
Abstract
Purpose:
To determine the effects of cryotherapy on quadriceps electromyographic (EMG) activity and isometric strength in early postoperative knee surgery patients.
Methods:
Twenty-two volunteers with recent knee surgeries were included. EMG readings of the vastus medialis (VM), rectus femoris (RF), and vastus lateralis (VL) from the surgical leg were collected during a maximal voluntary quadriceps setting (QS) activity. Maximum isometric knee extension force measurements were also recorded. Subjects were randomly assigned to receive an ice bag or a sham room-temperature bag to the front of their postsurgical knee for 20 min. After treatment, the subjects repeated the above mentioned maximum QS and isometric knee extension force measurements. The subjects returned 24 h later to conduct the same test protocol but received the treatment (ice or sham) not applied during their first test session.
Results:
A 38% increase in VM EMG activity during QS and a 30% increase in maximum isometric knee extension strength were found after cryotherapy treatment. No significant differences were found in RF or VL EMG activity during QS after cryotherapy. No significant differences were found in any measurements after the sham treatment.
Conclusion:
Clinicians should consider applying ice to knee joints prior to exercise for patients following knee surgery with inhibited quadriceps.
Introduction
Arthrogenic muscle inhibition of the quadriceps is commonplace after knee surgery. 1 –4 Arthrogenic muscle inhibition is a presynaptic, ongoing reflex inhibition of musculature surrounding a joint after distension or damage to the joint structures. 5 While pain and disuse are considered primary reasons for inhibition, arthrogenic muscle inhibition results from activity from many different joint receptors, which act on inhibitory interneurons synapsing on the motor neuron pool of joint musculature. 5 Mechanoreceptor activity may be most responsible for muscle inhibition. Quadriceps inhibition may occur from damage to articular mechanoreceptors which causes abnormal joint afferent input that decreases excitability of the spinal neurons controlling quadriceps activity. 6
Arthrogenic muscle inhibition is a limiting factor in joint rehabilitation, because it delays active exercise necessary for healing. 5 Reactivating patients’ inhibited quadriceps remains a primary objective in the early stages of postoperative knee surgery rehabilitation. Methods of reactivating inhibited quadriceps include volitional exercise, the use of electrical stimulation, and biofeedback. 7 –11 Cryotherapy may have a role in reactivating inhibited quadriceps. Hopkins et al. 9 observed that cryotherapy and transcutaneous electric neuromuscular stimulation decreased the inhibition of the vastus medialis (VM), and cryotherapy further facilitated the quadriceps motor neuron pool in artificially effused knees. The cryotherapy group experienced greater “disinhibition” or activation of the VM than the transcutaneous electric neuromuscular stimulation group with longer lasting effects. 9 Disinhibition is defined as “a return of some measure of recruitment to baseline or preinjury levels.” 12 Hopkins 12 later studied the effects of cryotherapy again in artificially effused knees. Consistent with earlier work, he observed that joint cryotherapy applied after knee effusion resulted in disinhibition of the quadriceps. 12
There is no consensus regarding the effects of cryotherapy on voluntary motor activity. Although the majority of authors have reported increases, 7,9,12 –17 others have reported decreases 9,18 –20 or no change 8,21,22 in muscle activity or force after muscle or joint cooling. 23 Differences in the site (muscle vs joint) of ice application, the type of measurement used, and the time that the measurement was taken (during or after cryotherapy treatment) contribute to the inconsistent results reported in the literature. 23 The use of ice or cryotherapy to assist with pain and inflammation is routine for knee surgery patients. 21,22,24 Yet, the effects of cryotherapy on inhibited quadriceps activity and strength in early postoperative knee patients have not been studied. We hypothesized that cryotherapy applied to the knee joint of early postoperative knee surgery patients would lead to an increase in quadriceps surface electromyographic (EMG) activity and isometric quadriceps strength.
