
Abstract
Objective
Existing isokinetic contractions are characterized using standardized angular velocities, which can induce differing adaptations. Here, we characterized the variation in the isokinetic parameters of knee extensors according to individualized angular velocity (IAV).
Methods
We performed a cross-sectional study of 19 young, healthy men. We measured the maximum angular velocity (MAV) of concentric knee extension using the isotonic mode of an isokinetic dynamometer. Isometric and isokinetic (at angular velocities corresponding to 100%, 70%, 40%, and 10% of each individual’s MAV) knee extensor contractions were performed, and the peak torque and mean power were recorded.
Results
Peak torque significantly decreased with increasing IAV (129.42 ± 25.04, 84.37 ± 20.97, and 56.42 ± 16.18 Nm at 40%, 70%, and 100%, respectively), except for isometric contraction (233.36 ± 47.85) and at 10% of MAV (208 ± 48.55). At the mean power, 10% of MAV (74.52 ± 20.84 W) was significantly lower than the faster IAV (176.32 ± 49.64, 161.53 ± 56.55, and 145.95 ± 50.64 W at 40%, 70%, and 100%, respectively), and 100% was significantly lower than 40%.
Conclusion
The optimized IAV for isokinetic contraction to improve power output while maintaining torque is 10% to 40% of MAV. IAV may reflect both the velocity and force components of power because individuals do not have the same angular velocity.
Keywords
Introduction
Muscular strength, which represents the ability to apply force to external objects or counter resistance, is an essential component of physical fitness and is necessary when performing various activities of daily living.1–4 Resistance training is a common exercise intervention that aims to improve muscle strength. 5 Maximizing the effectiveness of resistance training involves the manipulation of training variables such as the numbers of repetitions and sets, interval period and intensity, and movement velocity. 6 The type of muscle contraction (isometric, isotonic, or isokinetic) used in training also influences the training effect.7,8
Training using the isokinetic contraction of muscles is a relatively recently developed method, compared with the other types of contraction. 7 Isokinetic contractions can develop maximal tension over the full range of motion. The angular velocity of joint movement can be controlled or monitored using an isokinetic dynamometer7–11 in addition to their use in training and rehabilitation. The evaluation of isokinetic parameters, such as torque and power, is considered to be the gold-standard method of evaluating muscle strength because of its high levels of reliability and validity.12–15 Knee extensors are among the most frequently investigated muscles using a dynamometer. 16 Knee extensors are not only convenient for the assessment of muscle function using a dynamometer, but are also important for daily tasks and representative of total limb or total lower limb strength.2,16,17
The development of isokinetic dynamometers has facilitated a considerable number of studies regarding muscle characteristics.18,19 However, although they are frequently used for testing, relatively few practitioners use them for training or rehabilitation. However, in the fields of rehabilitation and sports, isokinetic contractions may have potential advantages over other types of contractions, such as angular velocity control and force–curve matching.11,12 An isokinetic dynamometer provides force–velocity and power–velocity relationships tested across a range of velocities, and these vary according to the neuromuscular characteristics of individuals.11,20,21 An individualized training program based on individual force–velocity relationships has recently been reported to be more effective at improving jump performance than a conventional resistance training program that is common to all individuals, regardless of their force–velocity profiles. 21 In addition, the intensity setting for resistance training is conventionally determined according to the individual’s maximum intensity and their ability,3,5,22 and this permits individualized intensity settings to be used for training.
