
Abstract
BACKGROUND:
While extreme changes in body position (e.g., standing vs. sitting) have been shown to affect knee extensor strength, little is known regarding how less extreme changes in body position affect knee extensor strength and activation.
OBJECTIVE:
This study evaluated the effect of four seated positions on the maximum voluntary isometric contraction (MVIC) and electrically-evoked isometric strengths of the knee extensors.
METHODS:
Forty healthy subjects participated. MVIC strength, electrically-evoked strength, and voluntary activation of the quadriceps muscles were measured under four seated positions: 1) 22.5–25
RESULTS:
MVIC and electrically-evoked strengths increased (
CONCLUSIONS:
Knee extensor MVIC and electrically-evoked strengths were modestly enhanced as the body was tilted backwards. The use of a semi-reclined position may assist in obtaining a more forceful contraction of the knee extensors, thereby potentially resulting in better strength training outcomes.
Introduction
Strength assessment and strengthening of the knee extensor muscle group (i.e., quadriceps femoris) play an important role in research and patient care for various musculoskeletal disorders, such as knee ligament or meniscus tears, cartilage degeneration, and patellofemoral pain syndrome. However, the optimal testing position(s) and/or joint configuration(s) to evaluate knee extensors remain unknown. For example, while the optimal knee angle(s) for maximum voluntary isometric contraction (MVIC) activation and strength of the knee extensors have been studied extensively, there is no consensus on that angle. Several studies suggested an optimal angle of approximately 90
Given that the rectus femoris muscle spans both the hip and knee joints, position of the hip joint is another factor that may affect MVIC activation and strength of the knee extensors. However, previous findings on the optimal hip flexion angle(s) for knee extensor MVIC strength remain controversial [7, 8, 9]. Opposite results have been reported regarding whether a greater knee extensor MVIC strength could be achieved when the hip was flexed at 90
One possible factor that may have contributed to the inconsistent findings regarding the optimal knee/hip joint angle(s) for knee extensor activation and strength is the variation among studies in body position in the sagittal plane because of the wide variation in seating among different dynamometers that have been used to assess knee extensor strength. While holding hip and knee angles constant (120
However, little is known regarding the effects of less extreme changes in a sitting testing position on muscle activation and strength, which is more relevant and practical to be implemented clinically when compared to extreme modifications in testing positions (e.g., inversion, standing). Such information is thus critical for determining the optimal sitting position for knee extensor strength testing/training and standardizing testing protocols during muscle functional evaluation. The primary objective of our studies, therefore, was to assess the effect of altering body tilting position during sitting in the sagittal plane, while keeping the knee and hip angles constant, on MVIC muscle activation and strength as well as electrically-evoked strength of the knee extensors muscles. We hypothesized that altering body position during sitting would modify the activation and strength of the knee extensor muscles.
Methods
Participants
Twenty young, healthy subjects [14 males and 6 females; mean (
Study design
This study was based on a repeated-measures design. MVIC muscle activation and strength as well as electrically-evoked strength of the knee extensors muscles were measured under 4 different seated positions.