Materials and methods
Subjects
Twenty-two (15 males and 7 females) Department of Defense beneficiaries (mean age = 22.2 ± 5.4 years) who had recent knee surgery (mean time of testing following surgery = 4.3 ± 2.1 days) volunteered to participate in this study. Subjects were eligible to participate if they had surgery within 10 days of the completion of data collection. Eligible surgical procedures included isolated anterior cruciate ligament reconstruction (ACL-R); ACL-R with meniscectomy; ACL-R with associated ligamentous and/or soft tissue injury such as the medial collateral ligament, lateral collateral ligament, and menisci not requiring surgical repair; and arthroscopic knee surgeries to include meniscectomy and/or meniscal debridement, plica excision, and patellar shaving. Subjects were excluded if they had the following: ligamentous repairs other than ACL-R, surgery with meniscal repair or allograft, osteochondral procedures, and nonsurgical knee pathologies.
Of the 22 subjects, 15 had ACL-R surgeries using the semitendinosus and gracilis in single or double-bundled fashion (9) or bone-patellar-tendon-bone (6) as a graft source. The remaining seven subjects had arthroscopic knee surgeries involving meniscal debridement. One subject with arthroscopic meniscal debridement also had a lateral retinacular release.
This study was approved by the Keller Army Community Hospital Institutional Review Board at West Point, New York. All subjects signed informed consent forms before participating, and the rights of all subjects were protected.
Design
This was a two-by-two repeated-measures design, with each subject tested to assess their response to a type of treatment (ice or no ice/sham) over time (pretreatment and posttreatment). The subjects participated in two separate data collection sessions randomly to evaluate the effects of ice and no ice/sham treatment on their quadriceps surface EMG activity and isometric knee extension strength. Statistical analysis was done using repeated-measure analysis of variance (ANOVA) comparing the pretreatment and posttreatment means of both quadriceps EMG activity and isometric strength with SPSS 11.5 for Windows (SPSS Corp. Chicago, Illinois, USA). Significance level was set at p < 0.05.
Quadriceps EMG recording and data analysis
The surface EMG measurements were collected using the Biopac MP100WSW system (BIOPAC Systems, Inc., Goleta, California, USA) and Bagnoli EMG System (Delsys Inc., Boston, Massachusetts, USA). The electrode sites were shaved and scrubbed with rubbing alcohol to prepare the skin. 25,26 Single differential Ag-AgCl bar electrodes (DE-2.1; Delsys Inc.) were positioned using an electrolyte gel and adhesive skin interfaces at a fixed interelectrode distance of 1 cm. 27 The reference electrode was attached to the medial malleolus of the nonsurgical leg. EMG data were collected for the following muscles of the surgical leg: VM (two finger breadths proximal to the superomedial border of the patella along the assumed line of the fibers), rectus femoris (RF; midway along a line between the anterior superior iliac spine and the superior pole of the patella), and vastus lateralis (VL; four finger breadths proximal to the superolateral border of the patella along the assumed line of the fibers). 1 The three sites were marked with a skin marker prior to electrode placement to duplicate placement during the second data collection session. The electrodes stayed in place for the duration of the test session. Pilot testing revealed that skin surface temperature measurements at the EMG electrode sites did not change during and after ice bag application, which was consistent with comparable studies. 9,12 Therefore, skin surface temperature was not monitored during testing.
The EMG sampling rate was 2000 Hz. The EMG signal was amplified with an overall gain of 1000 and digitized using Acqknowledge 3.7.2 software (BIOPAC Systems, Inc). Bandpass (20–500 Hz) and notch filters (60 Hz) were used. For testing of quadriceps muscle setting, the EMG signal was collected for 5 s during a maximal voluntary isometric contraction (MVIC), whereas the knee was fully extended (isometric action of muscles monitored). The root-mean-square (RMS) for three trials during the middle 3 s (first and last seconds discarded) of the 5-s MVIC was calculated for each muscle. The greatest value of the three consecutive attempts was then calculated for analysis. 27
Isometric quadriceps strength measurement and data analysis
Isometric quadriceps strength was measured with a Lafayette Manual Muscle Test System (NEXGEN Ergonomics Inc., Montreal, Quebec, Canada) hand-held dynamometer. Interrater reliability is good to high for measurements of knee extensor force obtained by handheld dynamometry. 28,29 The peak force measurement of an MVIC while attempting knee extension with the knee maintained at 70° flexion was collected for 5 s. Two 5-s trials were averaged for analysis.
