Previous in vitro studies have indicated that pyrimidinergic receptor P2Y (P2RY6, P2Y receptor) may function as a cancer-promoting factor in lung adenocarcinoma (LUAD). However, the prognostic significance of P2RY6 expression in LUAD has not been investigated.
OBJECTIVE:
This study aimed to assess the impact of P2RY6 expression on the survival of patients with LUAD.
METHODS:
First, we assessed P2RY6 mRNA and protein expression in LUAD and non-cancerous lung tissues using the online bioinformatics analysis tool GEPIA, fresh LUAD tissues, and LUAD tissue microarrays (TMAs). Second, we investigated the correlation between P2RY6 expression and clinicopathological parameters of LUAD patients based on data from The Cancer Genome Atlas (TCGA) database and TMAs. Finally, we analyzed the prognostic significance of P2RY6 expression in LUAD using the online survival analysis tool Kaplan-Meier Plotter and data from TMAs.
RESULTS:
We demonstrated that P2RY6 mRNA and protein expression levels in LUAD tissues were significantly higher than those in non-cancerous lung tissues. The expression of P2RY6 in LUAD was positively correlated with poor differentiation, more lymph node metastasis, and more advanced clinical stage. Higher P2RY6 expression level was correlated with shorter survival of the LUAD patients. Univariate and multivariate Cox regression analyses indicated that higher P2RY6 tumor expression was an independent unfavorable prognostic factor for LUAD patients.
CONCLUSIONS:
P2RY6 expression was elevated in LUAD and correlated with poor prognosis.
Lung cancer is the leading cause of cancer mortality worldwide [1]. Non-small cell lung cancer (NSCLC) accounts for 80% of lung cancer cases, of which approximately 50% are lung adenocarcinoma (LUAD) [2, 3]. Despite the therapeutic advances made over the last few decades, the improvement in the overall survival (OS) of lung cancer patients remains limited [4]. Therefore, novel prognostic markers and therapeutic targets are urgently needed to improve the survival of patients with LUAD.
Although data-driven computation strategies have made great advances in biomarker discovery for LUAD [5, 6, 7], the traditional molecular mechanism-driven approach based on the current biological understanding of LUAD remains useful for identifying new biomarkers [8, 9]. Receptors recognizing ATP and relative purine and pyrimidine nucleotides and nucleosides are called purinergic receptors and contain two major families, P and P purinoceptors. P purinoceptor is selective for adenosine, including A, A, A, and A subtypes, and is involved in the modulation of cardiovascular, immune, and central nervous system activities, while the P purinoceptor contains two subgroups, namely P2X ligand-gated ion channels and P2Y G-protein coupled receptors. The P2Y receptors can be further grouped into the Gq protein-coupled P2Y-like subfamily, comprising P2Y, P2Y, P2Y, and P2Y receptors, the Gi protein-coupled P2Y-like subfamily, comprising P2Y receptors, and the Gs protein-coupled subfamily P2Y receptor [10]. The interactions between these receptors and their corresponding ligands are extensively involved in the physiological, pathophysiological, or pharmacological regulatory mechanisms of the nervous, endocrine, cardiovascular, immune, pulmonary, and musculoskeletal systems [10]. Moreover, accumulating evidence has demonstrated that activation of P2Y receptors also promotes proliferation, migration, metastasis, and therapeutic resistance in multiple cancer types [11, 12, 13].
Among the P2Y receptors, P2Y and P2Y are characteristic of UDP receptors. The interaction of P2Y receptor with UDP is particularly important in regulating tumor formation and metastasis, such as that in colorectal [14], breast [15], and pancreatic cancer [16]. In colorectal cancer, activation of P2Y receptor was found to accelerate proliferation, inhibit apoptosis, promote migration, and induce chemotherapeutic resistance of tumor cells [14, 17, 18], while in breast cancer, the interaction of UDP and P2Y receptor was also reported to induce epithelial–mesenchymal transformation and metastasis [15, 19]. These reports suggested a cancer-promoting characteristic of P2RY6 in certain cancer types.
In lung cancer, P2Y receptor was reported to be involved in extracellular nucleotide-induced proliferation and migration of A549 human LUAD cells [18, 20]. Moreover, activation of P2Y receptor in A549 cells was also reported to amplify the cellular repair responses to DNA damage caused by gamma irradiation, suggesting a radiotherapeutic resistance potential of P2Y receptor in lung cancer [21, 22]. Additionally, a large-scale functional genetics study also showed that P2RY6 is a drug-resistant driver of ALK (anaplastic lymphoma kinase) inhibition in lung cancer [23]. All this evidence supports P2RY6 function as a cancer-promoting gene in LUAD. However, most of these results were derived from in vitro studies using lung cancer cell lines. To our best knowledge, the prognostic significance of P2RY6 expression in primary LUAD remains uninvestigated. In this study, we compared the expression of P2RY6 between LUAD and non-cancerous lung tissues, analyzed the correlation between the expression of P2RY6 in LUAD and clinicopathological variables, and tested the impact of P2RY6 expression on the prognosis of LUAD patients by univariate and multivariate survival analysis.
Material and methods
Tissue samples and TMAs
Eleven fresh surgically resected LUAD and corresponding paracancerous tissue samples (seven males and four females; age range, 57–76 years) were collected from the Longnan Hospital of Daqing (Daqing, China) from 2019 to 2020, and no chemotherapy or radiotherapy was received before the surgery. After sufficient tissue was reserved for pathological diagnosis, the surplus resected tissues were stored immediately in liquid nitrogen for exaction of mRNA and protein. The storage time of the 11 fresh tissue samples in liquid nitrogen ranged from 3 days to 8 months. Use of these samples was approved by the ethical institution of Longnan Hospital of Daqing, and written informed consent was obtained from all participants.
Two LUAD tissue microarrays (TMA) chips (cat. #HlugA180Su03 and cat. #HlugA180Su06) were purchased from Outdo Biotech Co. Ltd (Shanghai, China). The two TMAs contained 186 cases of human LUAD (104 males and 84 females; age range, 20–86 years). Among the 186 cases, 163 had validated OS information. The follow-up period of the patients ranged from 1 to 120 months, and the median follow-up was 39 months. Patient information including tumor differentiation, pathological T-size, pleural invasion, lymph node metastasis, and clinical stage was obtained from the data sheet provided by the TMA supplier. All samples were collected from treatment-naïve patients. Ethical approval for the use of the TMAs was provided by the TMA supplier.
The protocol of this study was approved by the Institutional Review Board of Harbin Medical University-Daqing (approval number: HMUDQ2020091503). All procedures were conducted in accordance with the Declaration of Helsinki (7 version, 2013) and the International Ethical Guidelines for Biomedical Research Involving Human Subjects.
