Patients with small ( 2 cm) invasive lung adenocarcinoma are at high risk of poor prognosis and disease recurrence after complete surgical resection. Therefore, identification of high-risk individuals from these patients emerges as an urgent problem. Elevated MACC1 expression predicts a poor prognosis in multiple types of cancer that are independent of TNM staging. This study investigated the prognostic value of MACC1 expression in patients with small invasive lung adenocarcinoma.
OBJECTIVE:
The current study aimed to evaluate the relationship between MACC1 expression in patients’ tumor tissue and prognosis in small invasive lung adenocarcinoma.
METHODS:
The records of 131 patients with small invasive lung adenocarcinoma who underwent complete surgical resection were reviewed. The MACC1 expression was detected by immunohistochemical staining in all specimens. Meanwhile, western blot and real-time quantitative PCR were used to examine the expression level of MACC1 in human lung adenocarcinoma cell lines. The effect of clinicopathological risk factors on patients’ survival was analyzed using the Kaplan-Meier approach and multivariable Cox models.
RESULTS:
Elevated MACC1 expression was observed in 53 (40.5%) specimens, and in A549, H358, H460 and H322 lung adenocarcinoma cell lines. MACC1 overexpression was associated with differentiation ( 0.005) and blood vessel invasion ( 0.001). Compared with low MACC1 expression, elevated MACC1 expression was associated with significantly shorter overall survival (odds ratio 6.515; 95% confidence interval: 1.382–30.721; 0.018) and disease-free survival (odds ratio 3.270; 95% confidence interval: 1.117–9.569; 0.031). Multivariate analyses demonstrated high MACC1 expression is an independent risk factor of worse overall survival (odds ratio 5.684; 95% confidence interval: 1.145–28.210; 0.034) and disease-free survival (odds ratio 4.667; 95% confidence interval: 1.372–15.877; 0.014).
CONCLUSION:
MACC1 is an independent prognostic marker in patients with small invasive lung adenocarcinoma after complete surgical resection. Differential outcomes are associated with MACC1 expression level.
Lung cancer is the leading cause of cancer death worldwide [1]. As recent improvement in computed tomography (CT) technique, the detection of small ( 2 cm) lung cancer, especially adenocarcinoma, the leading aggressive histopathologic type of lung cancer, has been increasing [2]. However, the 5-year survival rate of patients with early stage is merely about 50%–70% as the malignant features of early metastasis and recurrence [3, 4]. Thus, it is critical to identify these small but aggressive tumors for accurate prediction and adjuvant therapy. Advances in genomic research of lung cancer have changed the classification of lung adenocarcinoma to a categorization based on different gene phenotypes [5]. These facts highlight the need for identification of precise molecular biomarkers, to predict the prognosis in patients with lung adenocarcinoma and develop appropriate therapy.
MACC1 is a prognostic biomarker for colorectal cancer metastasis and patient survival that was recently identified in human colon cancer tissues [6]. MACC1 is reported promotes many types of cancer cell proliferation, migration and invasion in cell culture, metastasis in mice model [6, 7]. Recent studies have shown that MACC1 promotes Warburg effect by enhancing the expressions and activities of a series of glycolytic enzymes, including hexokinase (HK), pyruvate dehydrogenase kinase (PDK) and lactate dehydrogenase (LDH) in gastric cancer cells [8]. Meanwhile, overexpression of MACC1 was also involved in drug resistance and enhanced Warburg effect through activation of PI3K/AKT signaling pathway [9]. Moreover, overexpression of MACC1 is associated with poor prognosis in a wide variety of tumor types [7, 10, 11, 12]. Nevertheless, the prognostic role of MACC1 expression in lung cancer, especially in resected small invasive lung adenocarcinoma has not been sufficiently investigated.
Here, we explored the expression of MACC1 in patients with resected small invasive lung adenocarcinoma and evaluated the prognostic role of MACC1 in these patients. Our results showed that elevated MACC1 expression correlates with poor prognosis and early recurrence in small invasive lung adenocarcinoma patients.
Materials and methods
Patients and follow-up
One hundred and thirty-one patients with small invasive lung adenocarcinoma who underwent radical surgery of the primary tumor and systematic nodal dissection without any adjuvant therapy at the First Affiliated Hospital of Dalian Medical University from January 2009 to December 2011 were enrolled. The inclusion criteria of the study was based on invasive lung adenocarcinomas of the tumor 2 cm in diameter identified by routine histopathologic examination. Histologic classification of each tumor was independently examined by two pulmonary pathologists according to the WHO classification of tumors of the lung (4th Edition) which included T adenocarcinoma in situ (AIS), minimally invasive adenocarcinoma (MIA), acinar (Aci), papillary (Pap), micropapillary (MP), solid (Sol), mucinous (Mu). The tumor stage was classified according to the 8th revision of TNM (tumor, nodes, metastasis) staging of the international system for lung cancer. As our previous research [13], patients were followed every 3 months within the first year and at 6-month intervals thereafter. During the follow-up time, physical examination, chest radiography, analysis of blood chemistry, carcinoembryonic antigen (CEA), squamous cell carcinoma antigen (SCC) and serum cytokeratin-19 fragments (CYFRA21-1) test were performed. If any symptom or sign of recurrence appeared in these examinations, further evaluations to detect the recurrent site were carried out. The terminal follow-up time was January 2014 (median follow-up: 32 months). The study was approved by the Medical Ethical Committees of the First Affiliated Hospital of Dalian Medical University. All patients provided written informed consent and agreed their tissue samples could be used for clinical research but not commercial use.