Procedure
The enrolled volunteers reported to outpatient physical therapy to initiate postoperative knee rehabilitation per preestablished rehab protocols. As soon as the subjects acquired 70° of flexion in their surgical knee, not to exceed 10 days postsurgery, they participated in two separate 45-min data collection sessions. The separate sessions took place 24 h apart inside a quiet laboratory. The order of the testing was randomized with 14 of the 22 subjects receiving cryotherapy treatment during the first test session.
Subjects were seated with both knees fully extended on a padded table with their backs supported against a wall. The subjects’ knee girth measurements (in centimeter) were taken at the superior margin of the patella at the beginning of each session. Pain levels were recorded via a 10-point visual analog scale 30 to specifically evaluate subjective complaints after knee surgery. A practice period was held for all subjects at the beginning of each data collection session. This time was used to familiarize the subjects with the testing protocol and to practice maximal voluntary quadriceps setting (QS) and isometric knee extensions (three to five practice trials).
EMG measurements of the VM, RF, and VL from the surgical leg were collected during three trials of QS (Figure 1). Verbal commands of “ready,” “push,” and “stop” were given to the subjects. In performing the QS exercises, subjects were instructed to push the back of their surgical knee as hard as possible into the padded table that was under their knee until told to stop. Each QS trial lasted 5 s with 30 s rest between each trial. The subjects were instructed to relax while the data were being stored. After the three trials of QS, the subjects were asked to rate their pain on 10-point visual analog scale. 30 The subjects then sat at the edge of the padded table with their surgical leg in 70° of knee flexion (verified by a goniometer). A handheld dynamometer was placed over the anterior aspect of the subjects’ shins, just proximal to the ankle joint (Figure 2). Again using the verbal commands of “ready,” “push,” and “stop,” the subjects were instructed to extend their knee with maximal effort for 5 s with 30 s rest between two trials. The subjects were then asked to rate their pain on a 10-point visual analog scale. 30

Surface electromyographic measurements of the vastus medialis, rectus femoris, and vastus lateralis during quadriceps setting.

Maximum voluntary isometric contraction with the knee at 70° flexion.
The subjects then received either a 1.5 L crushed ice bag or a room-temperature bag (sham treatment—kitty litter) with the same consistency and weight as an ice bag to the front part of their postsurgical knee for 20 min. The bags were secured to the knee using an elastic ace wrap (Figure 3), which concealed the type of treatment to the blinded tester. Immediately after the cryotherapy or sham treatment, the abovementioned QS and isometric quadriceps strength testing was repeated using the same procedure as pretreatment. The subjects returned to the lab 24 h later to conduct the same test protocol with the treatment (ice or sham) that was not applied during the first test session. Between test sessions, the subjects continued their assigned home exercise programs (per preestablished rehabilitation protocols) consisting primarily of heel slides, QS, straight-leg raises, and calf pumps.

Setup of treatment application.
The subjects were blinded to the results of their measurements. The same tester collected all EMG measurements. The tester of the isometric strength testing using the handheld dynamometer was a different individual blinded to the type of treatment. After the second test session, the subjects were discharged from the study and resumed postoperative knee surgery rehabilitation.
