exercise protocols were applied during the six months of intervention, each performed for three months (Table 1), maintaining the same sequence of strengthening and stretching, as well as the same body segments but changing the order of equipment. Each session lasted 60 minutes.
Flow diagram (CONSORT) throughout the course of the study. Abbreviation: ITT, Intention-to-treat.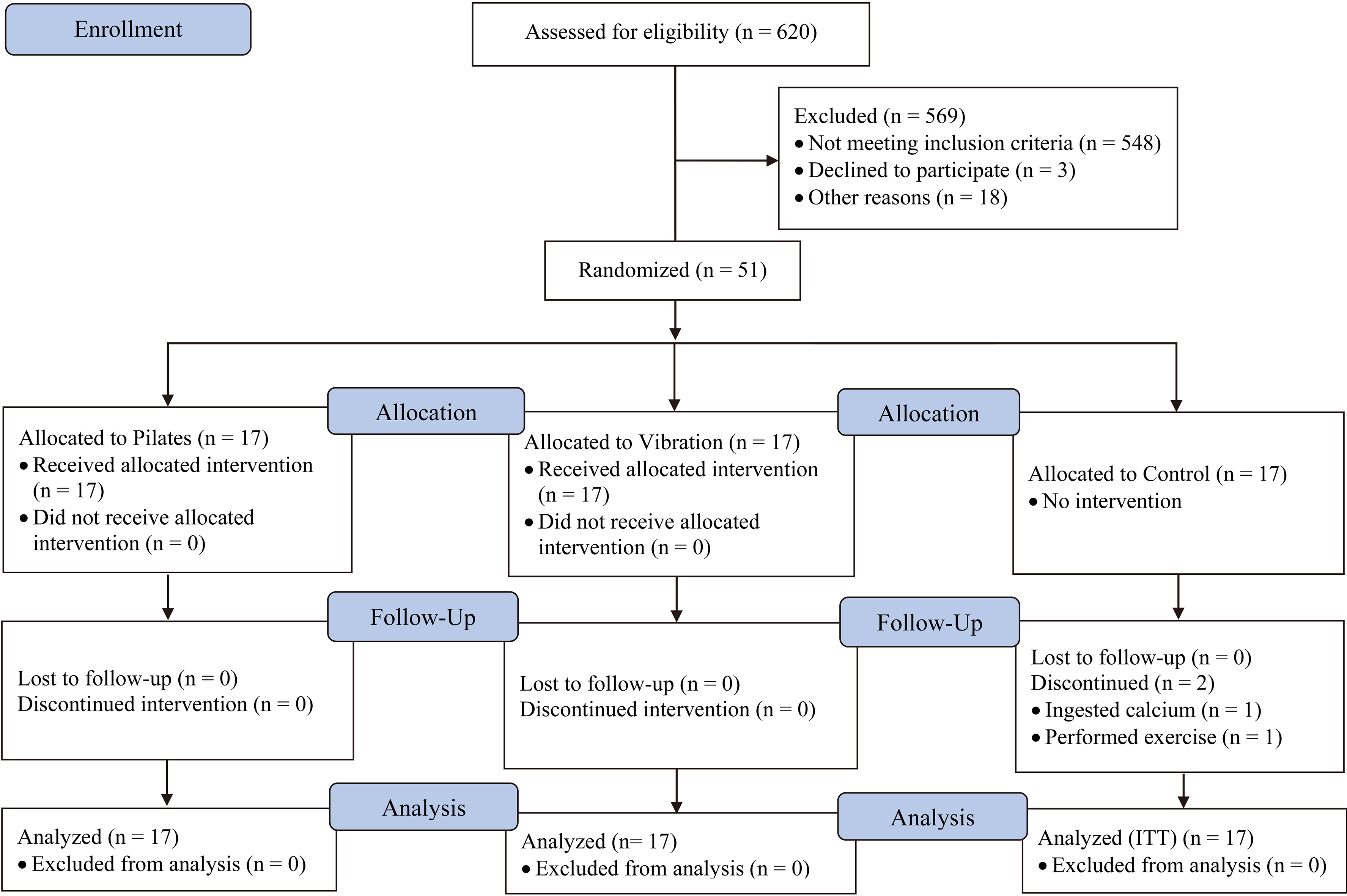
All exercises were performed in a series of ten repetitions, with a one-minute rest interval between exercises. The intensity of the overload in Pilates is mainly determined by the use of springs, which were modified according to the evolution of strength of each participant (changing the position of the springs in the equipment or changing the spring to another one of greater resistance) [45], always maintaining the number of repetitions and series. To determine the level of effort of the participants and the consequent evolution of the overload, a verbal description according to the Borg CR10 scale was used: light load (Borg
The VG was exposed to WBV for five minutes on a side-alternating type vibratory platform (Arktus, Cascavel, PR, Brazil), which oscillates through an anteroposterior axis, causing the right and left sides to alternate horizontally. A frequency of 20 Hz (1 Hz
Exposure time was 5 minutes because the side-alternating platform generates a large amplitude peak-to-peak displacement, which does not allow prolonged exposure. Other studies that used an side-alternating platform to identify effects on muscle strength also uses similar of low exposure times [26, 28, 29, 34].