Immunohistochemical staining (IHC)
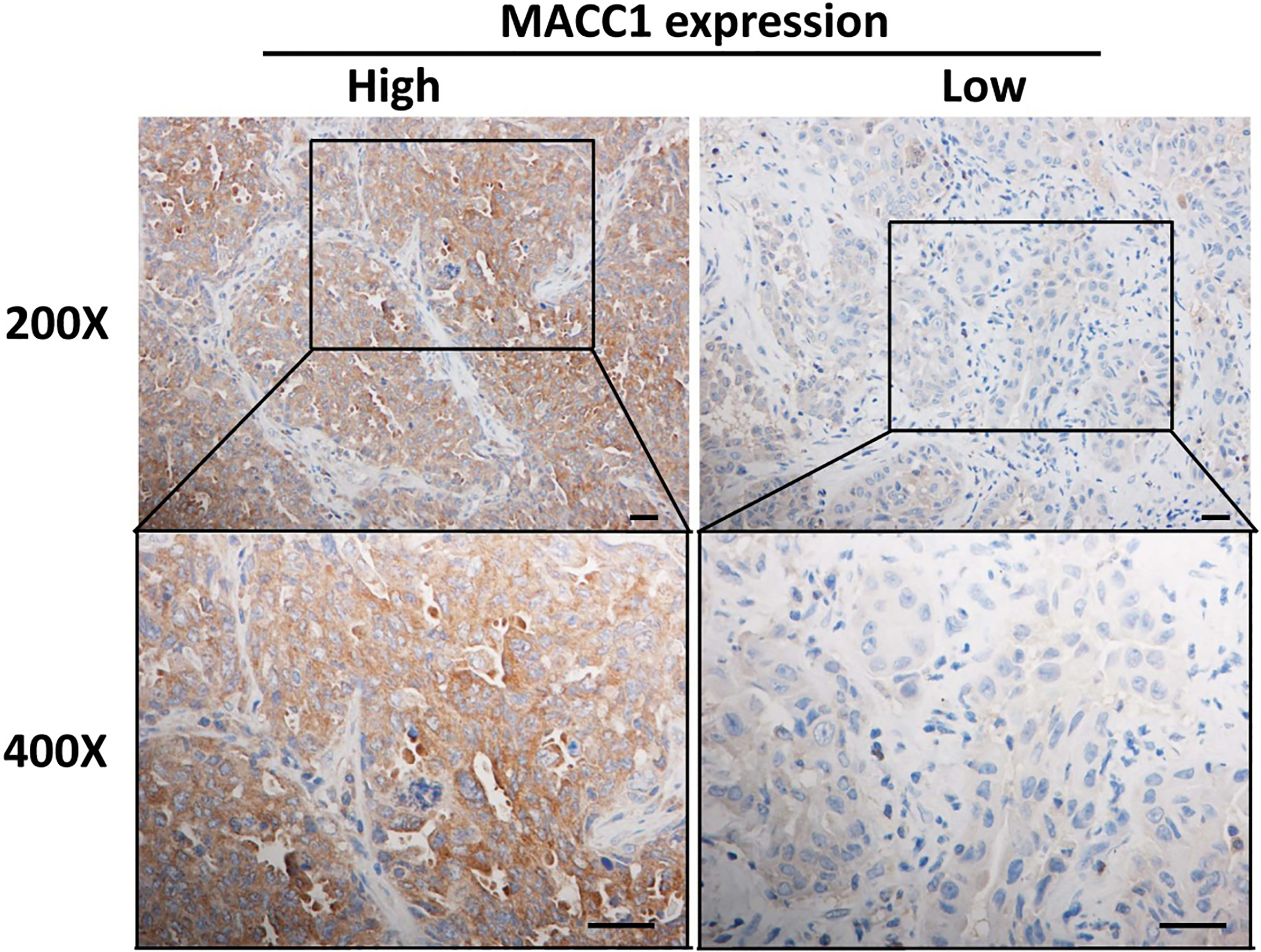
All resected specimens were obtained from primary lesions, fixed with formalin, embedded with paraffins, serial 3 m sections were prepared. The sections were briefly incubated with xylene, rehydrated with graded ethanol solutions, incubated with methyl alcohol containing 3% hydrogen peroxide and immersed in a citrate buffer for antigen retrieval. IHC staining was performed using Streptavidin-Peroxidase IHC assay kit (ZSGB-bio, China) following the manufacturer’s instructions. Antibodies of MACC1 (Abcam, ab12148) was diluted 1:200 in PBS containing 2% goat serum. Immunostaining was evaluated by two pulmonary pathologists using a blind protocol design. For each specimen, the total score of intensity expression (negative staining: 0 point; weak staining: 1point; moderate staining: 2 point; and strong staining: 3 point) multiplying stained cell numbers (positive cells as 25% of the cells: 1 point; 26–50% of the cells: 2 point; 51–75% of the cells: 3 point; 75% of the cells: 4 point) of MACC1 was estimated. When the sample was scored 6 point, we defined it as high expression, otherwise low expression.
Clinicopathologic characteristics in 131 patients with completely resected small ( 2 cm) invasive lung adenocarcinoma
Representative IHC staining in small lung adenocarcinoma tissue. Notes: The typical appearances had shown high and low expression of MACC1 by IHC, respectively. Original magnification 200 and 400 in inset.
Relations between the expression of MACC1 and clinicopathologic characteristics in invasive lung adenocarcinoma
Variable
MACC1 expression
-value
High (%)
Low (%)
Total
53 (40.5)
78
Sex
0.596
Male
29 (42.6)
39
Female
24 (38.1)
39
Age
0.126
69 y
31 (47.0)
35
69 y
22 (33.8)
43
Smoking
0.149
Non-smoker
15 (30.0)
35
Ex-smoker
17 (44.7)
21
Smoker
21 (48.8)
22
WHO classification
0.584
MIA
2
9
Lepidic
10
12
Acinar
19
31
Papillary
13
18
Micropapillary
2
1
Solid
1
2
Mucinous
6
5
Differentiation
0.005
Well
24 (31.6)
52
Moderate
24 (49.0)
25
Poor
5 (83.3)
1
Lymph node metastasis
0.098
Absent
43 (37.7)
71
Present
10 (58.8)
7
Blood vessel invasion
0.001
Absent
44 (36.4)
77
Present
9 (90.0)
1
TNM stage
0.144
I
43 (38.1)
70
II
8 (53.3)
7
III
2 (66.7)
1
CEA
0.375
Abnormal
5 (50.0)
5
Normal
48 (39.7)
73
SCC
0.248
Abnormal
6 (11.3)
47
Normal
5 (6.4)
73
CYFRA21-1
0.894
Abnormal
10 (18.9)
43
Normal
14 (17.9)
64
Notes: Statistical significance was evaluated using the chi-square test. Differences were considered to be statistically significant for -value 0.05 which are shown in bold. Abbreviations: TNM, tumor, node, metastases; MIA, minimally invasive adenocarcinoma; CEA, carcinoembryonic antigen; SCC, squamous cell carcinoma antigen; CYFRA21-1, serum cytokeratin-19 fragments; MACC1, metastasis-associated in colon cancer 1.