Statistical analysis
A two-by-two repeated-measure analyses of variance (ANOVA) was performed to compare prequadriceps and postquadriceps EMG activity and isometric strength. The within-subject factors were treatment (two levels: ice or no ice/sham treatment) and time (two levels: pretreatment and posttreatment). Paired t-tests were computed for knee girth and the Wilcoxon signed-ranks test was used for visual analog scale pain scores. Wilcoxon signed-ranks test was used for pain data. A statistical significance level was set at p < 0.05.
Results
Means and standard deviations for quadriceps EMG activity and isometric strength are provided in Tables 1 and 2. VM EMG activity increased significantly after cryotherapy treatment (F 1, 21 = 5.922; p ≤ 0.024). There was no significant difference in VM EMG activity between pre-sham and post-sham treatment (F 1, 21 = 0.047; p = 0.530). Likewise, no significant differences were found in RF and vastus lateralis (VL) EMG activity between precryotherapy and postcryotherapy (RF: F 1, 21 = 1.864; p = 0.187; VL: F 1, 21 = 0.186; p = 0.670) or pre-sham and post-sham treatments (RF: F 1, 21 = 0.284; p = 0.600; VL: F 1, 21 = 2.528; p = 0.127).
Electromyographic activity during maximum quadriceps setting.a
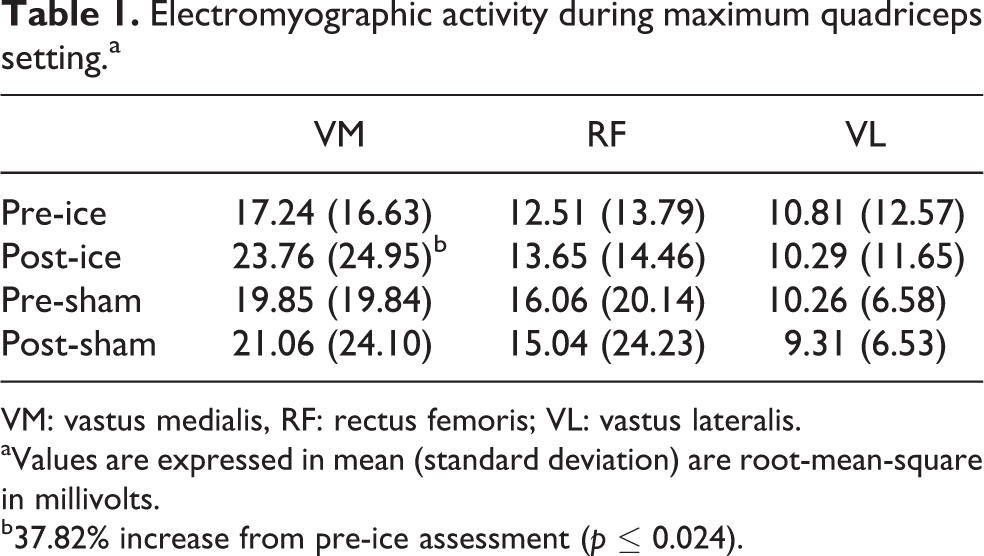
VM: vastus medialis, RF: rectus femoris; VL: vastus lateralis.
aValues are expressed in mean (standard deviation) are root-mean-square in millivolts.
b37.82% increase from pre-ice assessment (p ≤ 0.024).
Isometric quadriceps peak force.a

aValues are expressed in mean (standard deviation).
b29.86% increase from pre-ice assessment (p ≤ 0.0001).
Quadriceps isometric knee extension strength increased significantly after cryotherapy treatment (F 1, 21 = 31.097; p ≤ 0.0001). No significant difference in quadriceps isometric knee extension strength was found between pre-sham and post-sham treatment (F 1, 21 = 3.743; p = 0.067). With respect to knee girth, the difference between involved and noninvolved lower extremities for the two testing days was not significantly different (mean differences between involved and noninvolved lower extremities of 3.3 ± 1.5 cm for testing session 1 and 3.5 ± 1.4 cm for testing session 2). There were also no significant differences in pain levels during each test session or between test days (Table 3).