Tailoring exercise regimens to individual abilities and characteristics has been a long-standing principle of exercise. Nevertheless, several previous isokinetic studies have used only one-size-fits-all specific angular velocities, such as 60°/s, 90°/s, 180°/s, and 240°/s, for all the participants during the investigation of force–velocity relationships, training effects, and muscle strength.23–29 This is probably because the use of one-size-fits-all specific angular velocities makes it easier to assess large numbers of participants, allows direct comparisons between groups, and allows pre- and post-intervention analyses to be performed, without altering many variables. However, as for intensity, the maximum angular velocity (MAV) produced by a joint may vary considerably between individuals. Specifically, the standardized angular velocities (SAVs) commonly used in isokinetic contractions may correspond to fast angular velocities for some people and slow angular velocities for others. In other words, the use of SAVs likely induces differing adaptations, depending on the neuromuscular characteristics of individuals. Therefore, in the present study, we aimed to investigate the variation in the isokinetic parameters (torque and power) of knee extensors according to the individualized angular velocity (IAV) during isokinetic contraction. We hypothesized that the torque and power of the knee extensors might be influenced by differences in IAV.
Methods
The reporting of this study conforms to the STROBE guidelines. 30
Ethics approval
The study was approved by the Sunmoon University Institutional Review Board, Republic of Korea (approval number SM-202104-039-1) and conformed to the principles of the Declaration of Helsinki. After being informed regarding the experimental procedures, all the participants provided their written informed consent. All the participant details were de-identified prior to publication.
Participants
We performed a cross-sectional study of healthy young men aged between 21 and 30 years. Recruitment began in June 2021 and data collection ended in December 2021. The participants were recruited through printed and electronic advertisements on noticeboards in the university. The inclusion criteria were required to be physically active, but not participating in a specific lower limb training program. The exclusion criteria were as follows: a history of lower extremity surgery or trauma, knee pain, edema, limitation in the range of motion, or inflammatory disease. The required sample size was calculated using G-Power v.3.1.9.7 software (Heinrich Heine University, Düsseldorf, Germany) and was based on a previous study that measured decreases in torque with increasing angular velocity during knee extension, assessed using SAV, with isokinetic contraction (α = 0.05, power (1−β-error) = 0.95, r = 0.5, effect size η2 = 0.30). 31 This indicated that a sample size of eight was required. However, to allow for dropouts and increase the power of the study, we recruited some additional participants. Ultimately, 19 young, healthy men participated and the data obtained from all the participants were analyzed (Table 1).
General characteristics of the participants.

Data are presented as mean ± standard deviation.
Procedures
The participants were asked to visit the laboratory twice. At their first visit, the participants underwent an isometric test, and at the second visit, they underwent isokinetic testing according to IAV. All the participants’ second visits were approximately 48 hours after their first visits. A flow chart of the experimental procedure is presented in Figure 1.

Flow chart describing the study protocol.
Isometric and isokinetic testing
Before the isometric and isokinetic tests, the participants warmed up for 5 minutes on a cycle ergometer at their preferred pace, then rested for 3 minutes. Submaximal contractions were also performed for familiarization purposes before each test. All the measurements were performed using an isokinetic dynamometer (Humac Norm Testing & Rehabilitation System, CSMI, Stoughton, MA, USA). The muscles of the knee joint of the dominant leg (the one used to kick a ball) were assessed. During the tests, the participants were given verbal encouragement to contract their muscles as quickly and strongly as possible.
During isometric testing of the knee extensors, the participants sat upright on a dynamometer chair with 85° hip joint flexion and with their trunk and thigh being secured using straps. They also held the handle on the side of the chair with both hands for stability. We aligned the dynamometer axis with the femoral lateral epicondyle and placed the force pad (resistance part) approximately 3 cm above the medial malleolus of the dominant leg. The angle when the participant’s knee joint was fully extended by the researcher was set as 0°. Subsequently, the participants were asked to perform isometric contraction of the knee extensors for 5 s with the knee joint flexed to 60°. The peak torque (PT; Nm) during three contractions was recorded and the mean value was calculated and used in subsequent analyses.
Prior to the isokinetic test, the MAV (100% angular velocity, °/s) associated with the concentric extension of each participant’s knee was measured using isotonic mode. At this time, the range of motion of the knee joint ranged from 90° flexion to 0°, and the resistance value was set to 0, except for the weight of the dynamometer’s force pad. In other words, participants were free to move their knee joint to permit calculation of the MAV. Three trials were conducted, and the fastest value was recorded and used in subsequent analyses. Based on the 100% angular velocity, the 70%, 40%, and 10% angular velocities were calculated for each participant. After MAV was measured, the participants had a 5-minute rest before isokinetic testing.
