
Abstract
OBJECTIVE:
To compare EMG activity of the hip and thigh muscles during traditional static bed exercises and the sit-to-stand exercise in healthy older adults.
METHODS:
Twenty-four healthy, older adults (8 males; age 65
RESULTS:
Hip and thigh muscles were activated differently between the isometric bed and sit-to-stand exercises. Greatest RMS activity was shown in the chair rising phase of the sit-to-stand exercise. No bed exercise exceeded the muscle RMS activity required to perform a sit-to-stand, and only for sit-to-stands were all muscles activated over 40% of maximal; the level required to stimulate muscle strength adaptation.
CONCLUSIONS:
Functional daily activities, such as sit-to-standing, produce greater muscle activity than static bed exercises in healthy older adults. Sit-to-stands should be included in exercise and rehabilitation programs for older adults to evoke sufficient levels of neuromuscular activation for muscle strength adaptation.
Introduction
Muscle activity that produces force is essential for various activities of daily living (ADL), including walking, rising from a chair or stair climbing. These activities afford us physical independence and are targeted for improvement in clinical rehabilitation [1, 2]. For common orthopaedic procedures, such as total hip replacement, persistent muscle loss months after surgery is not surprising [3] and is likely to impair physical performance. A rise in population lifespan has seen more older adults pursuing active ageing, and more patients requiring orthopaedic rehabilitation [4] particularly from an earlier age [5]. ADL-based exercises are becoming more widely used for both healthy older adults and orthopaedic patients to enhance neuromuscular activation and promote muscle strength [6, 7].
Bed exercises have traditionally been advocated following surgical procedures, including hip replacement, to improve muscle function and joint mobility in the hip and thigh, and subsequently achieve functional discharge criteria [8, 9]. However, recent studies have questioned the value of bed exercises [10, 11]. Even with healthy ageing there is a loss of voluntary neuromuscular activation [12], yet within a week post-surgery, this age-related muscle activation loss is substantial, and accompanied by reduced hip muscle strength and leg-press power [13]. Rehabilitation practices are moving from the traditional range of motion (ROM) and static muscle contraction bed exercises to functional approaches, such as progressive resistance training. However, the traditional exercises remain part of many rehabilitation protocols [14, 15, 16].
Enhanced recovery after surgery (ERAS) principles have reduced hospital length of stay to 1 to 3 days after orthopaedic procedures [17, 18]. These principles include early mobilisation to reduce the surgical stress response [6]. For example, patients are now commonly mobilised within 4 hours of surgery, and discharged home within 3 days capable of fulfilling functional discharge criteria (e.g., chair/bed transfers and aided walking) [19]. The ability to initiate sit-to-stand movement is associated with physical independence [20] and considered an ADL presenting high biomechanical demand that translates to numerous daily movements [21, 22]. Supervised, progressive resistance training may be safe and effective in improving physical performance in older adults [1, 23]. However, sit-to-stands may offer a practical and functional exercise for both healthy and clinical older adults.
From a clinical perspective, if there is little evidence to support the use of static bed exercises, and patients are now capable of mobilising on the day of surgery through an ERAS pathway, this questions as to whether bed exercises should continue to be part of rehabilitation protocols. Other exercises may more effectively increase strength and function. Sit-to-stand movements are commonly used as a functional exercise in outpatient exercise programmes following surgery. Recently, a simple, progressive sit-to-stand exercise programme has shown to be feasible for hospitalised patients aged over 65 years [7]. As a proof-of-concept, it would seem appropriate to compare muscle activity between traditional bed exercises and sit-to-stand exercises in a healthy older cohort. Therefore, this feasibility study aims to establish whether a functional exercise, such as sit-to-standing, is more effective in activating muscles than traditional exercises. The study is informed by the hypothesis that hip (gluteus medius, maximus) and thigh (rectus femoris, vastus medialis, biceps femoris) muscle activation will be greater during sit-to-stand exercise, than during static bed exercises for community-dwelling older adults.