Cell lines and reagents
Human lung adenocarcinoma cell lines (A549, NCI-H358, NCI-H460 and NCI-H322) and normal human fetal lung fibroblasts cell line (HFL-1) were purchased from American Type Culture Collection (ATCC, Manassas, VA, USA). Cells were cultured in ATCC-recommended medium supplemented with 10% fetal bovine serum (FBS) and incubated at 37C in humidified 5% CO incubator.
Western blotting
Western blot analysis was performed according to the protocols for the routine measurement of antibodies against MACC1 (Rabbit, 1:2000, Abcam, ab12148), GAPDH (Mouse, 1:5000, Sigma, A5441), respectively. Goat-anti-rabbit IgG conjugated to hor- seradish peroxidase (HRP) (1:5000, Thermo, 31460) and goat-anti-mouse IgG conjugated to HRP (1:5000, Thermo, 31430) which was used as the secondary antibody.
RNA Isolation, reverse-transcription, and real-time quantitative PCR (q-PCR)
Total RNA was extracted by using TRIzol reagent (Invitrogen). Total RNA was used to generate cDNA by using PrimeScript reverse transcriptase reagent kit (Takara, RR014A) according to the manufacturer’s instructions. Real-time quantitative PCR was performed by using the specific SYBR Select Master Mix (Life technologies, 4472908) in a MX3000p cycler (Stratagene). Changes of mRNA levels were determined by the 2 method using Actin for internal crossing normalization. The following PCR primers were used: MACC1 (forward 5’-GGCTGTGATGCTACGAGAT A-3’; reverse 5’-ACACCAGGACAATGCCTACT-3’), ACTB (forward 5’-CATGTACGTTGCTATCCAGGC-3’; reverse 5’-CTCCTTAATGTCACGCACGAT-3’).
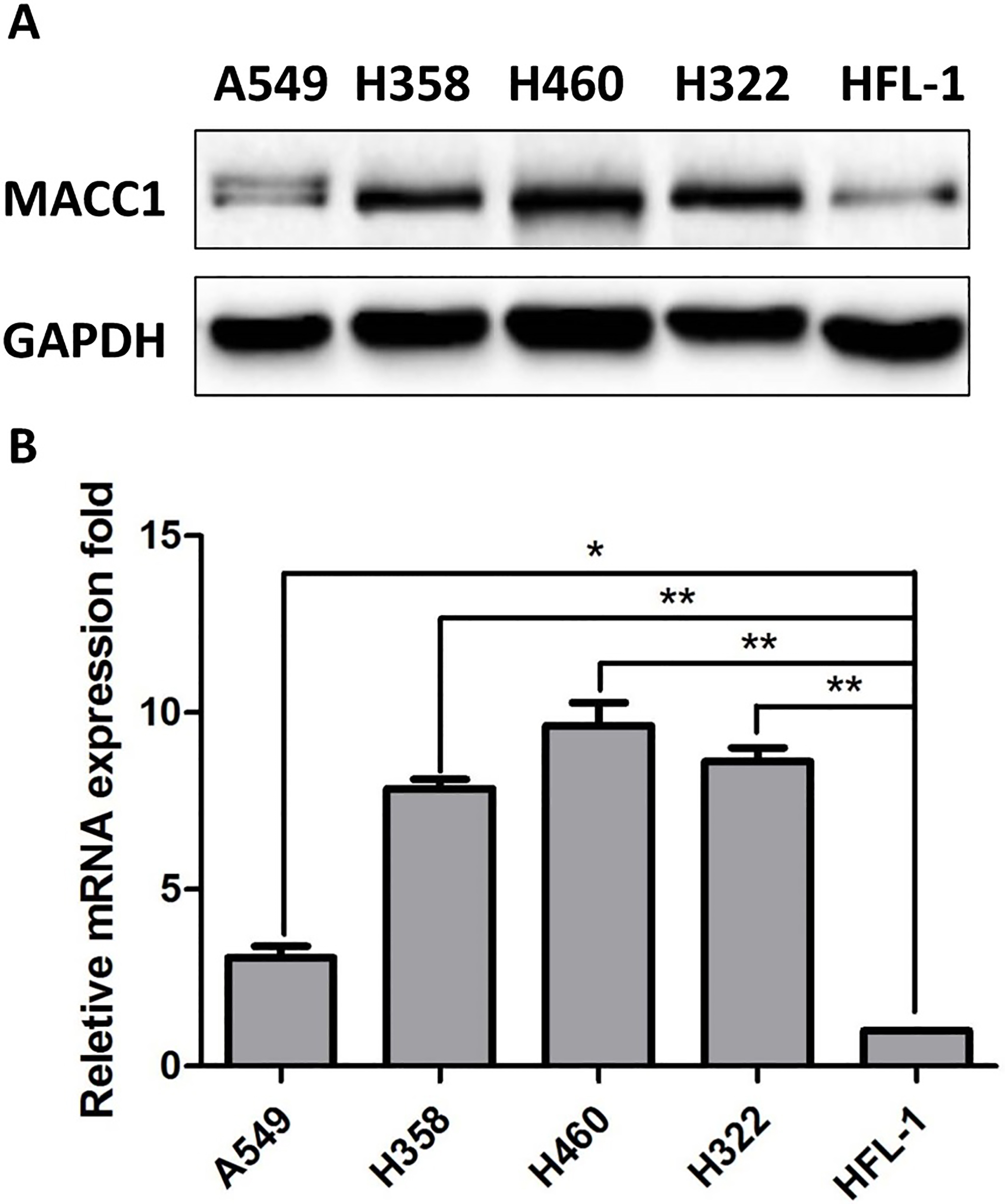
MACC1 is over-expressed in human lung adenocarcinoma cell lines. Notes: (A) Expression of MACC1 protein detected by Western blot analysis in cell lines. (B) Expression of MACC1 mRNA detected by Q-PCR in cell lines ( 0.05, 0.01). Error bars represent mean SD. Abbreviations: GAPDH, glyceraldehyde-3-phosphate dehydrogenase; SD, standard deviation.