Procedures
Study I: Effect of sagittal body position on strength and activation of the knee extensors
The knee extensors of the right leg were tested by having the subject seated in a knee extension/flexion machine (NT-1260, Nautilus Fitness Products; Louisville, CO, USA) with the hip and knee set at 90
Schematic of the experimental setup. The subject’s head, trunk, and legs were secured with straps. The four testing positions were then achieved by tilting the knee extension machine forward and backward in a random order (A). To calculate knee extension torque, a force transducer (for Study I) and strain gauge (for Study II) were attached to the metal frame of the knee extension/flexion machine (B).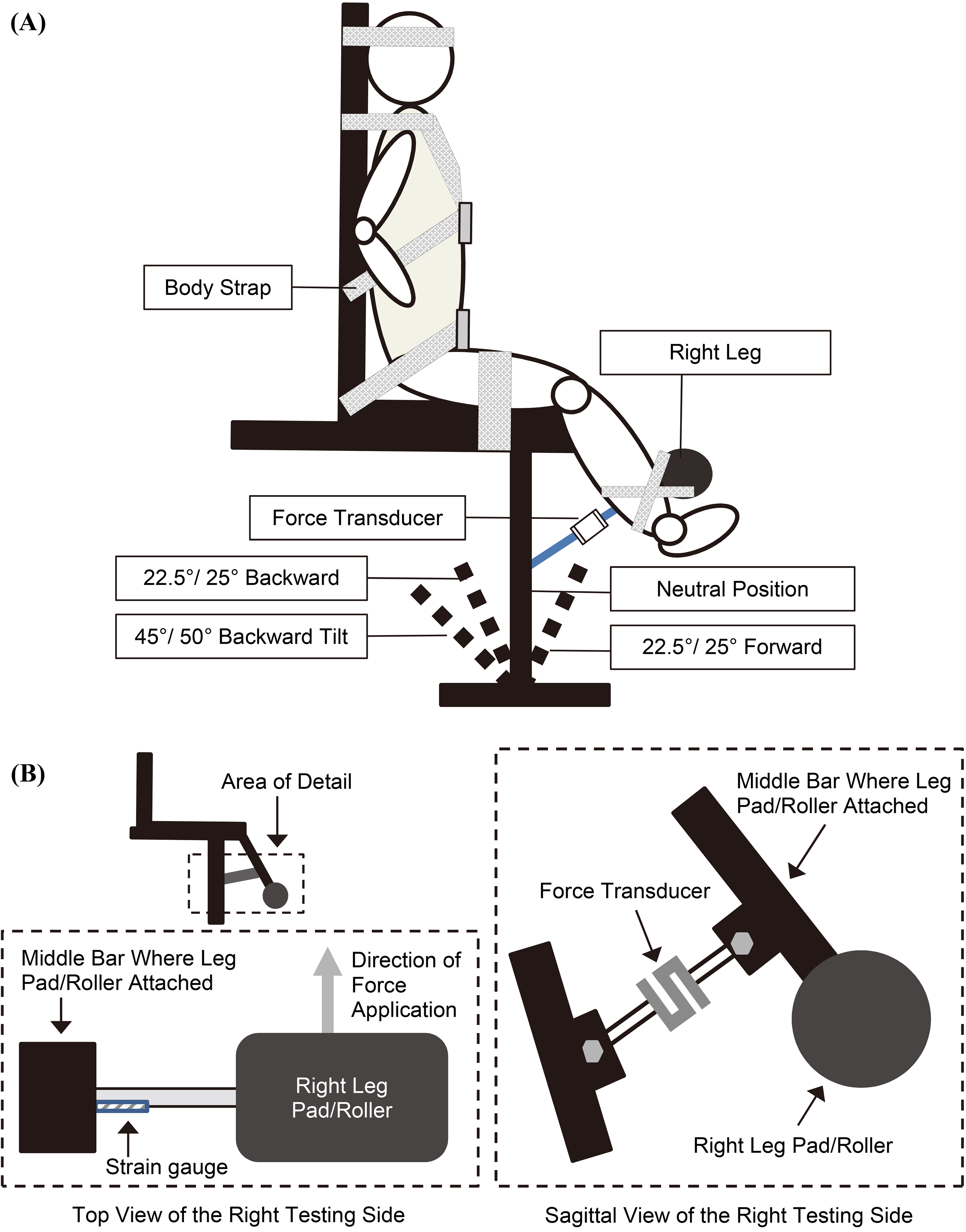
To measure knee extensor torque production, a force transducer (SBO-300, Transducer Techniques; Temecula, CA, USA) was attached on one end to the back of the bar upon which the subject kicked against with his/her right leg and the other end attached to immovable bracing of the machine (Fig. 1B). The output signal of the force transducer was amplified (TMO-2, Transducer Techniques; Temecula, CA, USA) and sampled at 5000 Hz using a combined A/D and D/A board (KPCI-3116, Keithley Instrument; Solon, OH, USA), 2.2-GHz Pentium computer, and custom written programs with TestPoint software (ver. 7.0, Measurement Computing, Norton, MA, USA). The force recorded was then multiplied by the moment arm (distance from the knee axis to the center of bar that the subject kicked against) to calculate the knee extensor torque. To remove the varying effects of the gravity among testing positions on strength recording, for each testing position, the passive torque exerted by the weight of the leg was determined prior to each measurement when the subject was instructed to relax completely. The recorded value of the passive torque (average from a 1-s recording) was then used to correct the subsequent strength measurements.