RNA extraction, reverse transcription, and real-time qPCR
Total RNA was extracted from fresh LUAD and corresponding paracancerous tissues with TRIzol reagent (Invitrogen Life Technologies) and then treated with DNase (Roche). First-strand cDNA was synthesized with M-MLV transcriptase (Promega) and oligo dT. Real-time quantitative PCR (RT-qPCR) was performed using SYBR Green PCR master mix kit (Takara Bio, Inc.) on a real-time PCR instrument (LC-480, Roche) for 40 cycles. The following primer sequences used for amplifying P2RY6 in Akhtari et al. [24] were adopted: 5-GTGTCTACCGCGAGAACTTCA-3 (forward), 5-CCAGAGCAAGGTTTAGGGTGTA-3 (reverse); pri- mers for ACTB were 5-GGACTTCGAGCAAGAGATGG-3 (forward) and 5-ACATCTGCTGGAAGGT-GGAC-3 (reverse). Melting curves were used to determine the specificity of the amplifications. Relative cDNA levels were normalized against ACTB and calculated using the 2 method. Each PCR amplification was performed in triplicate.
Protein extraction and western blotting
Total protein was extracted from fresh LUAD and corresponding paracancerous tissues by homogenizing the tissues in RIPA lysis buffer (radioimmunoprecipitation lysis buffer). After centrifugation at 12,000 for 20 min, the supernatant was mixed and denatured with Laemmli sample buffer. A total of 50 g protein from each sample was submitted to sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) and then transferred onto nitrocellulose membranes. The membranes were then blocked in 5% skimmed milk and washed thrice with Tris-buffered saline containing 0.05% Tween 20 (TBS-T). Subsequently, the membranes were probed with antibodies against P2Y receptor (Affinity Biosciences cat. #DF6956, RRID: AB_2838912, 1/1000) or -actin (Santa Cruz, cat. #sc-69879, 1/5000) at 4C overnight, and then incubated with the appropriate secondary antibodies for 1 h. Finally, the bands on the membranes were visualized with enhanced ECL reagent and quantified with the NIH Image J program for analysis. Endogenously P2Y receptor low-expressing SH-SY5Y human neuroblastoma cells and endogenously P2Y receptor high-expressing A549 human lung adenocarcinoma cells were used as negative and positive controls, respectively, to determine the selectivity of the antibody.
Immunohistochemistry
Immunostaining for P2Y receptor on TMA sections was performed according to the immunohistochemistry (IHC) protocol described previously [25]. Briefly, the TMA sections were first deparaffinized and rehydrated with xylene and alcohol gradients, then quenched for endogenous peroxidase with 3% hydrogen peroxide-methanol for 30 min. Antigen retrieval was performed by heating the sections by microwaving (500 W) for 15 min in 10-mM citrate buffer (pH6.0) prior to incubation of the sections with polyclonal antibody against P2Y receptor (Affinity Biosciences cat. #DF6956, RRID: AB_2838912, 1/200) at 4C overnight. A two-step IHC detection kit (Zhongshan Golden Bridge Biotechnology, cat. #PV-9000) was used instead of a traditional secondary antibody system according to the manufacturer’s protocol and the sections were finally visualized with the chromogen DAB and counterstained with hematoxylin. A colorectal cancer specimen with definite P2Y receptor protein expression was used as positive control, while a negative control was conducted by omitting the primary antibody in the antibody dilution buffer.
P2Y receptor immunoreactivity was evaluated independently by two of the authors (BSZ and JBL) who were blinded to the clinical and follow-up data of the patients. The percentage of positive cells (none 0; 10% 1; 11%–50%, 2; 51%–75% 3; 76%–100% 4) and staining intensity (none 0; weak 1; intermediate 2; and strong 3) were assessed. A final immunoreactivity score ranging from 0 to 12 was calculated by multiplying the intensity with the percentage score for each core. Cores with scores of 4 were classified as P2Y-High and those with scores of 4 as P2Y-Low.
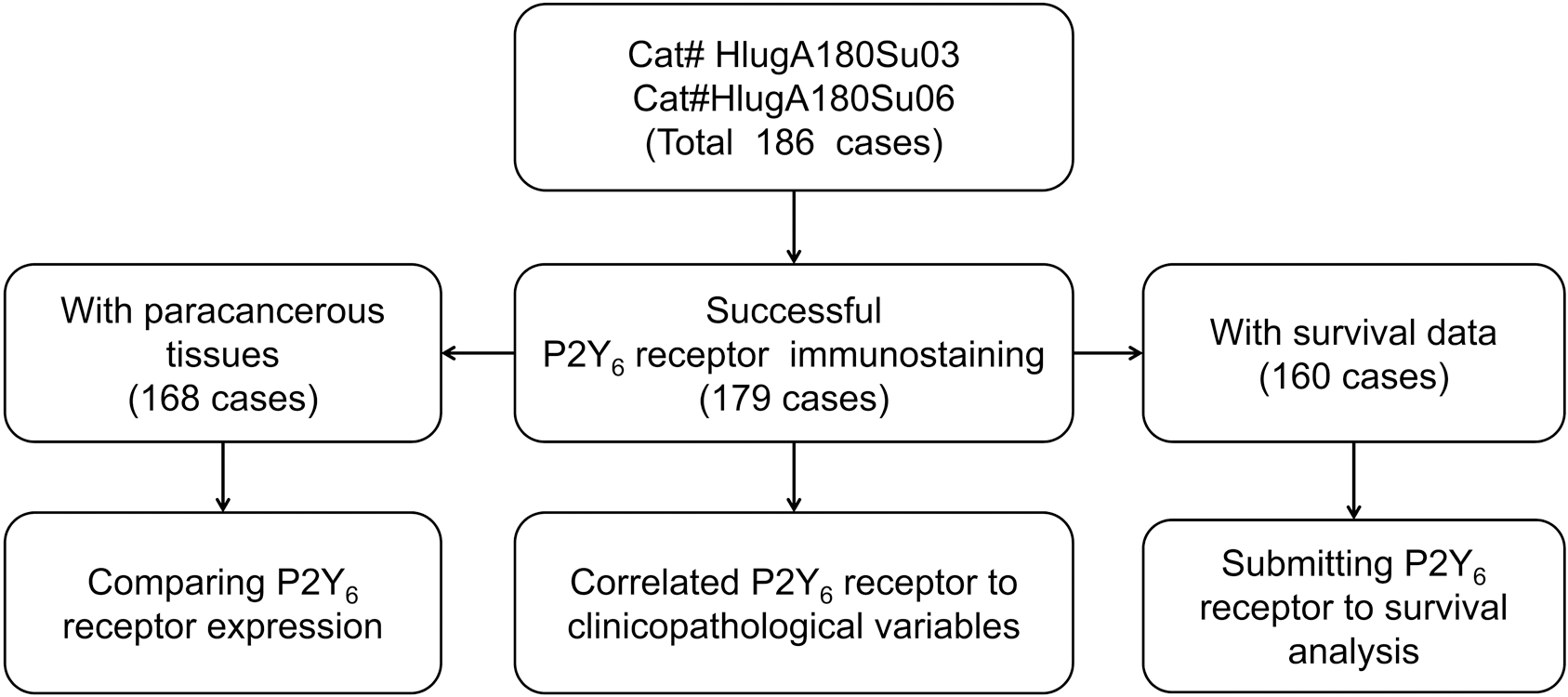
Analytic procedures of P2Y receptor immunostaining on LUAD TMA.