Control group
The CG did not perform any type of intervention. The researcher responsible for the study contacted the CG participants every month during the intervention to emphasize the importance of maintaining their usual routine related to physical activity, eating habits, the importance of not using supplements or medications that could affect bone or muscle mass, and not starting any type of physical exercise, according to the procedure also adopted with the PG and VG. At this time, the participants were also questioned about possible adverse events.
Baseline characteristics of participants
Baseline characteristics of participants
Abbreviations: SD, standard deviation; IQR, interquartile range (25
A standardized form was used to record occurrences of adverse events in all three groups. Participants were asked every month about any complications such as spasms or muscle pains, joint pains, dizziness, falls, cramps, and changes in blood pressure.
Between group comparisons for isokinetic muscular strength (in Nm) between baseline and follow-up
Between group comparisons for isokinetic muscular strength (in Nm) between baseline and follow-up
Outcome values at each time point are mean (standard deviation).
Comparisons of pairs for isokinetic muscular strength (in Nm)
Abbreviations: SD, standard deviation; 95% CI, 95% confidence interval.
Between-group comparisons for quality of life (SF-36 score), between baseline and follow-up
Outcome values at each time point are median (interquartile range, 25
Parametric data are presented as mean and standard deviation (SD), and non-parametric data as median and the respective interquartile range (25
Results
Participation
Initially 620 women were interviewed. After applying inclusion/exclusion criteria, 51 volunteers were eligible to participate (17 in each group). Of the 51 participants initially randomized, 49 (96.1%) completed the follow-up. Two CG participants dropped out of the study (one started exercising and the other took calcium-based supplementation) (Fig. 1). There were 78 intervention sessions over the 6 months of the study. The number of participants’ absences did not differ significantly between the experimental groups (
Baseline characteristics
Table 2 presents the baseline characteristics of the participants. Age, anthropometric variables, time in menopause, and SF-36 domains were similar in all three groups (
Muscular strength
Table 3 presents the results of isokinetic muscular strength of knee extensors and flexors at 60
Comparisons of pairs for quality of life (SF-36 score)
Comparisons of pairs for quality of life (SF-36 score)
Abbreviations: IQR, interquartile range (25
Table 5 presents the results of the quality of life comparisons as measured by the SF-36 questionnaire between groups. The PG was significantly (
Adverse events
Serious adverse events were reported in all three groups: two falls in the PG, two in the VG and one fall in the CG (that led to a fractured wrist for CG participant). All falls occurred outside exercise sessions. Reports of pain occurred mainly in the PG and VG. The primary complaint reported by participants was delayed onset muscle soreness, reported by the PG (100%) and VG (58.8%), principally in the first weeks of the intervention. Other less serious adverse events, such as pain in specific regions of the body, muscle spasms, and cramps occurred less frequently (Table 7).
Summary of adverse events
Summary of adverse events
Summary of the main results
This study aimed to examine the effects of Pilates exercise and WBV on the isokinetic muscular strength of knee extensors and flexors and quality of life in postmenopausal women. After six months of intervention, Pilates was superior (
Muscular strength
In agreement with the findings of the present study, others have identified significant improvement in lower limb muscular strength when comparing Pilates exercise in older women to control comparisons who received no treatment [9, 13, 14] or minimal intervention (stretching) [8, 15]. Oliveira et al. [8] evaluated the peak isokinetic torque of knee extensors and flexors at 60
In addition, a meta-analysis that grouped the different studies that applied the Pilates exercise as a form of intervention, identified that compared to control outcomes, the technique is associated with a large effect size (
Our results indicate that WBV was not effective in increasing the peak isokinetic torque of knee extensors and flexors in comparison with the control group, corroborating reports of investigations into the effects of this technique in postmenopausal women. Liphardt et al. [28] used WBV on a side-alternating platform at 20 Hz, peak-to-peak amplitude of 3 to 4 mm, with participants standing with knee flexion of 30
However, studies that have administered WBV associated with lower limb muscle strengthening exercises (such as squats during WBV) have identified significant improvement in lower limb muscle strength in postmenopausal women, when compared to relaxation exercises [24] or no treatment [25]. Von Stengel et al. [24] using synchronous vibration (35 Hz, peak to peak amplitude of 1.7 mm) and side-alternating vibration (12.5 Hz, peak to peak amplitude of 12 mm), with an exposure time of 15 minutes, found that, after 12 weeks of intervention, both types of vibration allows a significant improvement in isometric muscular strength of the knee extensors at 100
A meta-analysis concluded that WBV compared to no intervention provides significant effects on dynamic knee extension strength and isometric leg extension strength in older adults but no differences when compared to other physical exercise modalities. In addition, WBV did not increase isometric knee extension strength when compared to no intervention or other forms of exercise [22]. However, the authors did not perform subgroup analyzes considering in isolation studies that performed muscular strengthening exercises during WBV, or for different frequencies, magnitudes, types of vibration, or time of exposure. Meta-analysis studies should strive to perform subgroup analyzes in which studies with different interventionsare considered separately, thus making it possible to identify the source of effects identified in the analysis.