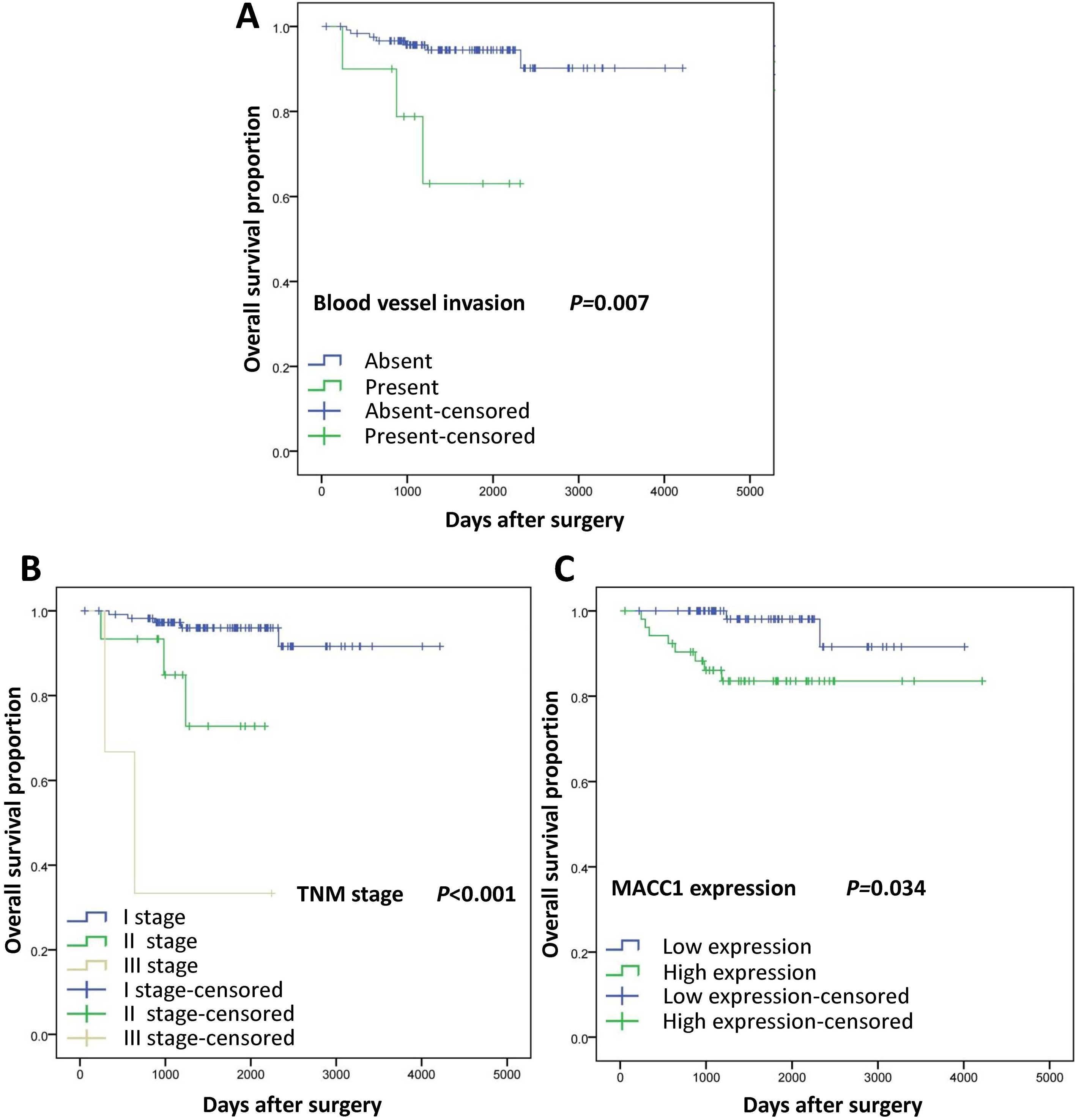
Kaplan-Meier survival curves for OS in 131 patients with small invasive lung adenocarcinoma after complete resection. Notes: (A) and (B) Patients with blood vessel invasion ( 0.007) or advanced TNM stage ( 0.001) had a shorter OS. (C) High expression of MACC1 was associated with worse OS ( 0.034) in lung adenocarcinoma. Abbreviation: TNM, tumor, node, metastases.