Methods
Participants
Twenty-four older adults (8 males; mean
Experimental design
Electromyographic (EMG) activity was measured during isometric exercises commonly prescribed after total hip replacement, and during the sit-to-stand test. Isometric exercises involved submaximal contractions of the gluteal, abductor, inner quadriceps and quadriceps, whilst lying on a therapy-plinth. Contractions were submaximal to be consistent with early post-operative (up to 72 hours) exercises, with instruction given to contract
Familiarisation with procedures and exercises were followed by measurements of the following participant characteristics: height, body mass (Seca model 274, Seca Ltd, Germany), blood pressure (Omron M4-I, Omron Healthcare Ltd, UK), grip strength and 10 m walking speed (Table 1). Standing grip strength was the highest of three maximum isometric repetitions (30 s rests; non-dominant hand), using a digital handgrip dynamometer (DHD-3, Saehan Corporation, Changwon, Korea). Normal walking speed was averaged from three 20 m trials (60 s rests; 5 m acceleration, 5 m deceleration zones to ensure steady-state) in the laboratory [26].
Physical characteristics of participating older adults
Physical characteristics of participating older adults
Data are presented as mean
Skin preparation for sensor placement involved shaving, gentle abrasion and alcohol-wipe cleansing. Bipolar SX230-1000 recording sensors were affixed to the mid-aspect of each muscle belly according to SENIAM recommendations [27], and connected to a portable Biometrics PS850 system (DataLOG, Biometrics Ltd., Newport, UK).
Sensors were placed on the: rectus femoris (mid-way between a line from the anterior superior iliac spine and the proximal patella border), vastus medialis (two-thirds along a line from the anterior superior iliac spine to the lateral patella), gluteus medius (mid-way between the inferior iliac spine and the greater trochanter), biceps femoris (midway between the ischial tuberosity and lateral epicondyle of the tibia) and gluteus maximus (midway between the sacral vertebrae and the postero-superior edge of the greater trochanter) of the non-dominant limb [28, 29]. The reference sensor was also placed over the lateral malleolus.
EMG signals were normalised to the highest peak amplitude recorded from three,
Bed exercises and sit-to-stands