Pain levels that were recorded via a 10-point visual analog scale.

QS: quadriceps setting.
Discussion
The results of this study support our hypothesis stating cryotherapy applied to the knee joint of early postoperative knee surgery patients leads to an increase in quadriceps surface EMG activity and isometric quadriceps strength. Consistent with previous studies, 9,12 we observed that knee joint cryotherapy actually had a disinhibitory effect on the inhibited quadriceps. While Hopkins et al. 9,12 used an experimental knee joint effusion model, our study included patients in the early postoperative phase. The reason why knee joint cryotherapy disinhibits the quadriceps is not fully understood. Arthrogenic muscle inhibition is associated with afferent stimuli from the knee joint 31 and occurs when sensory stimuli impede the voluntary activation of the muscle. 32 Certain sensory stimuli can block other afferent sensory stimuli in the spinal cord. Cutaneous sensory nerve stimulation can increase motor neuron excitability. 9,31 Cryotherapy might reduce quadriceps inhibition by preventing the activation of inhibitory synapses and/or by increasing the excitability of the anterior horn cells. 31 Cryotherapy may result in less supraspinal control over reflexive activity and more recruitment within the quadriceps motor neuron pool. 12
While pain and effusion may have a role in quadriceps inhibition in postoperative knee patients, we observed no difference in knee girth measurement between test days or for pain level during each test session (pretreatment vs. posttreatment) or between test days. Previous studies have demonstrated, using the artificial knee joint effusion model, that arthrogenic muscle inhibition can occur in the absence of pain. 9,33 Based on our findings, we are in agreement with Hopkins et al. 9,22 that cryotherapy has a direct effect on diminishing arthrogenic muscle inhibition and not just pain.
The use of cryotherapy to specifically diminish arthrogenic muscle inhibition or disinhibit muscles is not widely studied or commonly practiced among rehabilitation professionals. During rehabilitation, cryotherapy is most commonly used after active exercise because of its well-documented local physiological responses of decreased temperature, metabolism, inflammation, circulation, pain, and muscle spasm. 34 However, using joint cryotherapy to assist in the reactivation of inhibited muscles is an unconventional, yet promising, concept in clinical application. 9,12,23 The opportunity to assess patients in the early phase following knee surgery in this study is clinically relevant. Our findings, combined with the work of Hopkins et al., 9,12,23 are pertinent to actual patients seen in rehabilitation settings.
Sixty-eight percent (15 of 22) of the subjects received ACL-R surgeries. The scarcity of existing literature regarding the early postoperative strength testing of patients following ACL-R suggests that maximal isometric quadriceps testing in these patients may be unsafe and might compromise the surgical grafts. But according to Beynnon et al., 35 –37 isometric quadriceps strength measurement is safely attainable for patients following ACL-R, if the patients are tested between 60° and 90° of knee flexion. Based on these findings, we felt testing at 70° knee flexion was safe for our subjects. All 22 enrolled subjects completed data collection without adverse events or effects.
The VM was the only portion of the quadriceps that we found a difference in EMG activity after cryotherapy. This difference may be due to the VM being the most affected portion of quadriceps from arthrogenic muscle inhibition. While common belief and clinical observation suggest that the VM is more inhibited than the other heads of the quadriceps after joint injury, 5,31 recent data indicate uniform weakness, atrophy, and deactivation of the quadriceps after joint injury. 38,39
QS is a primary exercise assigned to patients with inhibited quadriceps. Generally in most rehabilitation settings, QS is done by forcefully contracting the quadriceps with the knee in maximum extension. It has been suggested that QS should be performed with the knee in a position of some flexion (approximately 30°) to avoid inhibition of the muscle. 32,40 The decision to conduct QS during this experiment in full extension was based on the authors’ intent to keep the testing protocol consistent with general clinical practice. Each subject’s postsurgical knee range of motion was measured and verified to be at least 0–70 prior to each test session. However, each subject’s postsurgical knee extension was not compared to their nonsurgical knee range of motion. Therefore, symmetrical bilateral knee extension, and potentially hyperextension, was not verified at the time of testing. Lacking knee hyperextension (if hyperextension is normal) may contribute to decreased quadriceps activation during quadriceps setting. 41,42 Whether or not the subjects’ surgical knee range of motion would have changed between pretreatment and posttreatment and between testing days is questionable. The time it takes for postsurgical knee patients to reacquire knee hyperextension, if normal, is patient specific and highly variable. After a subsequent review of the subjects’ medical records, we found no documentation of genu recurvatum or knee hyperextension in any of the subjects’ bilateral knees. Retrospectively, the subjects’ nonsurgical knee range of motion should have been verified at the time of testing.
