
Abstract
BACKGROUND:
Abdominal or back pain is a common symptom in pancreatic diseases. However, the role of pain in pancreatic neuroendocrine neoplasm (PNENs) has not been clarified.
OBJECTIVE:
In this study, we aimed to show the association between the pain and the grade of PNENs.
METHODS:
A total of 186 patients with pathologically confirmed PNENs were included in this study. Clinical features and histological or radiological findings (size, location, and vascular invasion and local organs invasion and distal metastasis) were collected. Logistic regression analyses were used to show the association between pain and grade of PNENs. Nomogram was developed based on associated factors to predict the higher grade of PNENs. Receiver operating characteristic (ROC) curve was used to evaluate the diagnostic performance of size and nomogram model.
RESULTS:
The prevalence of pain in the cohort was 30.6% (
CONCLUSION:
Abdominal or back pain is associated with the grade of PNENs. The nomograms based on clinical features may be a powerful numerical tool for predicting the grade of PNENs.
Abbreviations
Introduction
Pancreas is one of the main common organs for neuroendocrine neoplasms (PNENs) occurrence. PNENs account for 1% to 2% of all pancreatic neoplasms [1]. The incidence of PNENs has been increasing due to improvement of available imaging modalities [1, 2, 3]. In 2017, the updated WHO classification of gastrointestinal neuroendocrine neoplasms divided NENs into grade 1 (G1), grade 2 (G2) and well-differentiated high-grade neoplasm (PNEN G3) and poorly differentiated carcinomas (PNEC G3). PNENs grades are related to genetic changes, clinical presentations, imaging features, prognosis, and therapeutic strategies [1, 2]. Therefore, it is helpful to identify those PNENs preoperately with a higher grade for treatment planning.
Previous studies had shown that radiological features derived from magnetic resonance imaging (MRI) and computed tomography (CT) favor the identification of PNENs pathological grades [2, 4, 5, 6, 7, 8]. However, little is known on the association between clinical presentations and WHO grade of PNENs. Abdominal or back pain is a common symptom of pancreatic diseases. Some studies indicated that abdominal pain sensation in pancreatic diseases may be used as an additional diagnostic tool to estimate pancreatic tumor and patient’s prognosis [9, 10, 11]. Many studies showed the association between pain and chronic pancreatitis or pancreatic cancer [12, 13, 14, 15]. Little is known on the relationship between abdominal pain and PNENs. Zaidi et al. showed that pain may be related with PNENs recurrence in univariate analysis [3]. However, the association between pain and PNENs grade is not clear. Nerve invasion, which may be a cause of pain in pancreatic cancer [16], is not uncommon in PNENs [17]. Therefore, the purpose of our study was to determine the association between the abdominal or back pain and PNENs grade and to develop nomogram models to predict higher grade of PNENs.
Materials and methods
Patients
A total of 204 patients with pathologically diagnosed PNENs were identified between January 2011 and July 2020. Ten patients was excluded due to the missing information of clinical symptom or histological grade. Eight patients underwent biopsy were excluded because the limitations of nerve invasion evaluation. Finally, 186 patients were included for further analysis. Demographic information and clinical symptoms were obtained from the medical database. Pain was evaluated based on a 6-point Likert scale: no pain, very mild, mild, moderate, severe, and very severe. The pain assessments were performed by patients via self-report.