Four exercises were performed on an adjustable therapy-bed: static gluteal contractions (Fig. 1a), active hip abduction (Fig. 1b), static quadriceps contractions (Fig. 1c) and active inner quadriceps contractions (instructed to contract the quadriceps with a foam-roller placed under the knee to slowly raise the heel) (Fig. 1d) [8]. Ten,
Static gluteal contractions in a lying prone position, with neutral hip rotation (a); Active hip abduction in the frontal plane in a lying supine position (b); Static quadriceps contractions in a lying supine position (c); Active inner quadriceps contractions lying supine, with a foam roller placed under the active knee (d).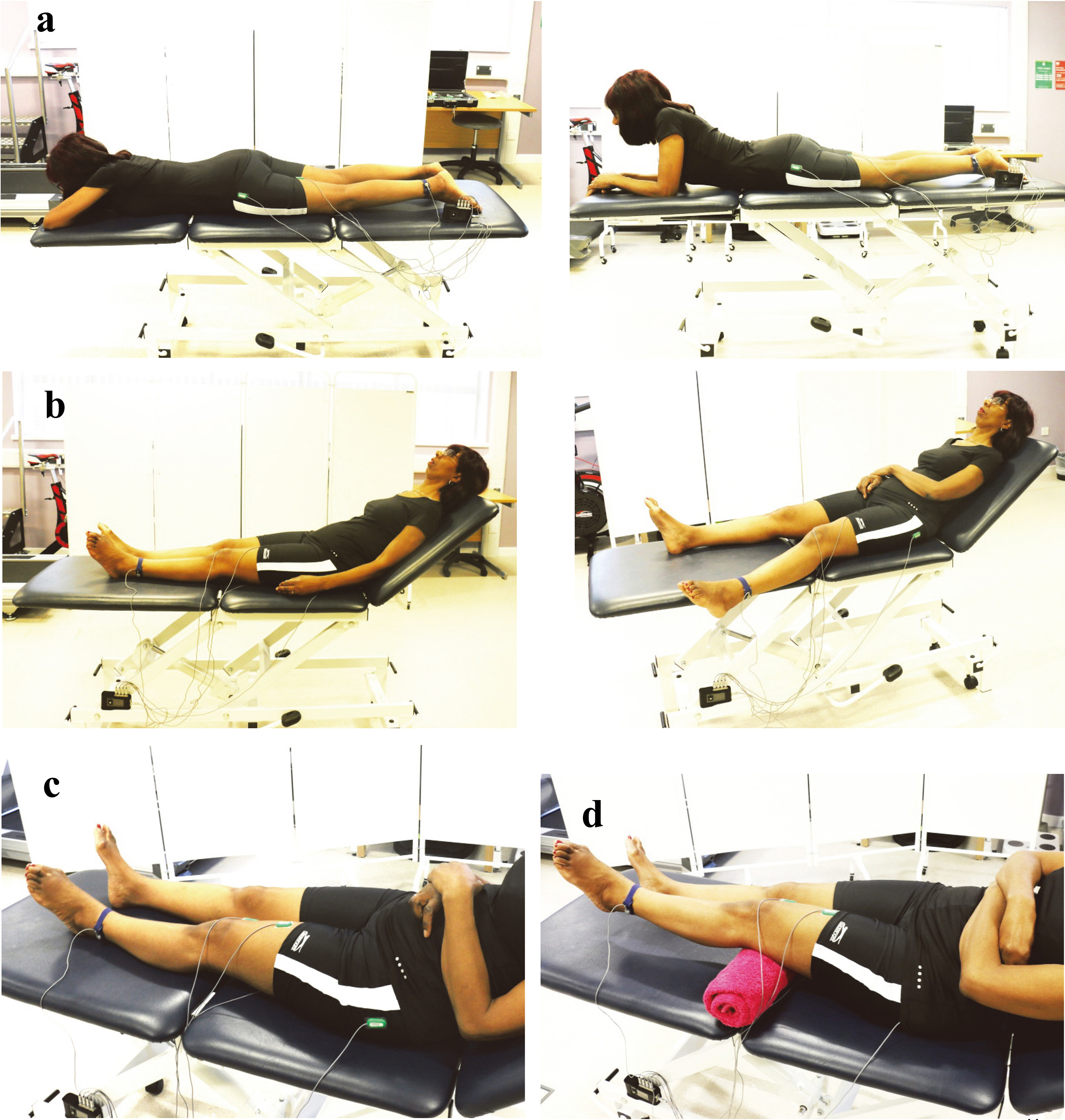
Sit-to-stand movement. The participant was seated in an upright position with their arms folded across their chest; instruction was given to rise to a standing position (sit-stand), and then return to a seated position (stand-sit) as many times possible within a 30 s period.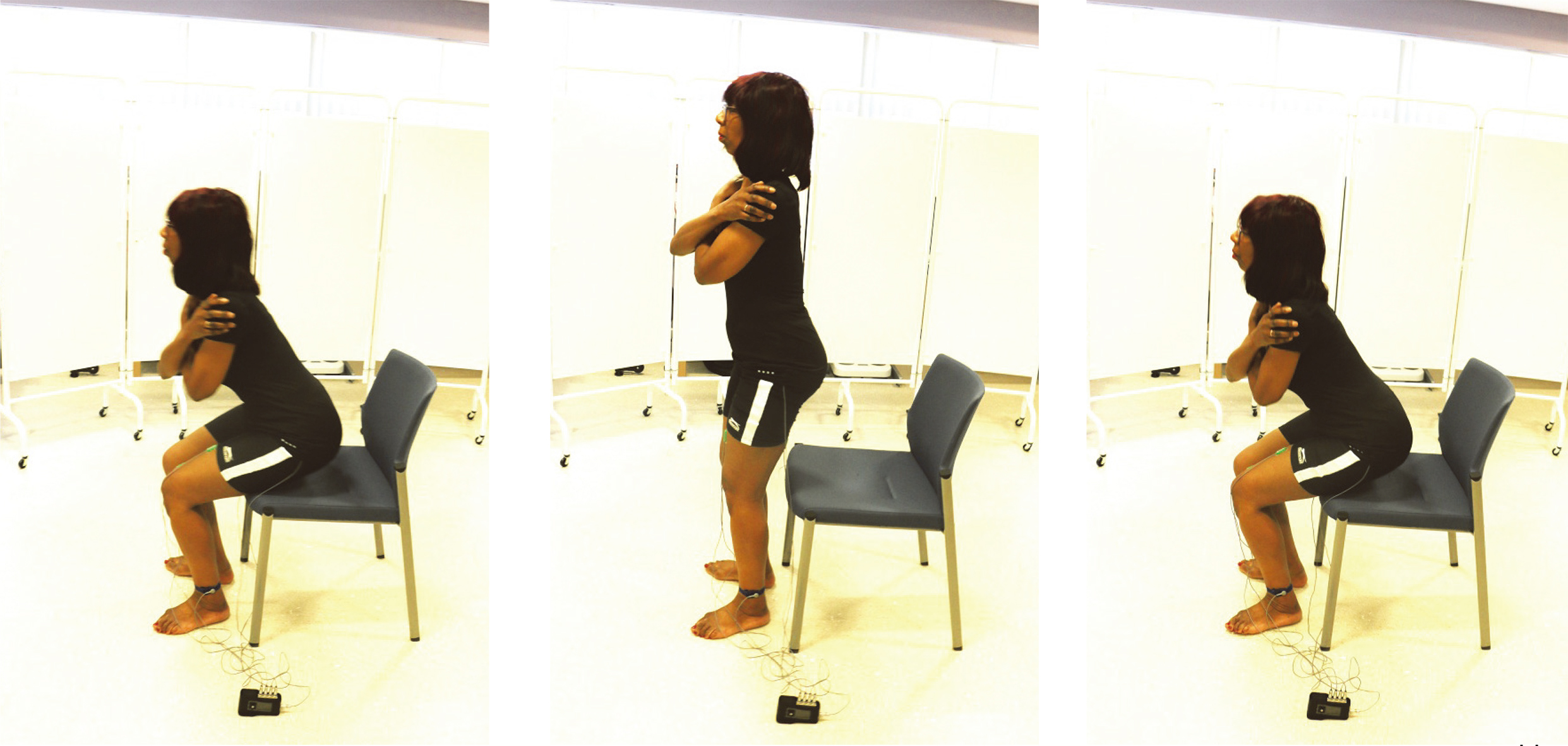
Intraclass correlation coefficients describing the within-session reliability of muscle EMG activity during three repetitions of each exercise
Mean, with 95% confidence intervals in parentheses;
Normalised RMS EMG activity during rehabilitation exercises and sit-to-stand movements for each upper-leg muscle
Data are mean