For the isokinetic test of the knee extensors, the participants sat on a dynamometer chair in the same position as for the isometric test. The positions of the dynamometer axis and force pad were also the same as for the isometric test. Three concentric extensions of the knee were performed for each of the four IAVs (100%, 70%, 40%, and 10%) using the isokinetic mode. We randomly assigned the order of the measurements to each individual and provided a 90-s rest between contractions at each angular velocity to permit the recovery of force-generating capacity. 32 Furthermore, the PT and mean power (MP; Watt) during isokinetic contraction were recorded. The mean values for the three contractions were calculated and used in subsequent analyses.
Statistical analysis
All the measured values are expressed as mean and standard deviation, after confirming the normality of the datasets using the Shapiro–Wilk test. We compared the PT and MP of the knee extensors according to IAV using one-way repeated measures ANOVA. When significant differences were identified, pairwise Bonferroni post-hoc comparisons were conducted and 95% confidence intervals (CI) were calculated. We also calculated partial eta squares (partial η2) and Cohen’s d, representing the effect size. Intra-session reliability (the differences between contraction numbers 1, 2, and 3) was determined using intraclass correlation coefficients (ICC, single measurement, two-way random model, absolute agreement). In addition, 95% CIs and coefficients of variation (CV%) were calculated. The statistical significance level was set as P < 0.05. Data were analyzed using SPSS v.22.0 software (IBM. Corp., Armonk, NY, USA).
Results
We studied 19 participants. The intra-session reliabilities of the MAV, PT, and MP measurements for the knee extensors are shown in the Table 2.
Intra-session reliability of the measurements of maximum angular velocity, peak torque, and mean power of the knee extensors.

ICC, intraclass correlation coefficients; CV, coefficient of variation; MAV, maximum angular velocity.
The measured MAV was 408.84 ± 34.42°/s. However, the 100% MAV isokinetic testing was performed at 396.54 ± 31.72°/s (96.99% of MAV). Table 3 shows the PT and MP during isokinetic concentric extension performed using IAV for 10%, 40%, 70%, and 100% MAV. The same table presents the mean and standard deviation values for each IAV. The PT and MP of the knee extensors, according to the IAV, significantly differed (PT: F = 186.420, P < 0.001, partial η2 = 0.912; MP: F = 48.604, P < 0.001, η2 = 0.730).
Comparison of the peak torque and mean power of the knee extensors, according to the individualized angular velocity (isometric and isokinetic contractions at 10%, 40%, 70%, and 100% of the maximal angular velocity).