With a repeated-measures design with testing sessions separated by 24 h, it is fairly safe to assume that subject characteristics (i.e. pain, motivation) and testing conditions (i.e. time of day, room temperature) remained constant throughout the course of this experiment. Therefore, differences seen among treatment conditions are more likely to reflect treatment effects and not variability between subjects. 43 Of the quadriceps inhibition and EMG studies reviewed, gender differences among the subjects either did not exist or were not mentioned. 1,9,12,26,40,44 –50 One disadvantage of a repeated-measure design was the potential for practice effects. 43 The additional data collection day to evaluate the effects of no ice/sham treatment helped to minimize practice effects in this study. The order of testing, QS followed by isometric quadriceps test at 70°, was not randomized. We assumed that isometric quadriceps extension testing would be uncomfortable for early postoperative knee patients, which might have resulted in subjects’ effort being affected during ensuing QS.
Relatively high standard deviations were observed in the EMG activity scores during QS. This finding is consistent with similar EMG studies. 12 Variance in subjects’ EMG scores in our study was not surprising, because the subjects were not expected to demonstrate equal levels of quadriceps inhibition after knee surgery. We observed significant differences only in VM EMG activity and overall isometric quadriceps strength after cryotherapy. Our relatively sample size of only 22 subjects may have contributed to not finding a difference in the RF and VL after cryotherapy and in all muscles after the sham treatment. Our clinically meaningful effect size was a 15% increase in both quadriceps EMG activity and isometric strength, which was exceeded in this study for VM EMG activity and overall isometric quadriceps strength after cryotherapy. A few of the measurements approached significance including RF EMG activity postcryotherapy (p = 0.187), VL EMG activity post-sham (p = 0.127), and isometric strength post-sham (p = 0.067). Yet, all these measurements showed small differences that are not considered clinically meaningful.
Our results cannot be generalized to all populations, because 19 of the 22 subjects who participated in this study were healthy young military cadets. The remaining subjects (two males, ages 29 and 41; one female, age 33) were active, healthy military members. The changes seen in VM EMG activity and isometric knee extension strength after icing the postoperative knee joints of individuals with quadriceps inhibition should be confirmed in other patient populations. Also, we did not investigate the parameters of how long to ice the joint nor how long the disinhibitory effects of cryotherapy last. Our sample was also somewhat heterogeneous. While all of the subjects in this study had pain and joint effusion, the degree of pain and joint effusion may vary among patients and the different surgical procedures which would influence muscle recruitment and strength. Future research should include randomized clinical trials comparing outcomes of patients following knee surgery who receive cryotherapy to their knee joints prior to active exercise to matched control groups. Also, the selective inhibition of the VM in patients following knee surgery and the effects of cryotherapy solely on VM inhibition and reactivation warrant further investigation.
Conclusion
This study examined the immediate effects of cryotherapy on quadriceps EMG activity and isometric strength in patients following knee surgery in the early post-operative phase. Our results indicate that cryotherapy applied to the knee joint leads to an increase in VM EMG activity and quadriceps isometric strength. Rehabilitation clinicians should consider the use of ice prior to active exercise for knee surgery patients with inhibited quadriceps.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.