Normalised RMS EMG activity during rehabilitation exercises and sit-to-stand movements for the rectus femoris (a), vastus medialis (b), gluteus medius (c), biceps femoris (d) and gluteus maximus (e) muscles.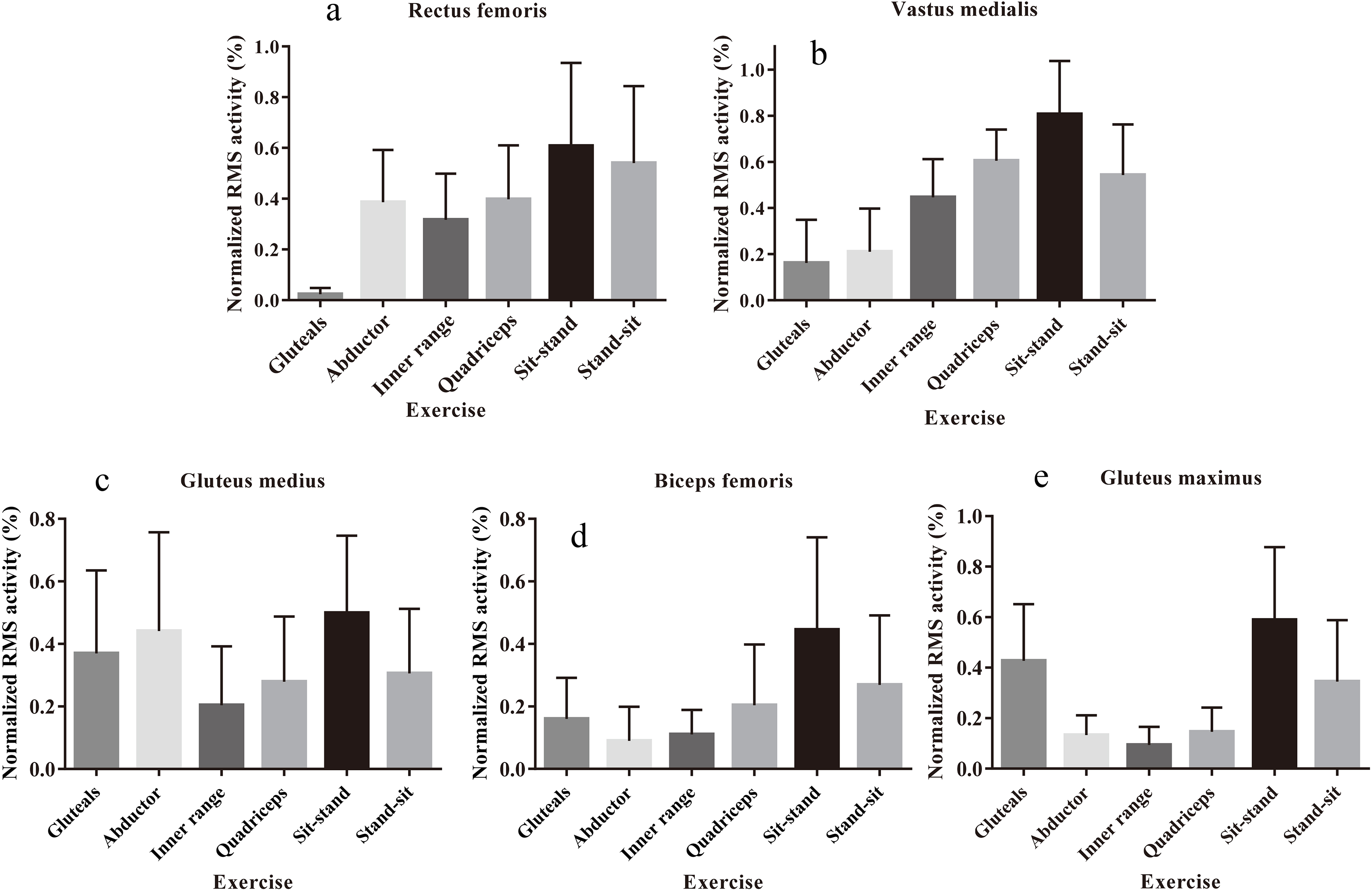
Sit-to-stands were performed following bed exercises, in the context of physical outcome testing. Participants were seated upright in the middle of a chair (46 cm), with feet shoulder-width apart and arms across the chest. Instruction was given to rise to an upright position (sit-stand), and then return to a seated position (stand-sit) in a controlled-manner, as many times as possible within 30 s (Table 1 and Fig. 2) [30]. Electromyograms were averaged over the middle three sit-to-stands within 30 s, and separately analysed for sit-stand and stand-sit phases [32].
Raw signals were sampled at 1000 Hz using amplifier-embedded sensors (10 mm diameter, 20 mm inter-electrode distance; bandwidth
Statistical analysis
GraphPad Prism version 6.00 (GraphPad Software, La Jolla, CA, USA) was used for analysis. Same-day, test-retest reliability of raw EMG recordings was determined using intraclass correlations coefficients (ICC) (absolute agreement, two-way random) [35]. EMG recordings for the first, middle and final contractions were used to assess reliability for each exercise set.