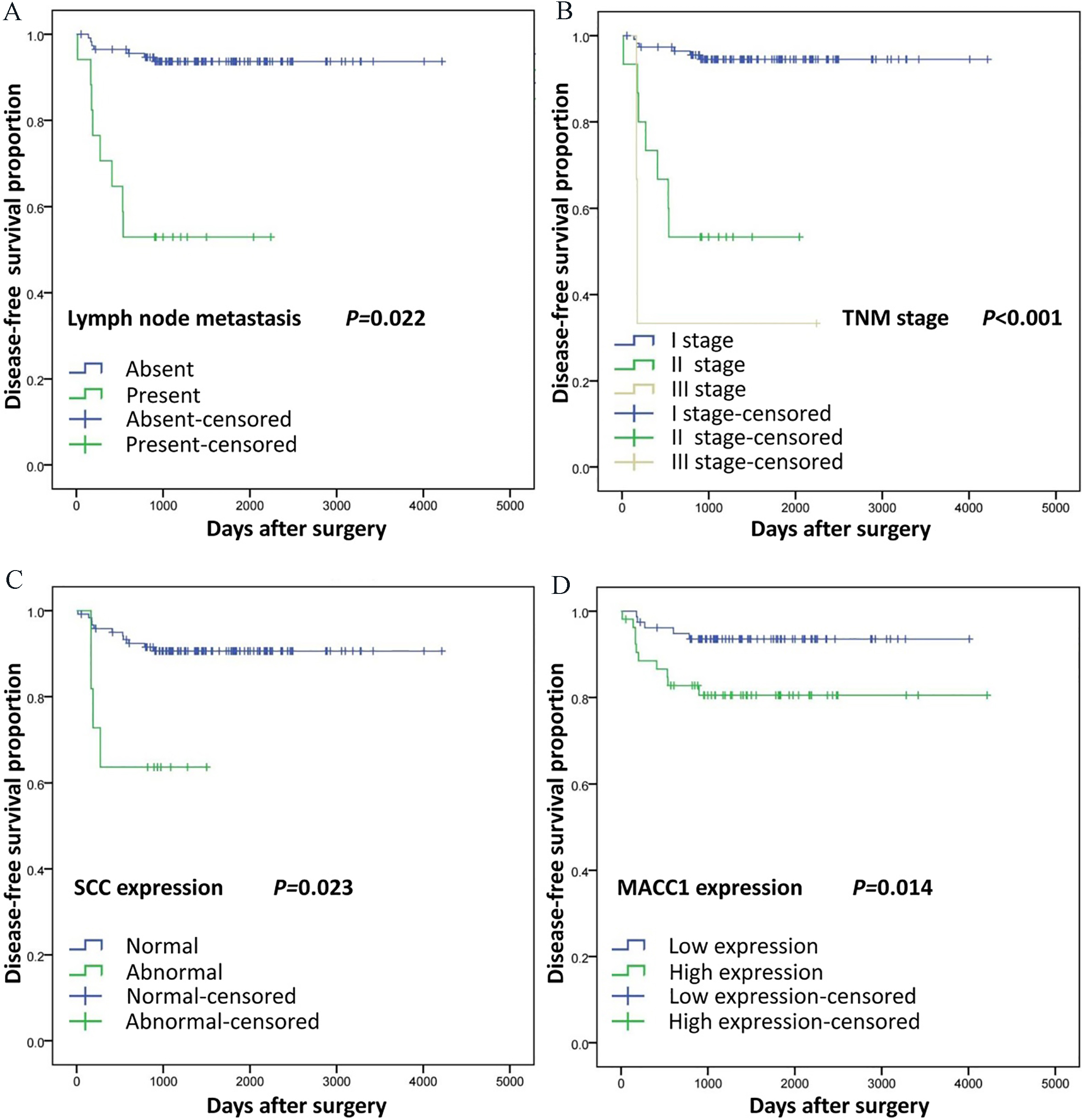
Kaplan-Meier survival curves for DFS in 131 patients with small invasive lung adenocarcinoma after complete resection. Notes: (A) and (B) Patients with lymph node metastasis ( 0.022) or advanced TNM stage ( 0.001) had a shorter DFS. (C) High level of serum SCC ( 0.023)or high expression of MACC1 ( 0.014) was associated with worse DFS. Abbreviation: TNM, tumor, node, metastases; SCC, squamous cell carcinoma antigen.
Univariate analysis overall survival (OS) and disease-free survival (DFS) on different clinicopathological factors by Cox regression
Variable
5-OS
5-DFS
OR
95% CI
-value
OR
95% CI
-value
Sex
Male
1.000
1.000
Female
0.742
0.209–2.633
0.643
0.690
0.246–1.939
0.482
Age
69 y
1.000
1.000
69 y
1.096
0.314–3.789
0.885
0.487
0.166–1.425
0.189
Smoking
Non-smoker
0.315
0.061–1.624
0.167
0.549
0.155–1.944
0.352
Ex-smoker
0.679
0.162–2.844
0.596
0.956
0.292–3.132
0.940
Smoker
1.000
1.000
WHO classification
MIA
0.001
–
0.974
0.001
–
0.984
Lepidic
0.001
–
0.963
0.142
0.015–1.368
0.091
Acinar
0.278
0.078–0.986
0.047
0.204
0.041–1.012
0.052
Papillary
0.147
0.027–0.803
0.027
0.111
0.110–1.066
0.057
Micropapillary
0.864
0.096–7.742
0.896
1.714
0.175–16.766
0.643
Solid
3.068
0.558–16.860
0.197
1.215
0.125–11.822
0.867
Mucinous
1.000
1.000
Differentiation
Well
0.092
0.015–0.564
0.010
0.066
0.009–0.466
0.006
Moderate
0.230
0.043–1.212
0.083
0.593
0.131–2.681
0.498
Poor
1.000
1.000
Lymph node metastasis
Absent
1.000
1.000
Present
9.996
2.673–37.382
0.001
9.821
3.545–27.202
0.001
Blood vessel invasion
Absent
1.000
1.000
Present
7.098
1.769–28.488
0.006
3.506
0.988–12.439
0.052
TNM stage
I
0.033
0.006–0.185
0.001
0.041
0.008–0.208
0.001
II
0.209
0.035–1.268
0.089
0.456
0.094–2.227
0.332
III
1.000
1.000
CEA
Abnormal
1.406
0.178–11.104
0.747
0.899
0.118–6.836
0.918
Normal
1.000
1.000
SCC
Abnormal
3.739
0.768–18.195
0.102
4.966–
1.576–15.647
0.006
Normal
1.000
1.000
CYFRA21-1
Abnormal
2.044
0.525–7.957
0.303
1.101
0.311–3.901
0.882
Normal
1.000
1.000
MACC1
High expression
6.515
1.382–30.721
0.018
3.270
1.117–9.569
0.031
Low expression
1.000
1.000
Notes: Statistical significance was evaluated using the Cox regression test. Differences were considered to be statistically significant for -value 0.05 which are shown in bold. Abbreviations: OR, odds ratio; MIA, minimally invasive adenocarcinoma; TNM, tumor, node, metastases; CEA, carcinoembryonic antigen; SCC, squamous cell carcinoma antigen; CYFRA21-1, serum cytokeratin-19 fragments; MACC1, metastasis-associated in colon cancer 1.