An interpolated twitch procedure was used to quantify MVIC muscle activation and strength as well as electrically-evoked strength at each of the four body positions [13, 14, 15]. For stimulating the knee extensors, two 7-cm
To determine the stimulation current needed for the interpolated twitch procedure, a series of electrically-evoked isometric contractions of the knee extensors was performed with the current being increased on succeeding stimulations. Each stimulation consisted of a paired-pulse stimulation, i.e., two 0.2-ms pulses separated by 10 ms. Stimulator current was initially set to 100 mA and increased by 20 mA on each succeeding stimulation. Progressively stronger stimulations were delivered once every 20 s until the peak contraction torque reached a plateau and then showed a decline on two successive stimulations. The current eliciting the highest peak torque on the plateau of the torque-current curve was used for the remainder of the test session. Determination of the optimal stimulation current was performed at each of the 4 body positions.
To do the interpolated twitch procedure, the subject was instructed to perform a 3-s MVIC of his/her right knee extensor muscles. Auditory cues elicited by the custom-written TestPoint software were used to signal the subject when to start and stop the contraction. At 2.5 s into the MVIC, the muscle group was stimulated with a paired-pulse stimulation, and the increase in muscle torque over the MVIC level (i.e., interpolated twitch torque, ITT) was measured. At 2 and 4 s after the end of the MVIC, the same paired-pulse stimulation was administered again to relaxed muscle to determine the peak electrically-evoked torque (EET). The average value for the two stimulations was used as the electrically-evoked strength and as the EET for the percent muscle activation calculation. The percent muscle activation during MVIC was calculated as 100% (1 – ITT/EET) [13, 14, 15]. MVIC strength was defined as the average torque between 2 and 2.5 s into the MVIC.
Muscle electrical activities of the knee extensor and flexor muscles were also assessed during the interpolated twitch procedure using preamplified surface EMG electrodes (Delsys DE-2.1, Boston, MA, USA). Overlying skin was first prepared by shaving any hair and cleaning with an alcohol wipe. Electrode placement was as per Rainoldi et al. [16]. For the VL muscle, an EMG electrode assembly was placed at 33% of the distance between the superior lateral patella and ASIS. For the VM muscle, an electrode assembly was placed over muscle at 30% of the distance between the superior medial patella and ASIS. For the biceps femoris (BF) and semitendinosus/semimembranosus (ST/SM) muscles, the subject was placed in the prone position with the knee extended. For the BF muscle, an electrode assembly was placed at 67% of the distance from the ischial tuberosity to the lateral border of the popliteal cavity. For the ST/SM muscles, an electrode assembly was placed at 67% of the distance from the ischial tuberosity to the medial border of the popliteal crease across the ST tendon. The longitudinal axis of each electrode assembly was aligned parallel to the estimated longitudinal axis of the underlying muscle fibers. An adhesive 2-cm
During testing for each body position, six interpolated twitch procedures were performed, with one minute of rest between procedures. Of the six interpolated twitch procedures, the three best attempts (i.e., the three trials with the highest peak MVIC torques) were determined and their data averaged together for use in the statistical analyses.