Shapiro-Wilk tests confirmed non-normal distribution for RMS data; non-parametric tests analysed the RMS for bed exercises (four exercises) and sit-to-stand (two phases) exercises. One-way, Friedman’s repeated measures ANOVA compared RMS activity for each muscle, during bed exercises, and sit-stand and stand-sit exercises. Paired Wilcoxon Signed-Rank tests located specific RMS differences between individual exercises. Data were expressed as mean and SD, with 95% confidence intervals (CI). Effect sizes (
Results
Reliability of EMG recordings
Test-retest reliability data of muscle EMG activity during three contractions for each exercise are shown in Table 2.
EMG recordings during static rehabilitation exercises and sit-to-stands
Normalised RMS activity for each muscle (expressed as a percentage of iMVC) during each bed and sit-to-stand exercise are shown in Fig. 3a to e (specific values in Table 3).
Rectus femoris RMS activation was significantly different between exercises (
Vastus medialis RMS activity was significantly different between exercises (
Gluteus medius RMS activity was different between exercises (
Biceps femoris RMS activity was different between exercises (
Gluteus maximus RMS activity significantly differed between exercises (
Discussion
The current study’s purpose was to compare the muscle activity of five hip and thigh muscles during: i) traditional, isometric bed exercises and, ii) functional, sit-to-stands in healthy, older adults. Observations from EMG signals during muscular contraction can provide information as to which exercises result in higher neuromuscular activation, and subsequently have greater potential benefit to improve functional muscle strength.
Our findings indicate that the hip and thigh muscles were activated differently for bed (isometric) and sit-to-stand (dynamic) exercises. Greatest activation was shown during chair rising when performing the sit-to-stand exercise. Although agonist muscle activation for specific exercises (i.e., gluteus medius/maximus for isometric gluteals; rectus femoris/vastus medialis for isometric quadriceps) was similar between bed and sit-to-stand exercises, for no bed exercise did muscle activity exceed that required to sit-stand. Hamstrings (biceps femoris) activity failed to exceed 40% MVC (from 9–15%) for bed exercises, yet hip and thigh muscle activity was at least 45% MVC for sit-stands. Only for sit-to-stands were all muscles activated over 40%; the level required to stimulate muscle strength adaptation [36].
Sit-to-stands involve the quadriceps contracting through a concentric phase to rise from the chair, and then an eccentric phase to control the body’s lowering into a seated position. Lower activation when sitting, compared to standing, was likely due to a lesser requirement for motor unit activity during eccentric actions of the quadriceps and gluteal muscles [37], and the gravitational effect when controlling the body’s lowering. When sitting, the lengthening action of the quadriceps may partly explain the similar muscle activity between specific bed exercises, and stand-sit movements. Our healthy cohort was able to control the lowering phase when becoming seated, without involving additional quadriceps and gluteal muscle recruitment. All of our participants succeeded in sit-standing in a controlled manner for 30 s without falling, suggesting a feasibility exercise in healthy older adults. However, orthopaedic patients (who receive bed exercises) require greater quadriceps activation to control the eccentric, sitting phase following surgery [38]. Sit-to-stands are feasible as an outcome measure for hospitalised patients; however as an exercise, feasibility is unknown. Future work should assess the feasibility and neuromuscular activity of hip and thigh muscle in a cohort receiving bed exercises, such as orthopaedic patients in the early stages of recovery.
Traditional practices in rehabilitation and exercise medicine pathways should be questioned regarding specificity and function [39]. At present, patients are undertaking static bed exercises as part of their rehabilitation. However, now patients are mobilised on the day of surgery, and perform sit-to-stands as part of this mobilisation, the value of static bed exercises should be questioned in clinical practice. Our findings from age-matched healthy adults indicate that more functional exercises with application to activities of daily living could be performed instead. This feasibility study confirms our working hypothesis that there is greater muscle activation in sit-to-stand exercises, than in static bed exercises in healthy older adults. This suggests that sit-to-stand exercises are more likely to increase muscle strength effectively than bed exercises. Whilst this finding may appear unsurprising to some, it has not previously been established, and given the current practice of physiotherapists [14, 15, 16] appears not to be appreciated by the profession. The study findings should be confirmed in the relevant clinical population, but this study involving healthy older adults suggests that the proposed trial is feasible within a clinical setting.