Among the total 186 TMA cases, scoring of P2Y receptor immunoreactivity in 7 cases was unavailable because of the detachment of the tissues during IHC. Of the 179 LUAD specimens that were successfully immunostained, 168 cases had corresponding paracancerous tissues, and 160 cases had OS information. These samples were submitted to subsequent comparison, correlation, or survival analyses, respectively (Fig. 1).
Bioinformatics analysis
GEPIA (http://gepia.cancer-pku.cn/) was used to explore the expression difference of P2RY6 between LUAD and non-cancerous lung tissues [26]. Kaplan–Meier Plotter (http://kmplot.com) [27] was applied to preliminarily analyze the correlation between P2RY6 expression (Affymetrix ID: 208373_s_at) and survival of the LUAD patients. Before running the Kaplan-Meier analysis, the parameters were set as following: “Only JetSet best probe set” was chosen for the probe setting, “Auto select best cutoff” was chosen for splitting patients, and array quality control was set to “exclude biased array”.
Statistical analysis
Student’s -test was used to compare the mRNA and protein levels of P2RY6 between fresh LUAD and corresponding paracancerous tissues. Chi-squared test was used to compare P2Y receptor expression between LUAD and corresponding paracancerous tissues in TMAs and to determine the correlation between P2Y receptor expression and clinicopathological variables. Kaplan-Meier analysis and log-rank test were used to evaluate the correlation of P2RY6 expression and OS of the patients. Univariate and multivariate Cox regression analyses were used to assess the prognostic impact of P2RY6 in predicting survival outcome. Survival-related statistical analyses were conducted using SPSS 19.0, while other statistical tests were performed with GraphPad Prism 6; two-sided -values of 0.05 were considered significant.
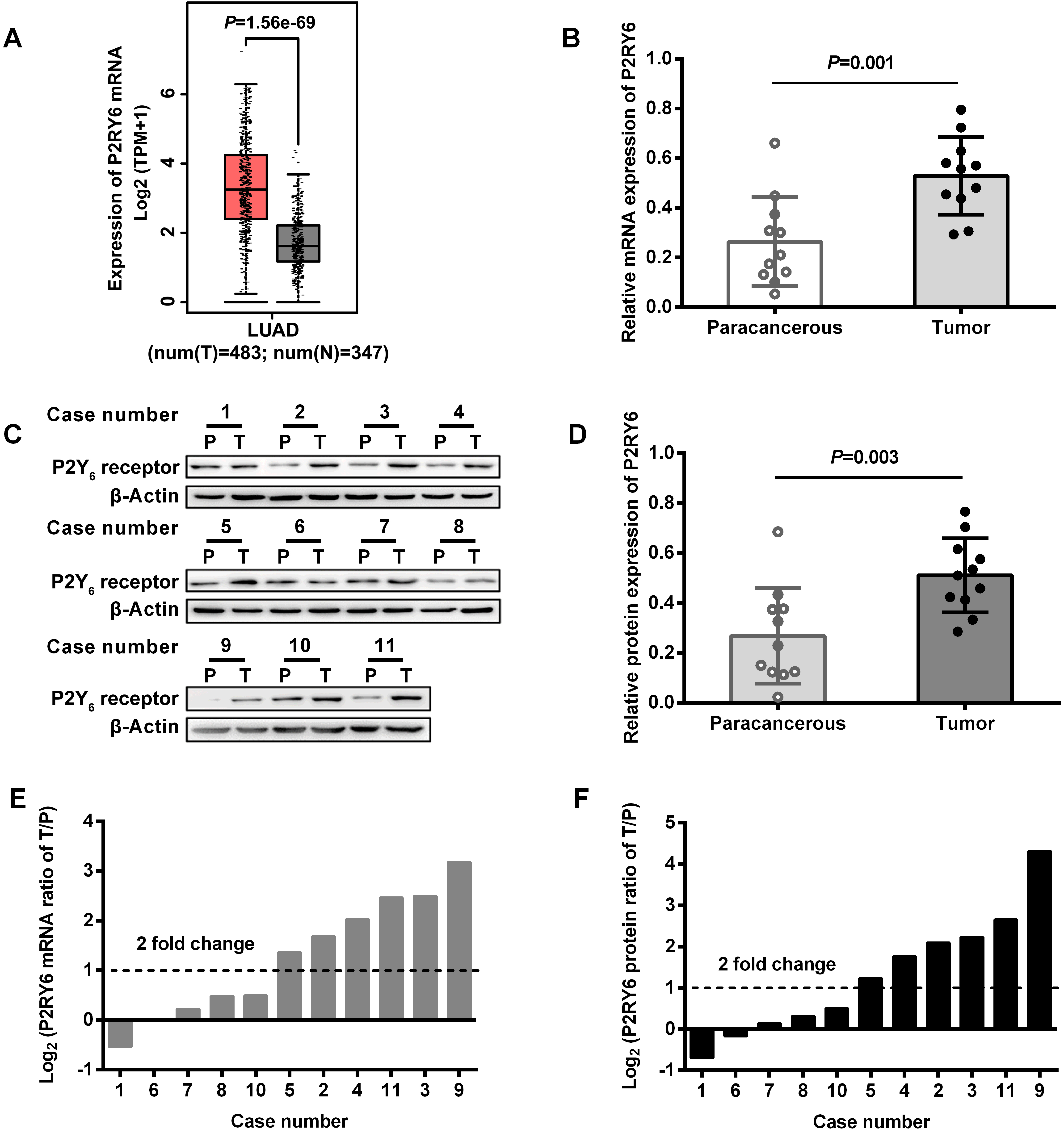
Overexpression of P2RY6 in LUAD. (A) Bioinformatics comparison of P2RY6 mRNA in LUAD to that in non-cancerous lung tissue using GEPIA. (B–F) the mRNA and protein levels of P2RY6 in 11 cases of fresh LUAD and corresponding paracancerous tissues were examined by RT-qPCR and Western blots. (B) Overall P2RY6 mRNA expression in LUAD was compared to that in corresponding paracancerous tissues. (C) Western blots of P2Y receptor in LUAD tumor (T) and corresponding paracancerous (P) tissues. (D) The protein level of P2Y receptor was quantified with ImageJ software and overall P2Y receptor protein expression in LUAD was compared to that in corresponding paracancerous tissues. (E) Log (P2RY6 mRNA level in tumor/that in corresponding paracancerous tissues) was calculated; cases with number of 2, 3, 4, 5, 9, 11 demonstrated more than 2-fold change of P2RY6 mRNA. (F) Log (P2Y receptor protein level in tumor/that in corresponding paracancerous tissues) was calculated; cases with number of 2, 3, 4, 5, 9, 11 demonstrated more than 2-fold change of P2Y receptor protein.