The MVIC strength (A), electrically-evoked torque/strength (B), and percent activation during MVIC (C) recorded under the four body positions. Values are shown as Mean 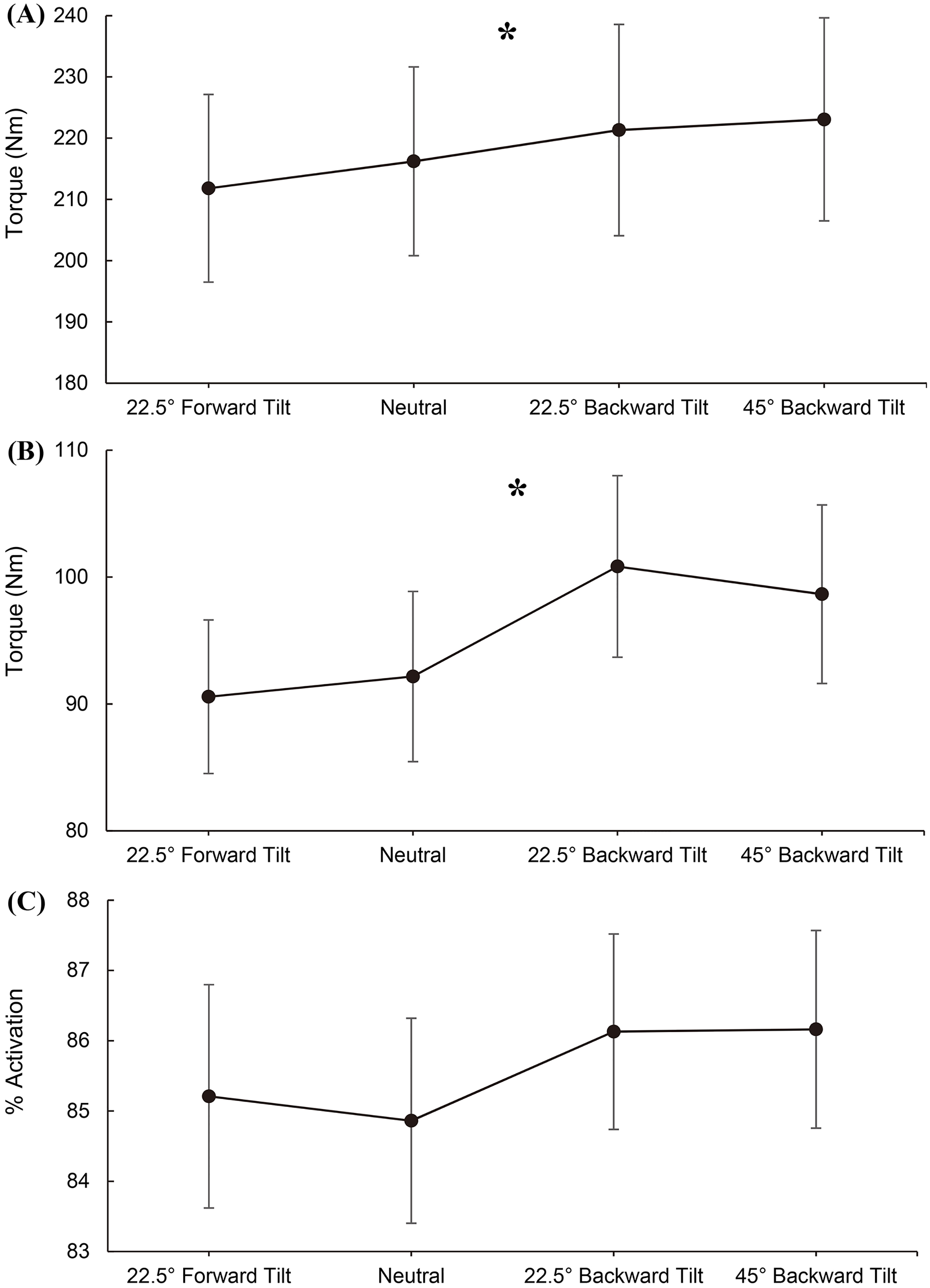
The EMG RMS values for the VL (A), VM (B), BF (C), and ST/SM (D) muscles. 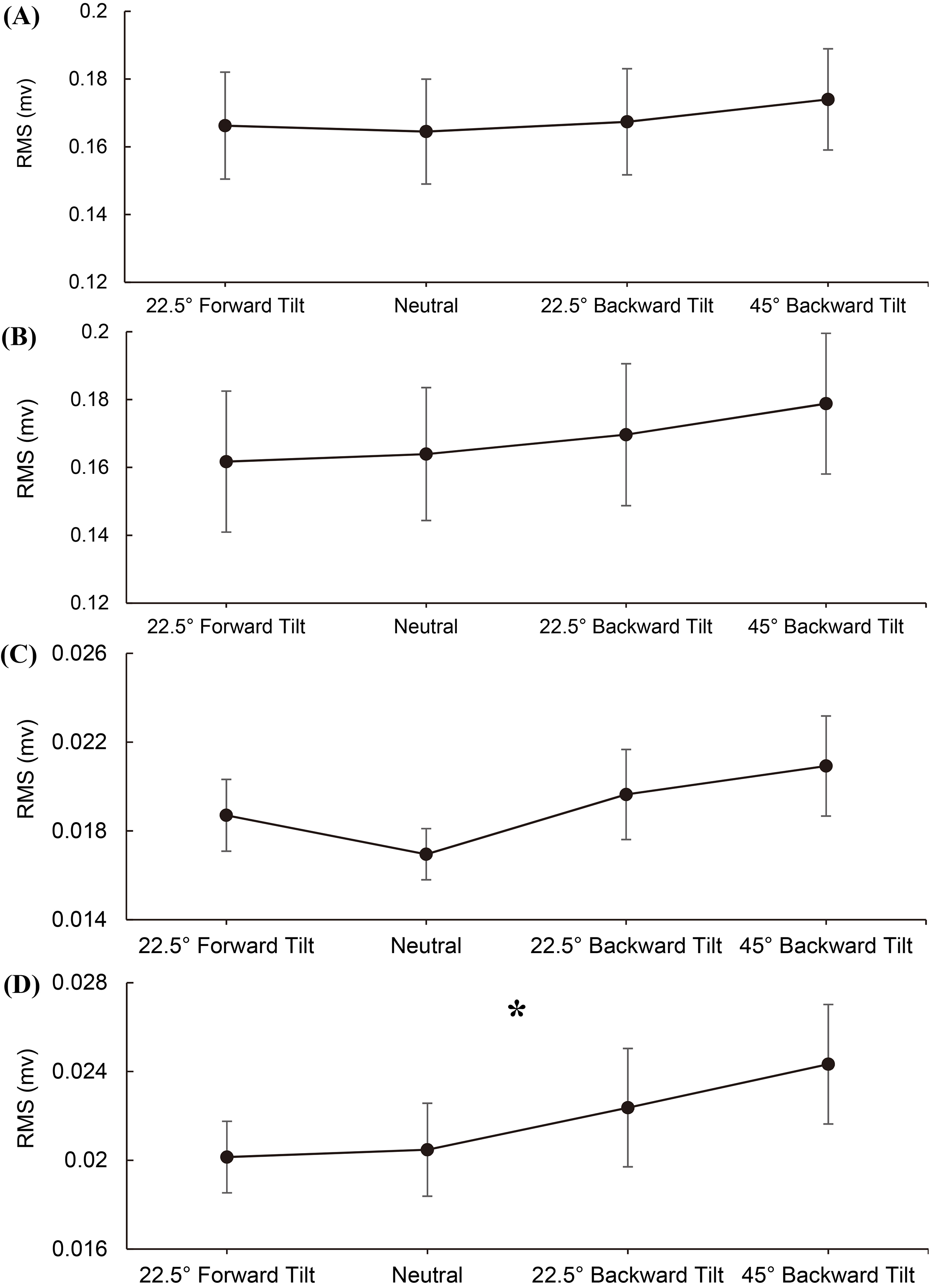
The un-potentiated (A) and potentiated (B) electrically-evoked isometric torque of the knee extensor muscles recorded under the four body positions. Values are shown as Mean 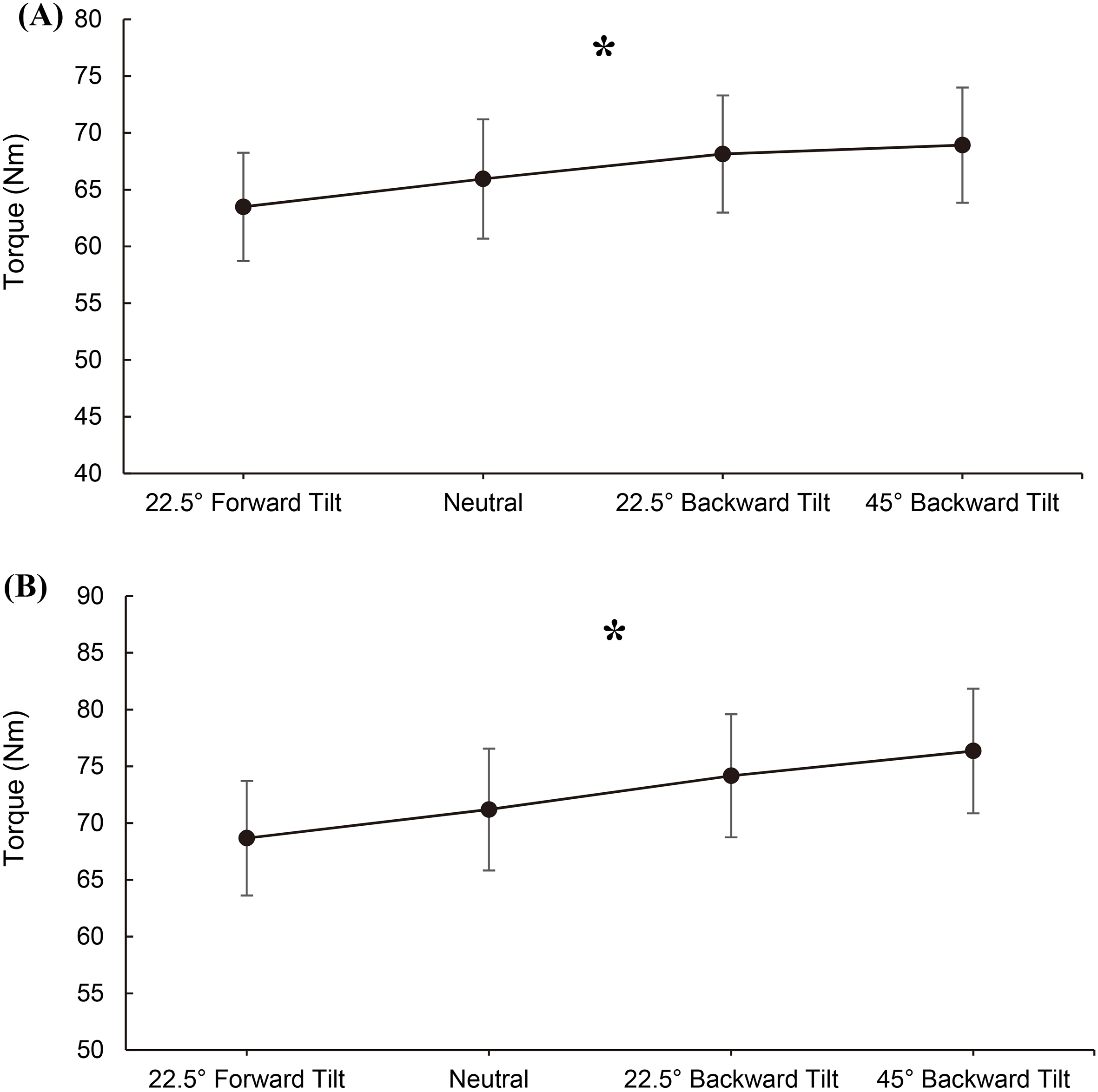
Because of our surprising finding in Study I of a sagittal body position effect on electrically-evoked strength, we conducted Study II to confirm and extend our Study I findings. In Study II, we used a force-measuring methodology (i.e., strain gauge-based) different from