Muscle strength can be gained through progressive resistance training [40]. This involves building muscular strength by exercising muscles against an external force set at a specific intensity, and this resistance is adjusted throughout the programme. Sit-to-stand exercise training could be developed adopting these principles, building on an individual’s initial maximum strength in order to improve muscle strength, and thereby maximising strength gains. Our findings support the use of sit-to-stands to increase muscle activity of specific hip and thigh muscles for healthy older adults, rather than isometric bed exercises. As the gluteus muscles were moderately active (medius, 37%; maximus, 43%) during gluteal contractions, sit-to-stands should be seen to complement, rather than replace traditional bed exercises in exercise training programmes for older adults.
STROBE schematic of the observational study design. 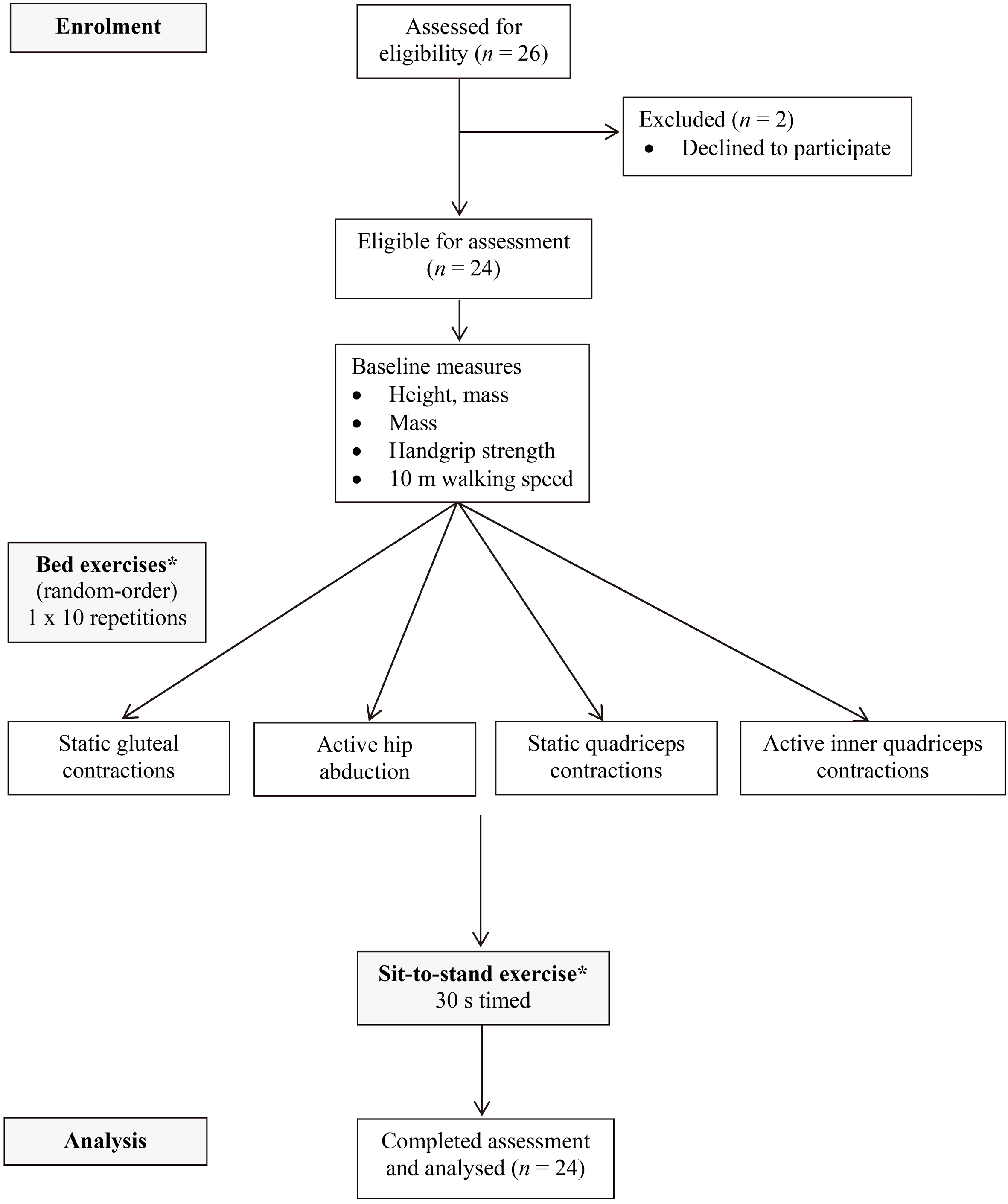
We plan to repeat this study in a clinical setting, with patients recovering from hip replacement surgery to examine whether sit-to-stand exercises can produce higher activation amplitudes than bed exercises. The sit-to-stand protocol (Fig. 4) will also be tested for feasibility as a rehabilitation exercise for patients following hip replacement surgery, by completion rates (of sets and repetitions) and acceptability. For older adults undergoing orthopaedic surgery, muscle weakness, pain and dizziness are the main reasons for delaying hospital discharge [18]. We expect that patients with total hip replacement will exhibit different movement patterns to healthy adults, and subsequently different muscle activation strategies, when performing sit-to-stands as an exercise,
Our study is limited by the participant sample; older adults who are active and ambulatory. The EMG signal amplitude during bed exercises and sit-to-stand exercises would likely differ for patients in the acute post-operative phase due to pain, impaired function and limited ROM. However, this feasibility study’s aim was to determine if there were significant differences in EMG activity in individual hip and thigh muscles during exercises (with an exercise-dependent effect between isometric bed and sit-to-stand exercises) for healthy adults (age-matched to the most common hip replacement age demographic). In a patient population the magnitude of differences would likely be greater, but also constrained by limited movement patterns. We also accept