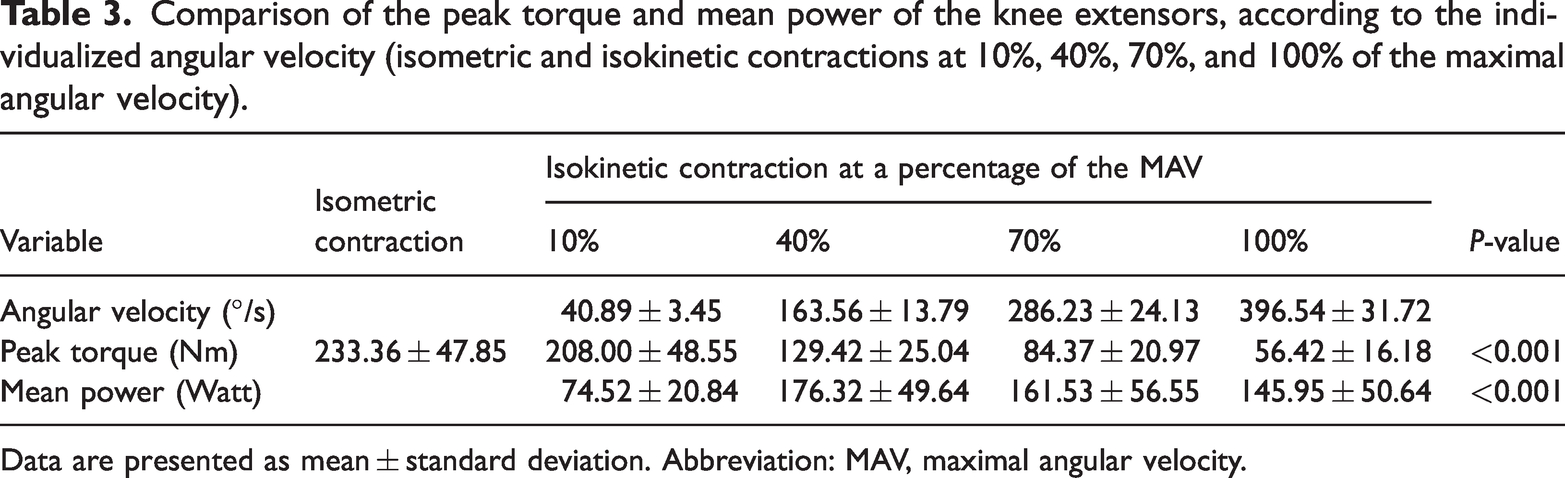
Data are presented as mean ± standard deviation. Abbreviation: MAV, maximal angular velocity.
The results of the post-hoc analysis were as follows (Figure 2): PT significantly decreased with increasing IAV, except between isometric contraction and 10% of MAV (P < 0.001, isometric vs. 40%: d = 2.72, 95% CI: 75.90 to 131.98; isometric vs. 70%: d = 4.03, 95% CI: 119.47 to 178.52; isometric vs. 100%: d = 4.95, 95% CI: 145.56 to 208.31; 10% vs. 40%: d = 2.03, 95% CI: 52.82 to 104.34; 10% vs. 70%: d = 3.31, 95% CI: 93.59 to 153.67; 10% vs. 100%: d = 4.19, 95% CI: 118.23 to 184.93; 40% vs. 70%: d = 1.95, 95% CI: 34.37 to 55.73; 40% vs. 100%: d = 3.46, 95% CI: 59.68 to 86.32; 70% vs. 100%: d = 1.49, 95% CI: 20.32 to 35.57). For MP, 10% of MAV was significantly lower than the faster IAV, and 100% was significantly lower than 40% (P < 0.001, 10% vs. 40%: d = 2.67, 95% CI: −124.27 to −79.32; 10% vs. 70%: d = 2.04, 95% CI: −118.90 to −55.11; 10% vs. 100%: d = 1.68, 95% CI: −100.10 to −41.86; 40% vs. 100%: P = 0.014, d = 0.61, 95% CI: 5.03 to 55.70).

Comparison of the peak torque and mean power of the knee extensor between individualized angular velocities. Red (continuous lines) indicate peak torque and blue (dashed lines) indicate mean power. Significant differences (P < 0.05) are shown vs. ISO (*), 10% (†), 40% (‡), 70% (¥), and 100% (§), respectively.
Discussion
In the present study, we aimed to investigate the changes in PT and AP during isokinetic contraction, according to the IAV, based on the individual’s MAV for knee extension. Our main finding was that the PT of the knee extensors significantly decreased with increasing IAV (from 10% to 100%), except between isometric contraction (angular velocity corresponding to 0) and 10% of MAV. Moreover, their MP was highest at 40% of MAV and significantly higher than at 10% and 100%. Further studies will be needed to determine the feasibility of IAV training by identifying an optimal IAV for exercise prescriptions and to confirm its advantages over current practice (SAV). Unlike in previous studies, we attempted to use IAV, instead of the SAV that is conventionally used in isokinetic contraction. It has been well documented that PT decreases as angular velocity increases and an inverse relationship with power output was also found for IAV during isokinetic contraction. In addition, when using IAV for isokinetic contraction, an angular velocity of between 10% and 40% of the MAV was estimated to increase power, while maintaining relative torque.