that used in Study I. This was done because the strain gauge-based system was less susceptible to noise induced by sudden impact forces on the knee extension/flexion machine. In Study II, we also focused exclusively on measuring electrically-evoked strength, specifically strength measured under unpotentiated and potentiated conditions.
The equipment and procedures used in Study II were identical to those used in Study I with the following exceptions. First, as mentioned above, the force transducer-based system for measuring torque was replaced. A strain gauge (model SGD-30/120, Omega Engineering, Inc.; Norwalk, CT, USA) was bonded to the back of the bar upon which the subject kicked against (Fig. 1B). Additionally, an Omega BCM-1 bridge completion module and DMD-465 signal amplifier were used to record the torque. Second, three of the four body positions used were changed slightly to obtain the maximal range possible in the sagittal plane with our equipment. The forward and backward tilts of 22.5
Statistical analysis
The dependent variables for Study I included 1) MVIC strength, 2) percent muscle activation during MVIC, 3) electrically-evoked strength, and 4) EMG RMS of the knee extensor (i.e., VM and VL) and flexor (i.e., BF and ST/SM) muscles. The dependent variables for Study II were the unpotentiated and potentiated electrically-evoked strengths of the knee extensor muscles. For each variable of interest, a one-way repeated measures ANOVA with linear contrast was used to compare the difference among the four testing positions with a significance level of 0.05 (SPSS ver. 21, IBM; Armonk, NY, USA).