There are 89 males and 97 females. All patients were divided into two groups based on the presence or absence of abdominal or back pain: non-pain group (
Histopathologic analysis
Histopathologic analysis was performed based on the pathology report. The following information was collected: lymph node invasion, vascular invasion (vein and arteries), local organs invasion and nerve invasion. Distal metastasis was evaluated by radiological examinations. In accordance with the updated 2017 World Health Organization classification, the PNENs were classified as G1 (
The characteristic of subjects with or without abdominal pain
The characteristic of subjects with or without abdominal pain
The tumor size and ki67 index in pancreatic neuroendocrine neoplasms with or without pain.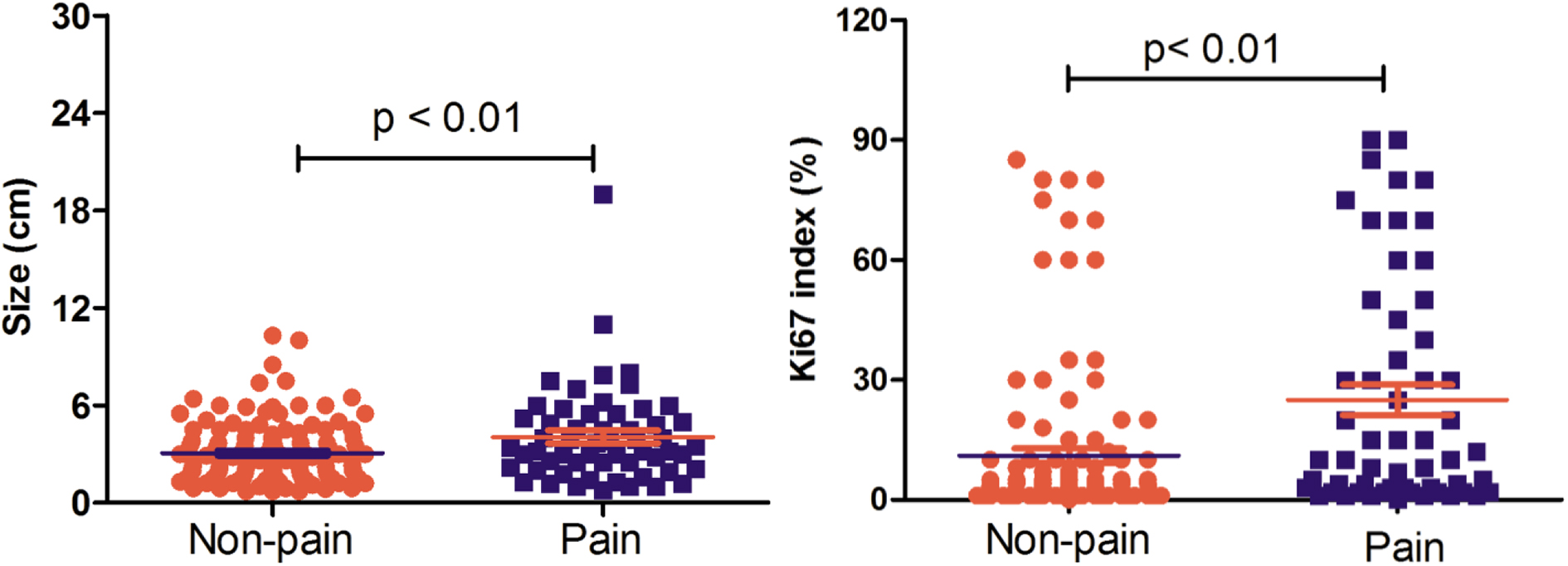
All statistical analyses were performed with commercially available software (SPSS 20.0 Chicago, III, USA). Quantitative data with normal distribution were presented as means
Results
Patients characteristics
The symptom of pain was mild or moderate in our patients, which persisted for more than one week. Patients characteristics are shown in Table 1. Vascular invasion (
The association between pain and PNENs grade
Linear regression test showed that there were no collinearity between pain and tumor size (VIF
The association between pain and G2/G3 grade of pancreatic neuroendocrine neoplasms
The association between pain and G2/G3 grade of pancreatic neuroendocrine neoplasms
Model 1 was adjusted with location. Model 2 was further adjusted with lymph node, vascular, nerve invasion and local organs invasion and distal metastasis. CI: confidence interval; OR: odds ratio.
The association between pain and G3 grade of pancreatic neuroendocrine neoplasms
Model 1 was adjusted with location. Model 2 was further adjusted with lymph node, vascular, nerve invasion and local organs invasion and distal metastasis. CI: confidence interval; OR: odds ratio.