Results
P2RY6 expression was elevated in LUAD
P2RY6 mRNA expression was first compared between LUAD and non-cancerous lung tissue with GEPIA, which combined data from TCGA and GTEx databases containing 483 LUAD and 347 non-cancerous lung tissues. P2RY6 mRNA levels in LUAD were significantly higher than those in non-cancerous lung tissues (Fig. 2A). To verify this in silico result, the mRNA and protein levels of P2RY6 in 11 pairs of fresh LUAD and corresponding paracancerous tissues were examined by RT-qPCR and western blotting. Both P2RY6 mRNA and protein expression in fresh LUAD tissues were significantly higher than those in paracancerous tissues (Fig. 2B–D). Among individuals, 6 of the total 11 cases showed a more than 2-fold elevation of P2RY6 mRNA and protein expression in LUAD compared with the corresponding paracancerous tissues (Fig. 2E and F).
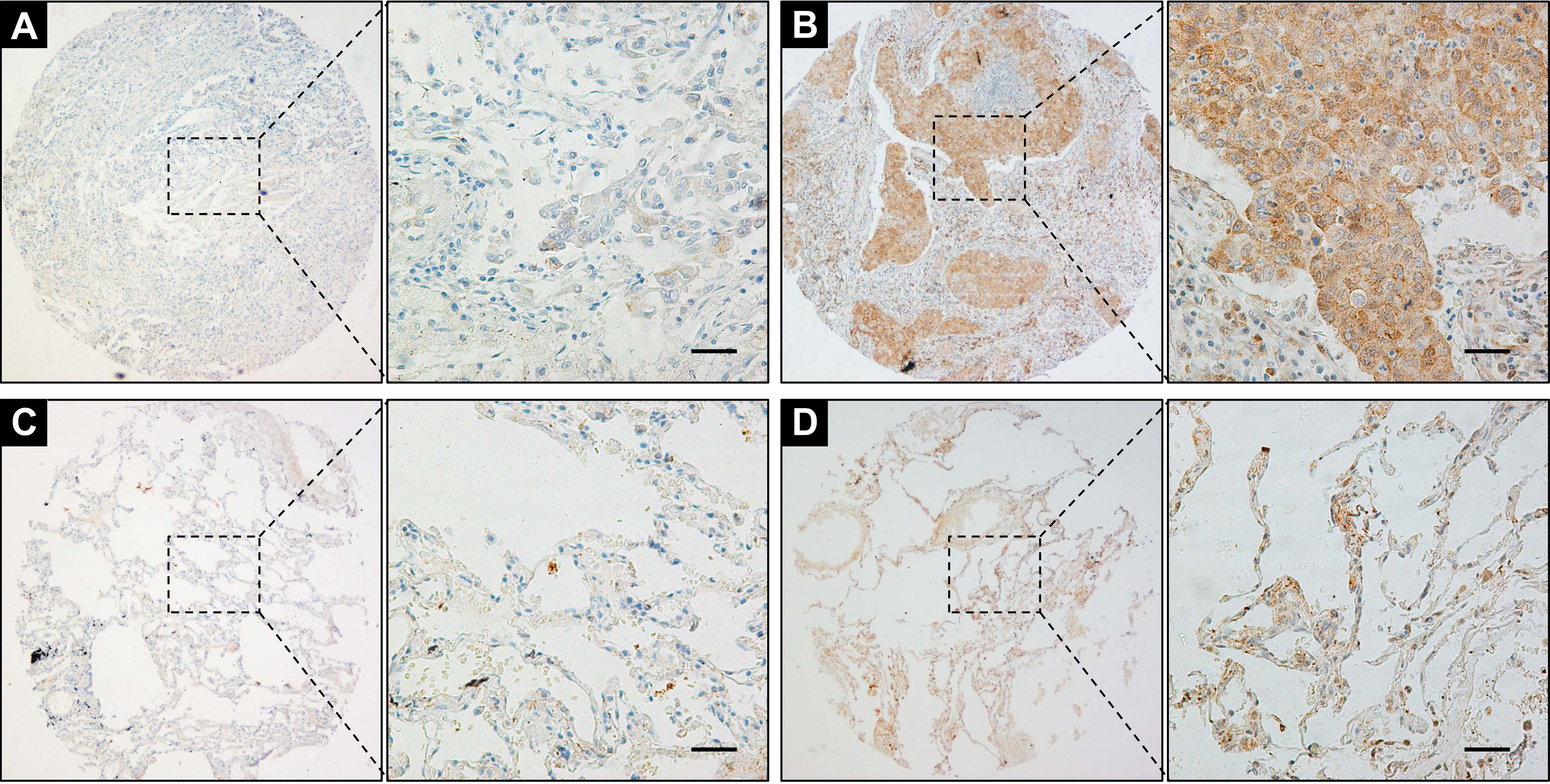
Detecting P2Y receptor expression in LUAD by IHC. (A) Low P2Y receptor immunostaining in LUAD tumor tissue. (B) High P2Y receptor immunostaining in LUAD tumor tissue. (C) Low P2Y receptor immunostaining in paracancerous tissue. (D) High P2Y receptor immunostaining in lung epithelium and lymphocytes in paracancerous tissue. Scale bar 50 m.
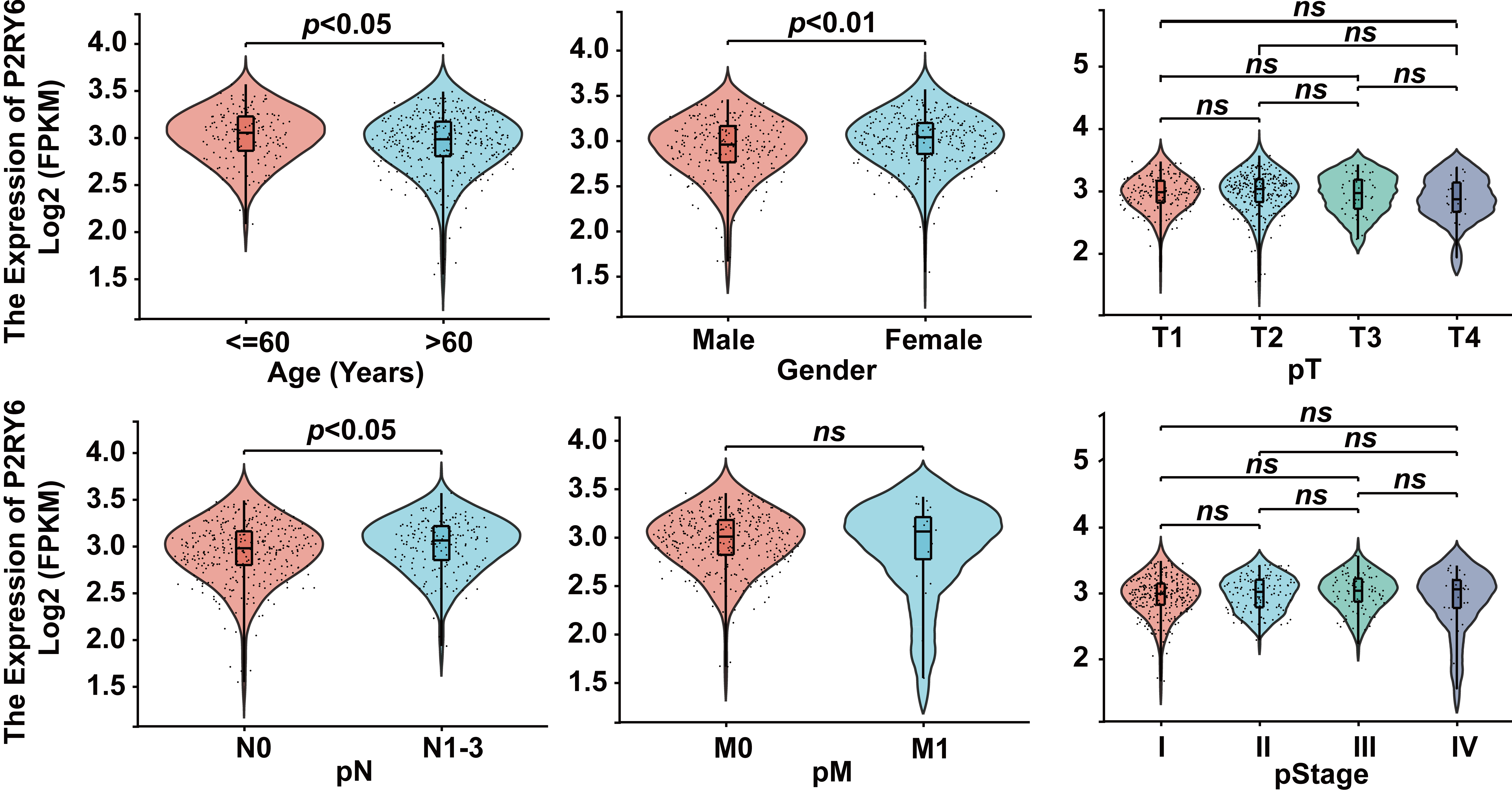
Correlating P2RY6 mRNA level to the clinicopathological variables of the LUAD patients using TCGA data.