Results
For Study I, a significant linear relationship was found between sagittal seated body position and knee extensor strength, both MVIC and electrically-evoked (
Discussion
The primary purpose of this study was to determine the effects of sagittal body position on knee extensor muscle activation and strength during a MVIC as well as the effect on electrically-evoked strength. The results in part supported our hypothesis that altering body position may result in changes in the strength and activation of the knee extensor muscles. Specifically, we found in Study I that as body position was changed from the 22.5
While the effects of body position on knee extensor strength have been investigated [10, 11], the experimental approaches in previous studies involved extreme changes in body position (e.g., standing vs. sitting, upright vs. inverted). Our modification of a sitting position by tilting the subject forward/backward while maintaining the same body/joint configurations is more comparable to knee extensor strength testing protocols commonly used in clinical practices. The observed linear increase in MVIC and electrically-evoked strengths with increased backward tilt angle may help explain some of the discrepancies in previous studies concerning the optimal joint position(s) of assessing knee extensor strength [1, 5, 7, 9]. Based on our findings, standardization of body tilting position during sitting in addition to the knee and hip angles must be considered when assessing knee extensor muscle strength. Future studies with combinations of various body tilting and lower-extremity joint positions may help determine the optimal body configuration(s) for examining knee extensor strength.
The mechanism(s) associated with the increased MVIC strength with backward body tilt remain(s) unclear. The varying effects of the gravity among testing positions were minimized by removing the passive torque exerted by the weight of the leg prior to each strength measurement. The increased MVIC strength also cannot be explained by increased central activation or increased muscle/nerve tissue excitability because no significant changes were observed among body positions in either percent muscle activation or EMG amplitude of the VM or VL muscles. A very small increase in ST/SM EMG amplitude indicating enhanced co-contraction was observed as the body was tilted backwards but this observation is directionally wrong in terms of explaining the body position effect on MVIC strength.
Our only explanation for the MVIC strength increase with backward tilting is based on our observation of a body position effect on electrically-evoked strength. This observation suggests that as the body is tilted backwards, intrinsic contractility of the knee extensor muscle tissue is increased. Assuming that all (or at least the same number of) muscle fibers in the knee extensors are activated by electrical stimulation in the four body positions, we can only hypothesize that perhaps calcium release or actomyosin interaction during contraction is altered by sagittal plane body position. However, we are unaware of precedence for such a mechanism under a similar scenario and thus consider this to be an unlikely possibility. Intuitively, it would seem more plausible that our observed sagittal body position effect on MVIC strength would be due to a vestibular effect on central activation and/or muscle/nerve tissue excitability during MVIC. We recommend that future studies consider probing the possibility.
Limitations
Several limitations must be addressed. First, the distinct varying tilting angles were selected mainly to examine the effects of changing body positions on knee extensor muscle function. These titling angles do not represent the best/worst seating position(s) when assessing knee extensor muscles. While we had ensured that all subjects were well secured during testing, it is still possible that stabilizations of the subjects to the testing chair were not the most ideal, particularly when the subjects were tilting forward (i.e., facing downward), thereby potentially affecting their abilities to perform the knee extensor muscle testing. Lastly, the present study combined both men and women into analyses because we did not intend to compare men to women. Our use of repeated measures study design and significant results/findings of the corresponding statistical analyses would suggest comparable responses in men and women to the changes in body position. Specifically, if men and women demonstrated different responses (e.g., increased performance in men but decreased performance in women when the body was tilted forward or backward), it would likely result in non-significant results instead. However, given our uneven and small samples in women and men, we were unable to fully test this premise through proper statistical analyses that compared men to women. Future studies with sufficient sample sizes of men and women will be needed to examine whether men may respond differently than women in terms of the knee extensor strength and activations under varying seated positions.
Conclusions
Strength training of the knee extensors, either through voluntary contraction or electrical stimulation, has been commonly prescribed to patients with knee injuries such as knee ligament or meniscus tears, cartilage degeneration, and patellofemoral pain syndrome. Our findings suggest that placing an individual in a semi-reclined sitting position can assist in obtaining a more forceful contraction of the knee extensor muscle group. Presumably, this would result in a better strength training outcome. Finally, we are unable to provide a definitive physiological mechanism for the sagittal body position effect on MVIC and electrically-evoked strengths.
Footnotes
Conflict of interest
The authors declare no conflict of interest.