Multivariate analysis of overall survival using Cox regression
Variable
Overall survival
OR
95% CI
-value
Differentiation
Well
0.913
0.068–12.182
0.945
Moderate
0.827
0.093–7.377
0.865
Poor
1.000
Lymph node metastasis
Absent
0.550
0.244–1.320
0.644
Present
1.000
Blood vessel invasion
Absent
1.000
Present
9.116
1.822–45.618
0.007
TNM stage
I
0.015
0.002–0.115
0.001
II
0.112
0.016–0.767
0.026
III
1.000
MACC1
High expression
5.684
1.145–28.210
0.034
Low expression
1.000
Notes: Statistical significance was evaluated using the Cox regression test. Differences were considered to be statistically significant for -value 0.05 which are shown in bold. Abbreviations: OR, odds ratio; TNM, tumor, node, metastases; MACC1, metastasis-associated in colon cancer 1.
Multivariate analysis of disease-free survival using Cox regression
Variable
Disease-free survival
OR
95% CI
-value
Differentiation
Well
0.447
0.046–4.356
0.488
Moderate
1.522
0.275–8.429
0.631
Poor
1.000
Lymph node metastasis
Absent
0.054
0.004–0.656
0.022
Present
1.000
TNM stage
I
0.003
0.001–0.072
0.001
II
0.264
0.048–1.453
0.126
III
1.000
SCC
Abnormal
4.598
1.233–17.147
0.023
Normal
1.000
MACC1
High expression
4.667
1.372–15.877
0.014
Low expression
1.000
Notes: Statistical significance was evaluated using the Cox regression test. Differences were considered to be statistically significant for -value 0.05 which are shown in bold. Abbreviations: OR, odds ratio; TNM, tumor, node, metastases; SCC, squamous cell carcinoma antigen; MACC1, metastasis-associated in colon cancer 1.
Statistical analysis
Student’s t-test or analysis of variance (ANOVA) was used to compare the values of the test and control samples in vitro and in vivo. Survival curves were calculated using the Kaplan Meier method. The log-rank test was used to analyze overall survival (OS) time between different clinicopathological factors in lung adenocarcinoma. Univariate and multivariate analysis were performed using the Cox regression model. Data was analyzed by the SPSS 20 software (Inc, Chicago, IL). Values of 0.05 were considered statistically significant difference.
Results
Clinicopathologic characteristics of patients
The overall clinicopathologic characteristics of the 131 patients were summarized in Table 1. Among 131 patients, 68 (51.9%) were male and 63 (48.1%) were female. Tumors were classified as MIA, lepidic, acinar, papillary, micropapillary, solid and mucinous in 11 (8.4%), 22 (16.8%), 50 (38.2%), 31 (23.7%), 3 (2.3%), 3 (2.3%) and 11 (8.4%) of the cases, respectively. The number of patients with well, moderate and poor differentiation was 76 (58.0%), 49 (37.4%) and 6 (4.6%), respectively. Seventeen (13.0%) and 10 (7.6%) patients appeared lymph node metastasis and blood vessel invasion, respectively. One hundred and thirteen (86.3%) patients with TNM stage I, 15 (11.5%) patients with TNM stage II and 3 (2.3%) patients with TNM stage III. The preoperative serum carcinoembryonic antigen (CEA), squamous cell carcinoma antigen (SCC) and cytokeratin-19 fragments (CYFRA21) level were elevated in 10 (7.6%), 53 (40.5%) and 53 (40.5%) patients, respectively.
Association between clinicopathologic characteristics and MACC1 expression
Among 131 patients, high MACC1 expression was observed in 53 (40.5%), and typical appearances of high and low MACC1 expression were shown in Fig. 1. Correlation between clinicopathologic characteristics and MACC1 expression were summarized in Table 2. MACC1 expression was positively correlated with differentiation ( 0.005) and blood vessel invasion ( 0.001) but not with sex, age, smoking status, lymph node metastasis, TNM stage, preoperative serum CEA, SCC and CYFRA21 level.
MACC1 is over-expressed in human lung adenocarcinoma cell lines
Next, we investigated the MACC1 expression in 4 human lung adenocarcinoma cell lines (A549, H358, H460, H322) and 1 normal human fetal lung fibroblast (HFL-1) by Western blotting and real-time quantitative PCR assays. As shown in Fig. 2, higher expression of MACC1 was observed in lung adenocarcinoma cell lines compared with normal human fetal lung fibroblast.
Impact of risk factor on survival and recurrence
As shown in Table 3 and Fig. 3, poor differentia- tion ( 0.010), lymph node metastasis ( 0.001), blood vessel invasion ( 0.006), advanced TNM stage ( 0.001) and high MACC1 expression ( 0.018) had a shorter overall survival (OS) by univariate analysis. In multivariate analysis, blood vessel invasion (odds ratio [OR] 9.116; 95% confidence interval [CI], 1.822–45.618; 0.007), advanced TNM stage (OR 0.015; 95% CI, 0.002–0.115; 0.001) and high MACC1 expression (OR 5.684; 95% CI, 1.145–28.210; 0.034) were shown as independent risk factors of OS (Table 4). Meanwhile, the results showed that poor differentiation ( 0.006), lymph node metastasis ( 0.001), advanced TNM stage ( 0.001), high level of serum SCC ( 0.006) and high MACC1 expression ( 0.031) were related to worse disease-free survival (DFS) by univariate analysis (Table 3 and Fig. 4). Furthermore, lymph node metastasis (OR 0.054; 95% CI, 0.004–0.656; 0.022), advanced TNM stage (OR 0.003; 95% CI, 0.001–0.072; 0.001), high level of serum SCC (OR 4.598; 95% CI, 1.233–17.147; 0.023) and high MACC1 expression (OR 4.667; 95% CI, 1.372–15.877; 0.014) were shown as independent risk factors of DFS, according to Cox proportional hazards model (Table 5).