We further performed IHC to detect the protein expression of P2Y receptor in TMAs containing 168 LUAD and corresponding paracancerous tissues. In the LUAD tissues, P2Y receptor-positive staining was mainly located in the cytoplasm of tumor cells. In some cases, moderate positive staining of P2Y receptor could also be found in a few stromal fibroblast cells or lymphocytes (Fig. 3A and B), while 65/168 cases (38.7%) showed low P2Y receptor expression and 103/168 cases (61.3%) showed high P2Y receptor expression. Furthermore, in the paracancerous tissues, P2Y receptor demonstrated negative or moderate positive staining in the cytoplasm of a few epithelial lung cells and scattered lymphocytes (Fig. 3C and D), while 132/168 cases (78.6%) showed low P2Y receptor expression and 36/168 cases (21.4%) showed high P2Y receptor expression. P2Y receptor expression in LUAD was significantly higher than that in paracancerous tissues ( 55.082, 0.001).
Correlation between P2RY6 expression and clinicopathological variables in LUAD
The correlation between P2RY6 mRNA levels in LUAD and clinicopathological variables of the patients was preliminarily tested using data from TCGA. It demonstrated that tumor P2RY6 mRNA levels in patients who were female, younger ( 60 years), or with higher-grade pathological lymph node metastasis (pN) were relatively higher than those in their counterparts. However, no significant correlation was found between P2RY6 mRNA levels and pathological tumor size (pT), pathological distal metastasis (pM), and pathological stage (pStage) (Fig. 4).
Correlation between P2Y receptor expression and clinicopathological variables of LUAD patients
Variables
Immunoreactivity of P2Y receptor
Low
High
Gender
Male
101
41 (40.6%)
60 (59.4%)
0.013
0.908
Female
78
31 (39.7%)
47 (60.3%)
Age
60
85
38 (44.7%)
47 (55.3%)
1.353
0.245
60
94
34 (36.2%)
60 (63.8%)
Tumor differentiation
Good
18
10 (55.6%)
8 (44.4%)
7.094
0.029
Moderate
139
57 (41.0%)
82 (59.0%)
Poor
20
3 (15.0%)
17 (85.0%)
Pathological tumor-size
T1
43
20 (46.5%)
23 (53.5%)
5.049
0.168
T2
87
36 (41.4%)
51 (58.6%)
T3
29
10 (34.5%)
19 (65.5%)
T4
14
2 (14.3%)
12 (85.7%)
Pleural invasion
No
161
65 (40.4%)
96 (59.6%)
0.015
0.903
Yes
18
7 (38.9%)
11 (61.1%)
Lymph node metastasis
Negative
75
37 (49.3%)
38 (50.7%)
5.865
0.015
Positive
85
26 (30.6%)
59 (69.4%)
Clinical stage
I
55
32 (58.2%)
23 (41.8%)
12.973
0.005
II
40
10 (25.0%)
30 (75.0%)
III
62
20 (32.3%)
42 (67.7%)
IV
3
1 (33.3%)
2 (66.7%)
Note: the tumor differentiation information of 2 cases were unavailable, the pT information of 6 cases were unavailable, the lymph node metastasis information of 19 cases were unavailable, the clinical stage information of 19 cases were unavailable.
Univariate and multivariate analysis of OS according to clinicopathological variables
Univariate analysis
Multivariate analysis
HR (95% CL)
P-value
HR (95% CL)
P-value
Gender (Male vs. female)
0.685 (0.474–0.991)
0.045
0.606 (0.399–0.922)
0.019
Age (years, 60 vs. 60)
1.110 (0.768–1.603)
0.579
Tumor differentiation (Good vs. Moderate vs. Poor)
We next evaluated the association of P2Y receptor expression with clinicopathological variables in LUAD samples with informative TMA data. The results demonstrated that higher P2Y receptor expression in the LUAD TMAs was positively correlated with poor differentiation, more lymph node metastasis, and later clinical stage of the tumor, but showed no significant association with patients’ sex, age, tumor size, and pleural invasion (Table 1).
To discuss how early P2RY6 expression could be detected as a candidate marker for LUAD, we compared the expression of P2Y receptor in 31 cases of early-stage tumors (good–moderate differentiation, T1 tumor size, negative lymph node metastasis, and no pleural invasion) with that in their corresponding paracancerous tissues. In tumors, 17/31 cases (54.8%) showed low P2Y receptor expression and 14/31 (45.2%) cases showed high P2Y receptor expression, while in the corresponding paracancerous tissues, 25/31 cases (80.6%) showed low P2Y receptor expression and 6/31 (19.4%) cases showed high P2Yreceptor expression, and P2Y receptor expression in early-stage LUAD was significantly higher than that in paracancerous tissues ( 4.824, 0.030).