that intramuscular, fine-wire EMG could have been used to improve the sensitivity of muscle activity assessment. Heterogeneous gluteus medius activity may partly be a consequence of variable activation of different specific muscle segments, and arising from their mixed fibre orientations [1, 41]. Surface EMG was used in this study based on pilot testing for i) participant acceptability, and ii) the least invasive technique to detect magnitude of effect.
As bed exercises are unlikely to harm an individual and may complement functional exercises there is no loss in keeping them as part of an exercise rehabilitation programme. However, we suggest that it is more beneficial to the healthy individual if the physical trainer dedicates time to teaching and supervising functional exercises, such as the sit-to-stand. For patient groups bed exercises may play a role by having circulatory effects to prevent deep-vein thrombosis, however this is yet to be determined.
Sit-to-stands appear to be a more effective exercise in activating the hip and thigh muscles of healthy older adults, than isometric bed exercises. Although using a functional outcome test (i.e. sit-to-standing) as an exercise did not produce maximum activation for a given muscle, it was a feasible method of producing greater amplitudes for specific hip (gluteus medius and gluteus maximus) and thigh (rectus femoris, vastus medialis, biceps femoris) muscles, when compared to bed exercises. Isometric bed exercises are used during early rehabilitation in hospital settings, particularly for orthopaedic patients who often mobilise on the day following surgery. However, there is little evidence to support the role of isometric bed exercises for healthy or hospitalised older adults. Sit-to-stands may offer a safe and feasible, functional exercise to maximise neuromuscular activity in the hip and thigh muscles for community-dwelling older people. This study now needs to be repeated with orthopaedic patients in the early recovery phase after surgery (i.e. 12–72 hours) to determine feasibility in a clinical setting.
Footnotes
Acknowledgments
This study would not have been possible without our participants’ commitment, time and effort. The study design was prepared by JPG, TI and TW; with data collected by JPG and LB; and the analysis, interpretation and manuscript preparation undertaken by JPG, LB, TI and TW. The final manuscript was approved by all authors.
Conflict of interest
The authors have none to declare.