The force–velocity relationship, which describes the decrease in contractile force as the contraction velocity of skeletal muscles increases, has been well documented.14,33 During isokinetic testing, both types I and II fibers contribute to torque generation at low velocities, whereas type II fibers primarily contribute to torque generation at higher velocities. 34 In addition, a larger type II muscle fiber area produces more torque at a higher velocity (4.19 rad/s); 35 i.e., as contraction velocity increases, the dropout of slow-twitch fibers, which contribute to torque production, increases. 34 As expected, we found a similar trend of a decrease in PT with an increase in IAV. The PT values obtained were highest for isometric contractions and did not significantly differ from those measured for 10% of MAV (40.89°/s ± 3.44°/s). This result is consistent with those of a previous study in which the PT values measured for isometric and isokinetic (30°/s and 60°/s) contractions did not significantly differ. 14 Given these findings, the frequent use of an angular velocity of 60°/s for isokinetic training and the identification of any improvement in PT would be appropriate.36–38 Moreover, it may be reasonable to use slow angular velocities with IAV (e.g., 10% of MAV in this case) to generate the individual’s PT, representing their maximal strength during isokinetic contraction.
Although PT decreases with increasing angular velocity, the power output is higher at faster angular velocities.39,40 Indeed, the power generated according to angular velocity during isokinetic contraction has been reported to increase to up to 180°/s to 240°/s and then plateau or decrease until 300°/s.41–43 Specifically, in a study using up to 480°/s, the measured power increased up to 180°/s, plateaued between 180°/s and 300°/s, and decreased between 300°/s and 480°/s. 44 Based on the results of studies of isokinetic contraction of the knee extensors, it is generally thought that tests performed at low velocities (or under isometric conditions) primarily reveal strength, whereas those performed at higher velocities primarily reveal power. 37 Consequently, common isokinetic test procedures often include various velocities, but 60°/s and 180°/s are used standardly.35,36 However, some studies, including those of athletes, have shown power output increments up to 288°/s to 300°/s.28,39
In the present study, the maximal AP was measured at 40% of MAV (163.54 ± 13.77°/s), which was significantly higher than that recorded at 10%. Unfortunately, we did not identify the MP generated between 10% and 40% of the MAV, and it is possible that the maximal MP might have been produced in this range. The present results are consistent with those of studies showing that muscle power increases by approximately a third of the maximum contraction velocity before exhibiting a parabolic decline. 45 However, the MPs obtained between 40% and 70% (286.19 ± 24.10°/s) of MAV did not significantly differ. This range has corresponded to the plateau of power production in previous studies using SAV.43,44 This result is consistent with the previous finding that the maximum power extrapolated from the second-order equation of the power–velocity relationship did not significantly differ from the power obtained at 270°/s. 46 As the velocity increased to the individual’s MAV (396.54 ± 31.72°/s), the AP significantly decreased from that measured at 40% of MAV. Given that power is the product of force and velocity, it may theoretically remain constant if the ratio of the decrease in torque and the increase in velocity is equal. However, in the present study, the MP gradually decreased above 40% of MAV. Thus, the loss of torque could be greater than the gain in angular velocity during this period.