Higher P2RY6 expression correlated with adverse outcomes of LUAD patients
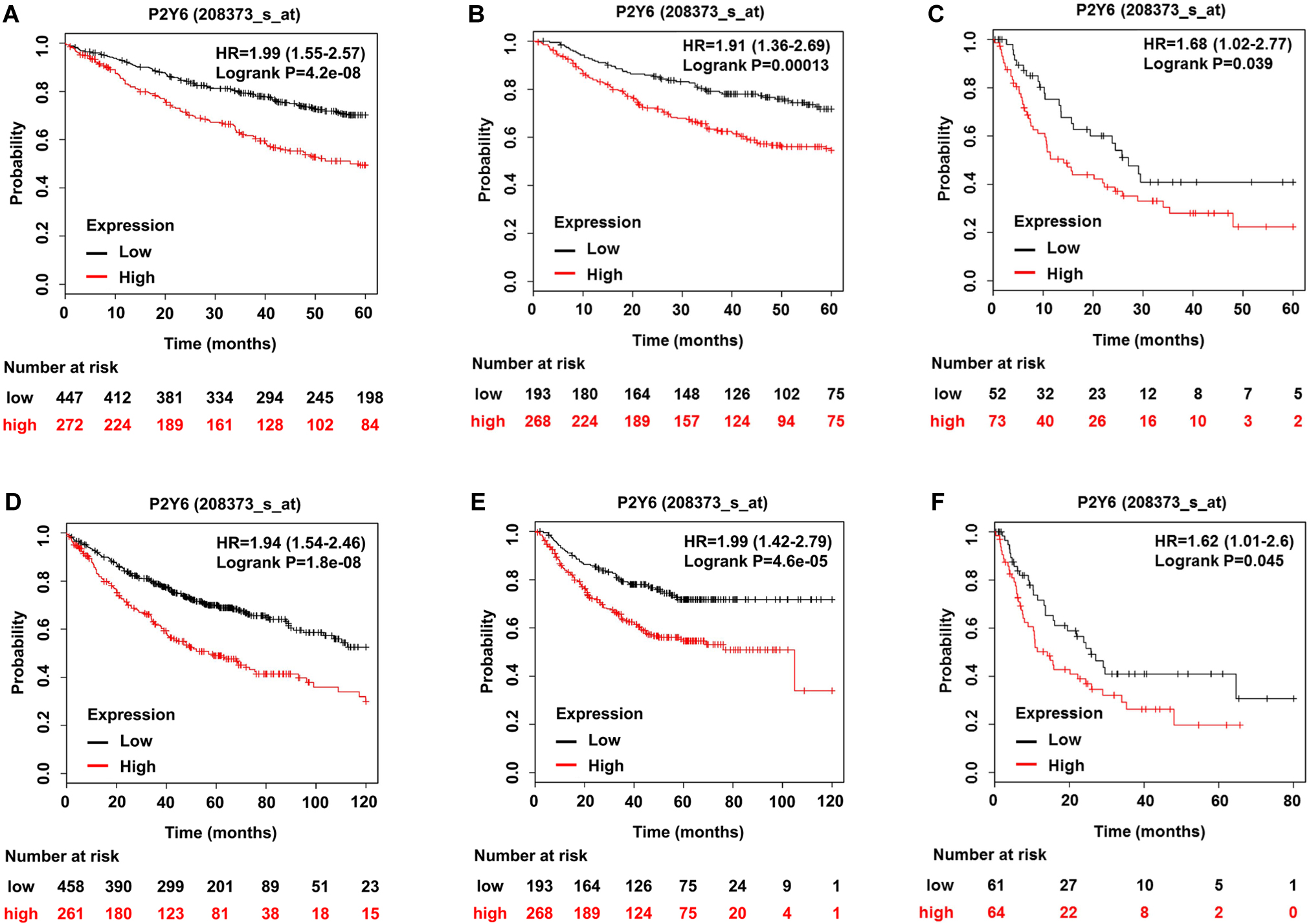
The association of P2RY6 mRNA expression with OS, survival before the first progression (FP), and post-progression survival (PPS) of LUAD patients was preliminarily tested with Kaplan-Meier Plotter (http://kmplot.com), which included 719 LUAD samples based on GEO, EGA, and TCGA databases. The results indicated that LUAD patients with higher P2RY6 mRNA expression had significantly shorter OS, FP, and PPS than those with lower P2RY6 mRNA expression, regardless of whether the follow-up period was 5 or 10 years (Fig. 5).
Bioinformatics analysis of correlation between P2RY6 mRNA expression and survivals of LUAD patients. (A) Association between P2RY6 mRNA expression and 5 years OS of the patients. (B) Association between P2RY6 mRNA expression and 5 years FP of the patients. (C) Association between P2RY6 mRNA expression and 5 years PPS of the patients. (D) Association between P2RY6 mRNA expression and 10 years OS of the patients. (E) Association between P2RY6 mRNA expression and 10 years FP of the patients. (F) Association between P2RY6 mRNA expression and 10 years PPS of the patients.
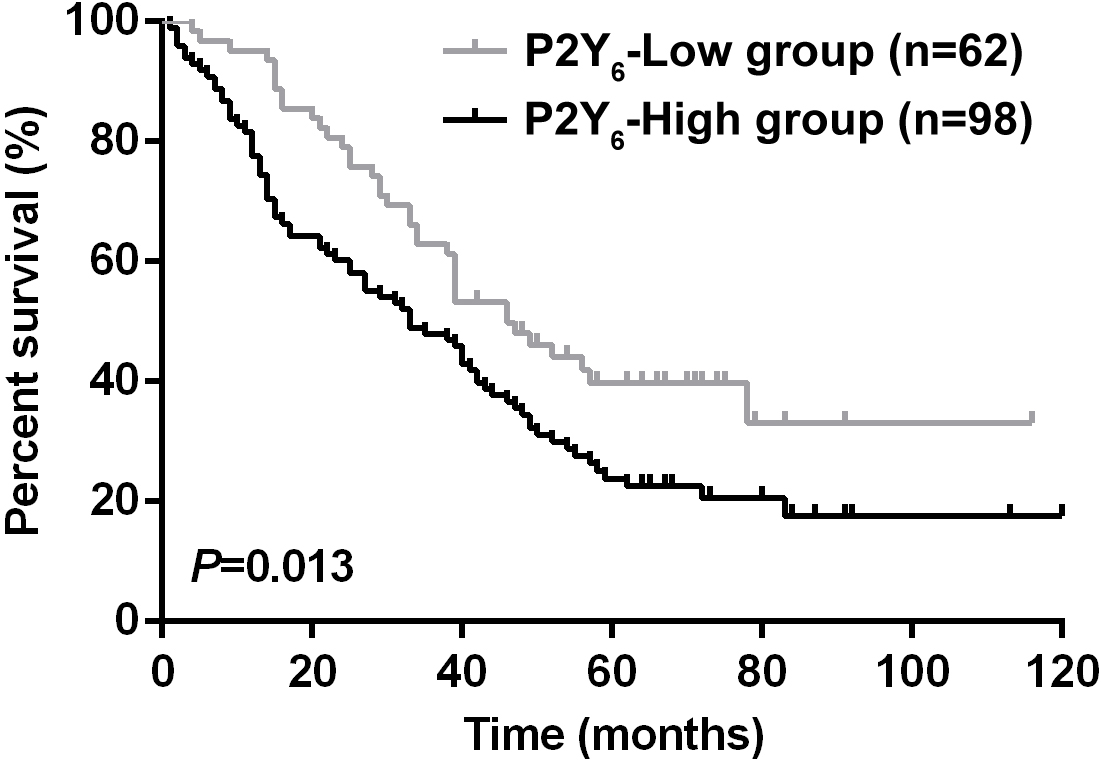
Verifying Correlation between P2Y receptor expression and OS of LUAD patients in TMA cohort.