Discussion
The prevalence of low-dose spiral computed tomography screening has significantly increased the detection of small ( 2 cm) lung adenocarcinoma [14]. The main treatment for small ( 2 cm) lung adenocarcinoma is complete surgical resection with mediastinal lymph node dissection or systematic sampling. Unfortunately, in clinical practice, part of patients with small ( 2 cm) lung adenocarcinoma showed early metastasis and relapse after complete surgical resection [15, 16]. Therefore, identification of patients with poor prognosis through effective molecular biomarker is of significant importance, because such patients require more intensive follow-up and adjuvant treatment.
Our compelling evidence revealed that MACC1 is an independent prognostic marker in patients with small invasive lung adenocarcinoma after complete surgical resection. Specifically, we report the following findings: (1) the incidence of MACC1 positive staining was significantly higher in recurrent cases than in non-recurrent ones; (2) the protein and mRNA expression levels of MACC1 were much higher in lung adenocarcinoma cell lines than in HFL-1 cell line; (3) clinically, univariate and multivariate Cox regression analysis showed that MACC1 was an independent risk factor prognostic indicator for patients with small ( 2 cm) lung adenocarcinoma. These results indicate that the expression of MACC1 is a useful prognostic marker for patients with small lung adenocarcinoma.
MACC1 was previously reported to regulate invasion and metastasis through regulating HGF/c-Met pathway in several cancer types [6, 17, 18]. We previously found that MACC1 was a useful marker for predicting postoperative recurrence in patients with lung adenocarcinoma following surgery [19]. However, the prognostic role of MACC1 expression in resected small invasive lung adenocarcinoma remains unclear. In the present study, we found that 53 (40.5%) patients with small invasive lung adenocarcinoma had high MACC1 expression primarily distributed in cytoplasm. Nevertheless, this study focused on invasive adenocarcinoma and especially those with the diameter 2 cm in the enrolled patients, our previous study and other researchers reported the higher proportion of MACC1 expression appeared in lung cancer [19, 20, 21]. Furthermore, we confirmed the high expression of MACC1 in lung adenocarcinoma through detecting the protein and mRNA expression in human lung adenocarcinoma cell lines (A549, H358, H460 and H322). The Western blotting and real-time quantitative PCR results showed that lung adenocarcinoma cells exhibited higher expression of MACC1 than HFL-1 cells.
According to our results, high expression of MACC1 was positively correlated with differentiation ( 0.005) and blood vessel invasion ( 0.001) but not with other clinical pathologic factors. Consistent with our data, recent reports have shown that the expression of MACC1 is positively correlated with differentiation grade [20, 21]. Meanwhile, blood vessel invasion is a well-established adverse prognostic factor for non-small cell lung carcinoma (NSCLC) [22, 23]. Recently, blood vessel invasion has been demonstrated as a independent predictor of worse OS and recurrence in small-sized NSCLC [24]. In our study, poor differentiation ( 0.010), lymph node metastasis ( 0.001), blood vessel invasion ( 0.006), advanced TNM stage ( 0.001) and high MACC1 expression ( 0.018) affected the OS of the 131 patients with small lung adenocarcinoma by univariate analysis; poor differentiation ( 0.006), lymph node metastasis ( 0.001), advanced TNM stage ( 0.001), high level of serum SCC ( 0.006) and high MACC1 expression ( 0.031) were related to the DFS by univariate analysis. In the further multivariate analysis, blood vessel invasion (OR 9.116; 95% CI, 1.822–45.618; 0.007), advanced TNM stage (OR 0.015; 95% CI, 0.002–0.115; 0.001) and high MACC1 expression (OR 5.684; 95% CI, 1.145–28.210; 0.034) were shown as independent risk factors of OS. Furthermore, lymph node metastasis (OR 0.054; 95% CI, 0.004–0.656; 0.022), advanced TNM stage (OR 0.003; 95% CI, 0.001–0.072; 0.001), high level of serum SCC (OR 4.598; 95% CI, 1.233–17.147; 0.023) and high MACC1 expression (OR 4.667; 95% CI, 1.372–15.877; 0.014) were shown as independent risk factors of DFS.
The limitations of this study should be taken into consideration. We did not record the information of treatment after recurrence, which may result in bias to OS. In addition, this retrospective analysis is a single institutional analysis, and focus on small-sized tumor samples. Thus, the inherent bias is inevitable.
Conclusions
These evidences revealed that MACC1 is an independent indicator in patients with small invasive lung adenocarcinoma after complete surgical resection. Detection of the MACC1 expression may be useful to for identifying patients with small lung adenocarcinoma who require more intensive follow-up and adjuvant treatment following a complete resection.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (81173453, 81774078). Natural Science Foundation of Liaoning Province, China (201602227).
Conflict of interest
The authors declare that they have no competing interests.
References
1.
SiegelR.L.MillerK.D. and JemalA., Cancer statistics, 2016, CA: a cancer journal for clinicians66(1) (2016), 7–30.
2.
The National Lung Screening Trial ResearchChurchT.R.BlackW.C.AberleD.R.BergC.D.ClinganK.L.DuanF.FagerstromR.M.GareenI.F.GieradaD.S.JonesG.C.MahonI.MarcusP.M.SicksJ.D.JainA. and BaumS., Results of initial low-dose computed tomographic screening for lung cancer, The New England journal of medicine368(21) (2013), 1980–1991.
3.
GoldstrawP.ChanskyK.CrowleyJ.Rami-PortaR.AsamuraH.EberhardtW.E.NicholsonA.G.GroomeP.MitchellA. and BolejackV., S. International Association for the Study of Lung Cancer, A.B. Prognostic Factors Committee, I. Participating, S. International Association for the Study of Lung Cancer, B. Prognostic Factors Committee Advisory, I. Participating, The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer, Journal of thoracic oncology: official publication of the International Association for the Study of Lung Cancer11(1) (2016), 39–51.
4.
SawabataN., Prognosis of lung cancer patients in Japan according to data from the Japanese Joint Committee of Lung Cancer Registry, Respiratory investigation52(6) (2014), 317–321.
5.
Cancer Genome Atlas Research Network, Comprehensive molecular profiling of lung adenocarcinoma, Nature511(7511) (2014), 543–550.
6.