Considering that the ability to generate force at various velocities is influenced by physiological, biomechanical, and neural factors,20,21 isokinetic contractions performed at the same angular velocity for all individuals may cause different muscle responses and adaptations that depend on the individual’s muscle performance. Moreover, the faster was the angular velocity used for the measurements, the more pronounced the power difference was between individuals. 47 Differences in muscle fiber composition may explain the difference in power output between individuals. Type I fibers are mechanically the most efficient during isometric and isotonic slow contractions, while type II fibers can produce power at higher velocities. 48 Furthermore, electromyographic activity levels were higher at faster contraction velocities; therefore, greater neural drive from alpha motor neurons to muscles is required for high-power and fast contractions. 49 In previous studies, SAV (e.g., 180°/s, 240°/s) was used for isokinetic contractions, regardless of the muscle fiber type distribution and neural drive in each individual.41–44 Therefore, it may not accurately reflect the ability of an individual to generate joint angular velocity. In other words, the calculation of the peak power using a preselected angular velocity may underestimate (e.g., 30°/s) or overestimate (e.g., 300°/s) the actual isokinetic power. 50 As a result, the difference in the velocity range in which the maximal power output was generated in studies using SAV may be attributed to the characteristics of the study participants.
During isokinetic resistance training, the use of SAV for everyone may not be an optimal approach to improving torque and power generation according to individual neuromuscular characteristics. Using an individualized training program, involving the division of the population into force-deficit and velocity-deficit groups according to individual force–velocity profiles, was found to be more effective at improving jumping performance than standard resistance training. 20 Individualized training programs could serve as optimized training stimuli that are tailored to participants’ force–velocity characteristics. 20 Similarly, our results suggest that the use of IAV rather than SAV for isokinetic training may provide optimal stimulation for training effects because it reflects the different neuromuscular characteristics of individuals. Specifically, isokinetic (10% of MAV) and isometric training appear to be appropriate stimuli to improve strength (PT), whereas isokinetic training (10%–40% of MAV) may be more suitable to improve MP while maintaining PT. In addition, we believe that the risk of injury is low because the angular velocity used for training is determined according to the MAV measured during an individual’s voluntary contractions. However, we did not evaluate the effect of isokinetic training using IAV or compare it with SAV in the present study. Therefore, the data should be interpreted with caution and this issue should be further investigated.
The present study has several limitations. To permit appropriate generalization of the results of the study, the following should be considered. First, given the differences in muscle contraction related to sex and age, the study participants consisted only of healthy young men. Therefore, further studies of other groups should be conducted. Second, at fast angular velocities close to the MAV, the duration of the actual isokinetic (isovelocity) contraction may have been short, and the load range corresponding to the actual isokinetic contraction has not been confirmed. In addition, we did not identify during which periods the measured PT and MP occurred: during the acceleration, load range, or deceleration. Third, considering the interaction of multiple joints or the use of countermovement, joint movements in daily life may generate considerably higher angular velocities than those suggested by the present data. Finally, eccentric contraction of the knee extensor muscles was not evaluated, but rather concentric contraction alone.
Conclusion
In the present study, we measured the PT and MP of knee extensors during isokinetic concentric contraction using IAV, rather than one-size-fits-all SAV for all individuals. Despite this methodological approach, the generation of PT and MP according to the increase in IAV tended to be similar to the well-documented force–velocity relationship (force decreased as the contraction velocity increased). We have estimated the optimized angular velocity range of isokinetic contraction for the improvement of power output while maintaining torque at 10% to 40% of MAV. Using IAV may reflect both the velocity and force components of the power because individuals do not have the same angular velocity. Further studies comparing the use of IAV and SAV during isokinetic testing and training are needed to confirm these findings and develop standardized protocols for IAV training.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241262186 - Supplemental material for Torque and power of knee extensor muscles at individualized isokinetic angular velocities
Supplemental material, sj-pdf-1-imr-10.1177_03000605241262186 for Torque and power of knee extensor muscles at individualized isokinetic angular velocities by Jiheon Hong, Jonggeun Woo and Jeongwoo Jeon in Journal of International Medical Research
Footnotes
Acknowledgements
The authors are grateful to the participants who took interest in and assisted with the study.
Author contributions
JH and JJ conceived and designed the study. JW and JJ collected and analyzed data. JH, JW, and JJ interpreted data and drafted the article. JH and JJ edited and revised the manuscript. All the authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work and to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All persons designated as authors qualify for authorship, and all those who qualify for authorship are listed.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (grant number RS-2023-00249155).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.