To verify this in silico result, the correlation between P2Y receptor and OS was further tested in our LUAD TMA cohort. Kaplan-Meier analysis showed that patients in the P2Y-High group had significantly shorter OS than those in the P2Y-Low group (Fig. 6). Multivariate Cox regression analysis after adjusting for sex, tumor grade, pathological tumor size, pleural invasion, and LN metastasis demonstrated that higher P2Y receptor expression was an independent adverse OS risk factor for the patients with LUAD (Table 2).
Discussion
In this study, we investigated the expression and clinical significance of P2RY6 in LUAD. Results from GEPIA, fresh LUAD tissues, and LUAD TMAs all supported the hypothesis that both P2RY6 mRNA and protein expression were elevated in LUAD. The changes in mRNA and protein were highly consistent, suggesting a transcriptional dysregulation mechanism of P2RY6 in LUAD. Increased gene expression is closely related to amplification. The P2RY6 gene is located on chromosome locus 11q13.4, and the 11q13region was identified as one of the most amplified regions in human cancers [28]. Furthermore, the transcriptional activity of P2RY6 was closely related to p53 mutations in LUAD [29, 30, 31], and a recent study reported that the transcriptional activity of P2RY6 was significantly increased when the expression of p53 and p53 in A549 cells reached a ratio of 1:3 or 1:1 [32]. Therefore, gene amplification or p53 mutations might partially account for the aberrant expression of P2RY6 in LUAD observed in our study.
IHC has morphological advantages in assessing protein expressions in situ [33]. In this study, the protein expression of P2Y receptor in 186 cases of LUAD tissues in TMAs was examined by IHC and correlated to the clinicopathological variables. Interestingly, besides being mainly located in the cytoplasm of tumor cells, moderate positive staining of P2Y receptor could also be found in a few lymphocytes in some samples. A panel of studies have reported that P2Y receptor is widely expressed in immune cells including T lymphocytes [34, 35], dendritic cells [36], and macrophages [37], and plays important roles in animal models of autoimmune and allergic diseases. However, there are few reports on the role of P2Y receptor-positive lymphocytes in the tumor microenvironment. A recent article reported that activation of P2Y receptor reduced the tumor-killing activity of NK cells [38], suggesting that P2Y receptor -mediated signaling might affect not only tumor cells, but also the tumor immune microenvironment. In this study, we attempted to correlated P2Y receptor-positive lymphocytes in tumor stroma with the prognosis of the patients; however, because of the small amount of TMA tissue and the limited number of observable tumor stromal lymphocytes, we failed to obtain valuable results from this analysis.
As for the correlations analysis between P2Y receptor expression and clinicopathological variables, we found that higher P2Y receptor expression was associated with poorer differentiation, more lymph node metastasis, and more advanced clinical stage of the tumors in our LUAD TMA cohort. Further, to determine how early P2RY6 expression could be used as a candidate marker for LUAD, we compared the expression of P2Y6 in 31 cases of early-stage tumors. This demonstrated that P2Y receptor expression in early-stage LUAD was significantly higher than that in paracancerous tissues. This result suggested that the increase in P2RY6 expression occurred very early on the development of LUAD and may have acted as driving force for tumor initiation. However, the sample size (31 cases) for the above comparison was quite small, and a large sample, multi-center prospective study is needed to address the question as to whether the high/low expression of P2Y receptor could represent different LUAD variants.
The expression of the P2 family member P2RX7 has been reported to be associated with the poor outcomes of patients with lung cancer [39]. However, the prognostic value of other P2 family members, including P2RY6, was unknown. In this study, we tested the association of P2RY6 expression and clinical outcomes of LUAD patients using Kaplan-Meier Plotter and subsequently verified the in-silico results with the TMA data. Kaplan-Meier Plotter indicated that higher expression of P2RY6 correlated with shorter OS, FP, and PPS in patients with LUAD. Echoing these bioinformatics results, results from the TMA cohort validated the significant association between P2Y receptor expression and shorter OS of patients with LUAD, and Cox regression analyses also identified P2Y receptor expression as an independent adverse risk factor for patients with LUAD. Unfortunately, because of the lack of recurrence information in the datasheet provided by the TMA supplier, the recurrence-free survival analysis (equal to the “survival before the first progression” in Kaplan-Meier Plotter) and PPS analysis were unavailable in the TMA cohort. Despite this weakness, the present results still supported P2RY6 expression as a potential novel prognostic biomarker for LUAD.
In conclusion, the data of this study suggest that P2RY6 is significantly highly expressed in LUAD patients and is associated with poor differentiation, lymph node metastasis, advanced stage, and short survival. Importantly, both univariate and multivariate survival analysis revealed that P2RY6 expression is an independent predictor of poor prognosis in patients with LUAD. Therefore, P2RY6 expression may be a potential biological biomarker for LUAD progression. In the future, we will further investigate the molecular mechanisms of P2RY6 involved in the malignant progression of LUAD.
Funding
This work was supported by the Natural Science Foundation of Heilongjiang Province of China (Grant No. LH2020H031), the Fundamental Research Funds for the Provincial Universities (Grant No. JFXN201906 and JFXN201910), the Scientific research project of Heilongjiang Health Commission (Grant No. 207-147), and the Postgraduate Tutor Foundation of Harbin Medical University-Daqing (Grant No. DSJJ2015003).
Author contributions
Conception: Xiuli Wang, Baoshan Zhao, Dan Ren, Jingbo Liu, and Lin Wang.
Interpretation or analysis of data: Yu Pan, Lili Liu, Xiaolei Hu, Xiaoxue Wang, Huanhuan Ma, Xueling Jia, and Sihang Song.
Preparation of the manuscript: Xiuli Wang, Baoshan Zhao, and Lin Wang.
Revision for important intellectual content: Yanzhi Zhang, Juanjuan Qiao, Yuhua Fan, Chong Zhao and Dongmei Zhang.
Supervision: Lin Wang.
Footnotes
Acknowledgments
We thank H. Nikki March, PhD, from Liwen Bianji (Edanz) (www.liwenbianji.cn/), for editing the English text of a draft of this manuscript.
Conflict of interest
All the authors declared no interest conflict.
References
1.
JalaV.R. et al., Enhanced expression of G-protein coupled estrogen receptor (GPER/GPR30) in lung cancer.BMC Cancer (2012), 624.
2.
WhithausK. et al., Evaluation of napsin A, cytokeratin 5/6, p63, and thyroid transcription factor 1 in adenocarcinoma versus squamous cell carcinoma of the lung.Archives of Pathology & Laboratory Medicine136(2) (2012), 155–162.
3.
WarthA. et al., Large-scale comparative analyses of immunomarkers for diagnostic subtyping of non-small-cell lung cancer biopsies.Histopathology61(6) (2012), 1017–1025.
4.
BlandinK.S. et al., Progress and prospects of early detection in lung cancer.Open Biology7(9) (2017), 170070.
5.