SteinU.WaltherW.ArltF.SchwabeH.SmithJ.FichtnerI.BirchmeierW. and SchlagP.M., MACC1, a newly identified key regulator of HGF-MET signaling, predicts colon cancer metastasis, Nature medicine15(1) (2009), 59–67.
7.
WangL.WuY.LinL.LiuP.HuangH.LiaoW.ZhengD.ZuoQ.SunL.HuangN.ShiM.LiaoY. and LiaoW., Metastasis-associated in colon cancer-1 upregulation predicts a poor prognosis of gastric cancer, and promotes tumor cell proliferation and invasion, International journal of cancer133(6) (2013), 1419–1430.
8.
LinL.HuangH.LiaoW.MaH.LiuJ.WangL.HuangN.LiaoY. and LiaoW., MACC1 supports human gastric cancer growth under metabolic stress by enhancing the Warburg effect, Oncogene34(21) (2015), 2700–2710.
9.
LiuJ.PanC.GuoL.WuM.GuoJ.PengS.WuQ. and ZuoQ., A new mechanism of trastuzumab resistance in gastric cancer: MACC1 promotes the Warburg effect via activation of the PI3K/AKT signaling pathway, Journal of hematology & oncology9(1) (2016), 76.
10.
LedererA.HerrmannP.SeehoferD.DietelM.PratschkeJ.SchlagP. and SteinU., Metastasis-associated in colon cancer 1 is an independent prognostic biomarker for survival in Klatskin tumor patients, Hepatology62(3) (2015), 841–850.
11.
HagemannC.FuchsS.MonoranuC.M.HerrmannP.SmithJ.HohmannT.GrabiecU.KesslerA.F.DehghaniF.LohrM.ErnestusR.I.VinceG.H. and SteinU., Impact of MACC1 on human malignant glioma progression and patients’ unfavorable prognosis, Neuro-oncology15(12) (2013), 1696–1709.
12.
MuendleinA.HubalekM.Geller-RhombergS.GasserK.WinderT.DrexelH.DeckerT.Mueller-HolznerE.ChamsonM.MarthC. and LangA.H., Significant survival impact of MACC1 polymorphisms in HER2 positive breast cancer patients, European journal of cancer50(12) (2014), 2134–2141.
13.
ZhaoS.GuoT.LiJ.UramotoH.GuanH.DengW. and GuC., Expression and prognostic value of GalNAc-T3 in patients with completely resected small (</= 2 cm) peripheral lung adenocarcinoma after IASLC/ATS/ERS classification, Onco Targets and therapy8 (2015), 3143–3152.
14.
LeeH.Y.HanJ.LeeK.S.KooJ.H.JeongS.Y.KimB.T.ChoY.S.ShimY.M.KimJ.KimK. and ChoiY.S., Lung adenocarcinoma as a solitary pulmonary nodule: prognostic determinants of CT, PET, and histopathologic findings, Lung cancer66(3) (2009), 379–385.
15.
ZhouQ.SuzukiK.AnamiY.OhS. and TakamochiK., Clinicopathologic features in resected subcentimeter lung cancer-status of lymph node metastases, Interactive cardiovascular and thoracic surgery10(1) (2010), 53–57.
16.
LiuS.WangR.ZhangY.LiY.ChengC.PanY.XiangJ.ZhangY.ChenH. and SunY., Precise Diagnosis of Intraoperative Frozen Section Is an Effective Method to Guide Resection Strategy for Peripheral Small-Sized Lung Adenocarcinoma, Journal of clinical oncology: official journal of the American Society of Clinical Oncology34(4) (2016), 307–313.
17.
GalimiF.TortiD.SassiF.IsellaC.CoraD.GastaldiS.RiberoD.MuratoreA.MassuccoP.SiatisD.ParaluppiG.GonellaF.MaioneF.PisacaneA.DavidE.TorchioB.RisioM.SalizzoniM.CapussottiL.PereraT.MedicoE.Di RenzoM.F.ComoglioP.M.TrusolinoL. and BertottiA., Genetic and expression analysis of MET, MACC1, and HGF in metastatic colorectal cancer: response to met inhibition in patient xenografts and pathologic correlations, Clin Cancer Res17(10) (2011), 3146–3156.
18.
ArltF. and SteinU., Colon cancer metastasis: MACC1 and Met as metastatic pacemakers, Int J Biochem Cell Biol41(12) (2009), 2356–2359.
19.
ChundongG.UramotoH.OnitsukaT.ShimokawaH.IwanamiT.NakagawaM.OyamaT. and TanakaF., Molecular diagnosis of MACC1 status in lung adenocarcinoma by immunohistochemical analysis, Anticancer research31(4) (2011), 1141–1145.
20.
WangZ.LiZ.WuC.WangY.XiaY.ChenL.ZhuQ. and ChenY., MACC1 overexpression predicts a poor prognosis for non-small cell lung cancer, Medical oncology31(1) (2014), 790.
21.
ZhouL.YuL.ZhuB.WuS.SongW.GongX. and WangD., Metastasis-associated in colon cancer-1 and aldehyde dehydrogenase 1 are metastatic and prognostic biomarker for non-small cell lung cancer, BMC cancer16(1) (2016), 876.
22.
DziedzicD.A.RudzinskiP.LangfortR. and OrlowskiT., Polish Lung Cancer Study Group, Risk Factors for Local and Distant Recurrence After Surgical Treatment in Patients With Non-Small-Cell Lung Cancer, Clinical lung cancer17(5) (2016), e157–e167.
23.
OkadaS.MizuguchiS.IzumiN.KomatsuH.TodaM.HaraK.OkunoT.ShibataT.WanibuchiH. and NishiyamaN., Prognostic value of the frequency of vascular invasion in stage I non-small cell lung cancer, General thoracic and cardiovascular surgery65(1) (2017), 32–39.
24.
ShimadaY.SajiH.KatoY.KudoY.MaedaJ.YoshidaK.HagiwaraM.MatsubayashiJ.KakihanaM.KajiwaraN.OhiraT. and IkedaN., The Frequency and Prognostic Impact of Pathological Microscopic Vascular Invasion According to Tumor Size in Non-Small Cell Lung Cancer, Chest149(3) (2016), 775–785.