The performance of dynamic exercises during WBV is likely to be an important moderating variable for gaining muscular strength. Another meta-analysis study involving different populations concluded that in WBV interventions in which participants perform dynamic and isometric muscle contractions, muscular strength gain is almost double compared to interventions using isometric contraction alone (such as remaining in a semi-flexed knee position) [48]. It was also concluded that synchronous platforms were more effective for gaining muscular strength when compared to side-alternating type platforms [48], which may explain the lack of significant results for WBV in the present study.
In the current study, when comparing WBV and Pilates, a significant difference (
The present study did not find significant differences between WBV and Pilates for the peak isokinetic torque of the knee extensors at 60
Interventions involving WBV use low exposure time, while in the different forms of physical exercise the interventions have significantly longer duration. Thus, the differences between WBV and Pilates for the peak isokinetic torque of knee extensors presented in the present study may have occurred as a result of the difference in exposure time of five and 60 minutes respectively.
Quality of life
Regarding quality of life, the PG was superior to the CG for four domains (role-physical, bodily pain, social functioning and role-emotional) of the SF-36 questionnaire. Pilates exercise appeared efficient for improving quality of life in components related to physical health and mental health. Other studies that used the same questionnaire in postmenopausal women found, after 12 weeks of Pilates,significant effects on the quality of life in favor of Pilates when compared to stretching exercises [15] and exercises performed at home, without professional supervision [16]. Campos de Oliveira et al. [15] observed improvement for six domains of the questionnaire, while Küçükçakır et al. [16] reported improvement for all eight domains.
Studies that used other questionnaire models to assess quality of life also identified significant improvements after Pilates compared to no treatment controls [7, 17]. Angın et al. [7] found improvement for all domains of the QUALEFFO-41 questionnaire in postmenopausal women after six months of Pilates. Siqueira Rodrigues et al. [17] after 8 weeks of intervention with the method, reported an improvement in the overall quality of life index, measured by the WHOQOL-OLD questionnaire, in older women. In addition, a meta-analysis, summarizing the results of different studies of Pilates on the quality of life in older adults, concluded that the technique was associated with a large effect size (
No significant differences between VG and CG were found in SF-36 scores. Few studies to date have observed the effects of WBV on quality of life in older adults. Bruyere et al. [27] compared two groups that participated in conventional physiotherapy and one of these groups complemented the intervention with WBV and found imporvements in all SF-36 domains for the WBV group. On the other hand, Santin-Medeiros et al. [30] after 8 months of WBV, did not observe differences for any SF-36 domain compared to no treatment controls.
In the present study, there were no significant differences in the comparisons between WBV and Pilates for the domains of quality of life measured by the SF-36. Given that few studies to date have observed the effects of WBV on the quality of life of postmenopausal women, and that no study has compared the technique with another form of physical exercise, further validation studies should be performed. The Pilates sessions lasted approximately 60 minutes, while the WBV sessions lasted only five minutes. Consequently, Pilates allowed greater social interaction among participants, which may explain the results of the present study for quality of life only of the Pilates group compared to the control group, but not for vibration compared to control.
Strengths and limitations
This was the first study to identify the effects of Pilates compared to WBV on muscular strength and quality of life in postmenopausal women. To our knowledge, this was also the first study to investigate the effects of WBV on the peak isokinetic torque of the knee flexors in postmenopausal women. Another strong point is the adherence of the participants to the intervention, with loss of only two volunteers from the control group, as well as the attendance frequency rate in the two intervention groups that was higher than 90%. As limitation, since the study included an intervention involving physical exercise, it was not possible to mask the participants and the professionals who ministered the interventions.
Conclusion
Six months of Pilates three times per week was superior to WBV for the peak isokinetic torque of knee flexors in postmenopausal women, while no difference between techniques was observed for the peak isokinetic torque of knee extensors or quality of life. Pilates was superior to no intervention in the variables of peak isokinetic torque of knee extensors and flexors, and for four of the eight domains of the SF-36 questionnaire. WBV was not significantly different to no intervention for these same variables.
Footnotes
Conflict of interest
There is no conflict of interest.