ShiY.X. et al., Prognostic and predictive values of CDK1 and MAD2L1 in lung adenocarcinoma.Oncotarget7(51) (2016), 85235–85243.
6.
SayeeramD. et al., Identification of potential biomarkers for lung adenocarcinoma.Heliyon6(11) (2020), e05452.
7.
LiuW. et al., Identification of genes associated with cancer progression and prognosis in lung adenocarcinoma: Analyses based on microarray from Oncomine and The Cancer Genome Atlas databases.Molecular Genetics & Genomic Medicine7(2) (2019), e00528.
8.
ZouJ. and WangE., Cancer Biomarker Discovery for Precision Medicine: New Progress.Current Medicinal Chemistry26(42) (2019), 7655–7671.
9.
TopalianS.L. et al., Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy.Nature reviews Cancer16(5) (2016), 275–287.
10.
JacobsonK.A. et al., Update of P2Y receptor pharmacology: IUPHAR Review 27.British Journal of Pharmacology177(11) (2020), 2413–2433.
11.
EtiqueN.Grillier-VuissozI. and FlamentS., Ethanol stimulates the secretion of matrix metalloproteinases 2 and 9 in MCF-7 human breast cancer cells.Oncology Reports15(3) (2006), 603–608.
12.
Campos-ContrerasA.D.R.Diaz-MunozM. and Vazquez-CuevasF.G., Purinergic Signaling in the Hallmarks of Cancer.Cells9(7) (2020).
13.
XuP. et al., P2RY6 Has a Critical Role in Mouse Skin Carcinogenesis by Regulating the YAP and beta-Catenin Signaling Pathways.The Journal of Investigative Dermatology142(9) (2022), 2334–2342e2338.
14.
PlacetM. et al., The G protein-coupled P2Y(6) receptor promotes colorectal cancer tumorigenesis by inhibiting apoptosis.Biochimica et Biophysica acta Molecular Basis of Disease1864(5 Pt A) (2018), 1539–1551.
15.
MaX. et al., Chemotherapy-induced uridine diphosphate release promotes breast cancer metastasis through P2Y6 activation.Oncotarget7(20) (2016), 29036–29050.
16.
Abbas AbidiS.M. et al., Differential influence of antiestrogens on the in vitro release of gelatinases (type IV collagenases) by invasive and non-invasive breast cancer cells.Clinical & Experimental Metastasis15(4) (1997), 432–439.
17.
HollaS. et al., Positioning Heterochromatin at the Nuclear Periphery Suppresses Histone Turnover to Promote Epigenetic Inheritance.Cell180(1) (2020), 150–164.
18.
GirardM. et al., The P2Y6 receptor signals through Galphaq /Ca(2+) /PKCalpha and Galpha13 /ROCK pathways to drive the formation of membrane protrusions and dictate cell migration.Journal of Cellular Physiology235(12) (2020), 9676–9690.
19.
AzimiI. et al., Altered purinergic receptor-Ca(2)(+) signaling associated with hypoxia-induced epithelial-mesenchymal transition in breast cancer cells.Molecular Oncology10(1) (2016), 166–178.
20.
SchaferR. et al., ATP- and UTP-activated P2Y receptors differently regulate proliferation of human lung epithelial tumor cells.American Journal of Physiology Lung Cellular and Molecular Physiology285(2) (2003), L376–385.
21.
RoomiM.W. et al., In vitro and in vivo antitumorigenic activity of a mixture of lysine, proline, ascorbic acid, and green tea extract on human breast cancer lines MDA-MB-231 and MCF-7.Medical Oncology22(2) (2005), 129–138.
22.
CarreauC. et al., Enterodiol and enterolactone, two major diet-derived polyphenol metabolites have different impact on ERalpha transcriptional activation in human breast cancer cells.The Journal of Steroid Biochemistry and Molecular Biology110(1-2) (2008), 176–185.
23.
SeegerH.WallwienerD. and MueckA.O., Effects of estradiol and progestogens on tumor-necrosis factor-alpha-induced changes of biochemical markers for breast cancer growth and metastasis.Gynecological Endocrinology: The Official Journal of the International Society of Gynecological Endocrinology24(10) (2008), 576–579.
24.
SmithC.L. and O’MalleyB.W., Coregulator function: a key to understanding tissue specificity of selective receptor modulators.Endocrine Reviews25(1) (2004), 45–71.
25.
ZhangY. et al., Prognostic significance of proline, glutamic acid, leucine rich protein 1 (PELP1) in triple-negative breast cancer: a retrospective study on 129 cases.BMC Cancer15 (2015), 699.
26.
TangZ. et al., a web server for cancer and normal gene expression profiling and interactive analyses.Nucleic Acids Research45(W1) (2017), W98–W102.
27.
LanczkyA. and GyorffyB., Web-Based Survival Analysis Tool Tailored for Medical Research (KMplot): Development and Implementation.Journal of Medical Internet Research23(7) (2021), e27633.
28.
SchwabM., Amplification of oncogenes in human cancer cells.BioEssays: News and Reviews in Molecular, Cellular and Developmental Biology20(6) (1998), 473–479.
29.
MogiA. and KuwanoH., TP53 mutations in nonsmall cell lung cancer.Journal of Biomedicine & Biotechnology (2011), 583929.
30.
CamplingB.G. and el-DeiryW.S., Clinical implications of p53 mutations in lung cancer.Methods in Molecular Medicine75 (2003), 53–77.
31.
WadowskaK. et al., Genetic Markers in Lung Cancer Diagnosis: A Review.International Journal of Molecular Sciences21(13) (2020), 4569.
32.
MolleC.M. et al., The expression of the P2Y6 receptor is regulated at the transcriptional level by p53.Biochemical and Biophysical Research Communications524(4) (2020), 798–802.
33.
AhmedM. et al., Next-generation protein analysis in the pathology department.Journal of Clinical Pathology73(1) (2020), 1–6.
34.
SomersG.R. et al., Expression of the P2Y6 purinergic receptor in human T cells infiltrating inflammatory bowel disease.Laboratory Investigation: A Journal of Technical Methods and Pathology78(11) (1998), 1375–1383.
35.
GiannattasioG. et al., The purinergic G protein-coupled receptor 6 inhibits effector T cell activation in allergic pulmonary inflammation.Journal of Immunology187(3) (2011), 1486–1495.
36.
LiZ. et al., P2Y(6) Deficiency Enhances Dendritic Cell-Mediated Th1/Th17 Differentiation and Aggravates Experimental Autoimmune Encephalomyelitis.Journal of Immunology205(2) (2020), 387–397.
37.
NagaiJ. et al., P2Y6 signaling in alveolar macrophages prevents leukotriene-dependent type 2 allergic lung inflammation.The Journal of Clinical Investigation129(12) (2019), 5169–5186.
38.
LiZ. et al., Purinergic Receptor P2Y(6) Is a Negative Regulator of NK Cell Maturation and Function.Journal of Immunology207(6) (2021), 1555–1565.
39.
BoldriniL. et al., P2X7 mRNA expression in non-small cell lung cancer: MicroRNA regulation and prognostic value.Oncology Letters9(1) (2015), 449–453.