The association between pain and PanNEC
Model 1 was adjusted with location. Model 2 was further adjusted with lymph node, vascular, nerve invasion and local organs invasion and distal metastasis. CI: confidence interval; OR: odds ratio; PanNEC: pancreatic neuroendocrine carcinoma.
The association between pain and G2/G3 or G3 grade of pancreatic neuroendocrine neoplasms in patients younger than 70 years old (
Model was further adjusted with location, lymph node, vascular, nerve invasion and local organs invasion and distal metastasis. CI: confidence interval; OR: odds ratio.
We also showed the association between pain and G2 PNENs. Multiple logistic regression showed a weak association between pain the G2 tumor (OR
Pain was also associated with PNEC (OR
Subgroup analysis in patients younger than 70 years old also showed that pain was associated with G2/G3 (OR
The nomograms for predicting G2/G3 (A) or G3 (B) pancreatic neuroendocrine neoplasms (PNENs). Age, tumor size and pain was adopted in identifying G2/G3 tumor; age, tumor size (1, 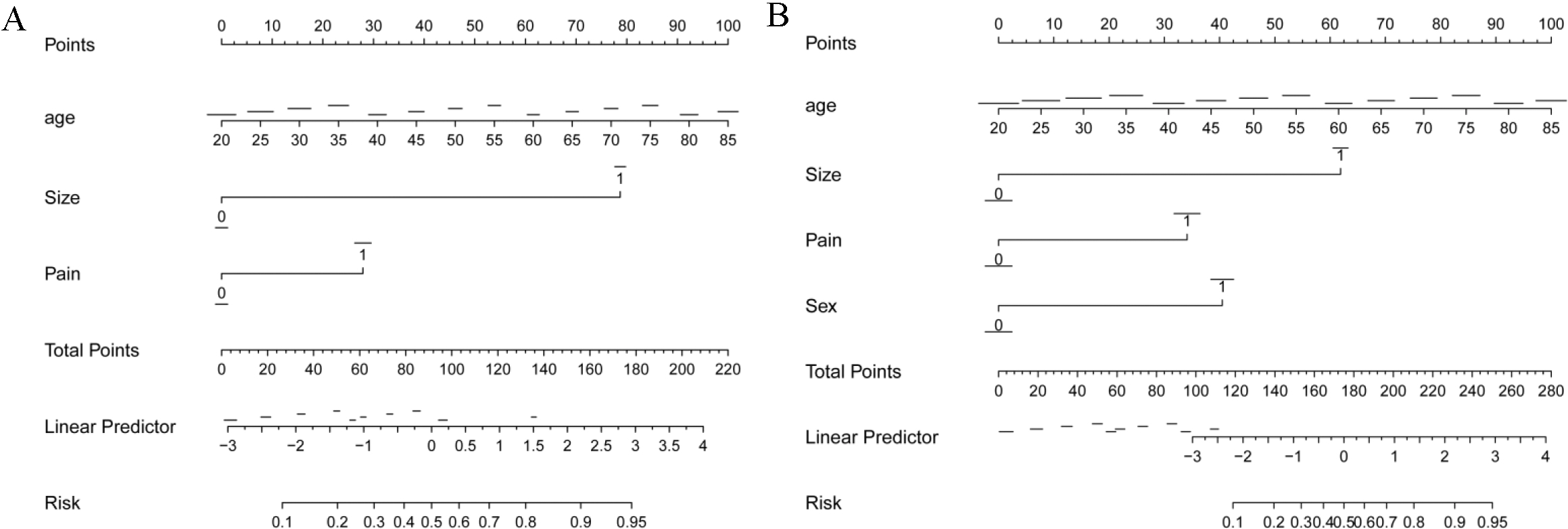
Receiver operating characteristic (ROC) curve for tumor size and nomogram in predicting G3 (A) or G2/G3 (B) pancreatic neuroendocrine neoplasms.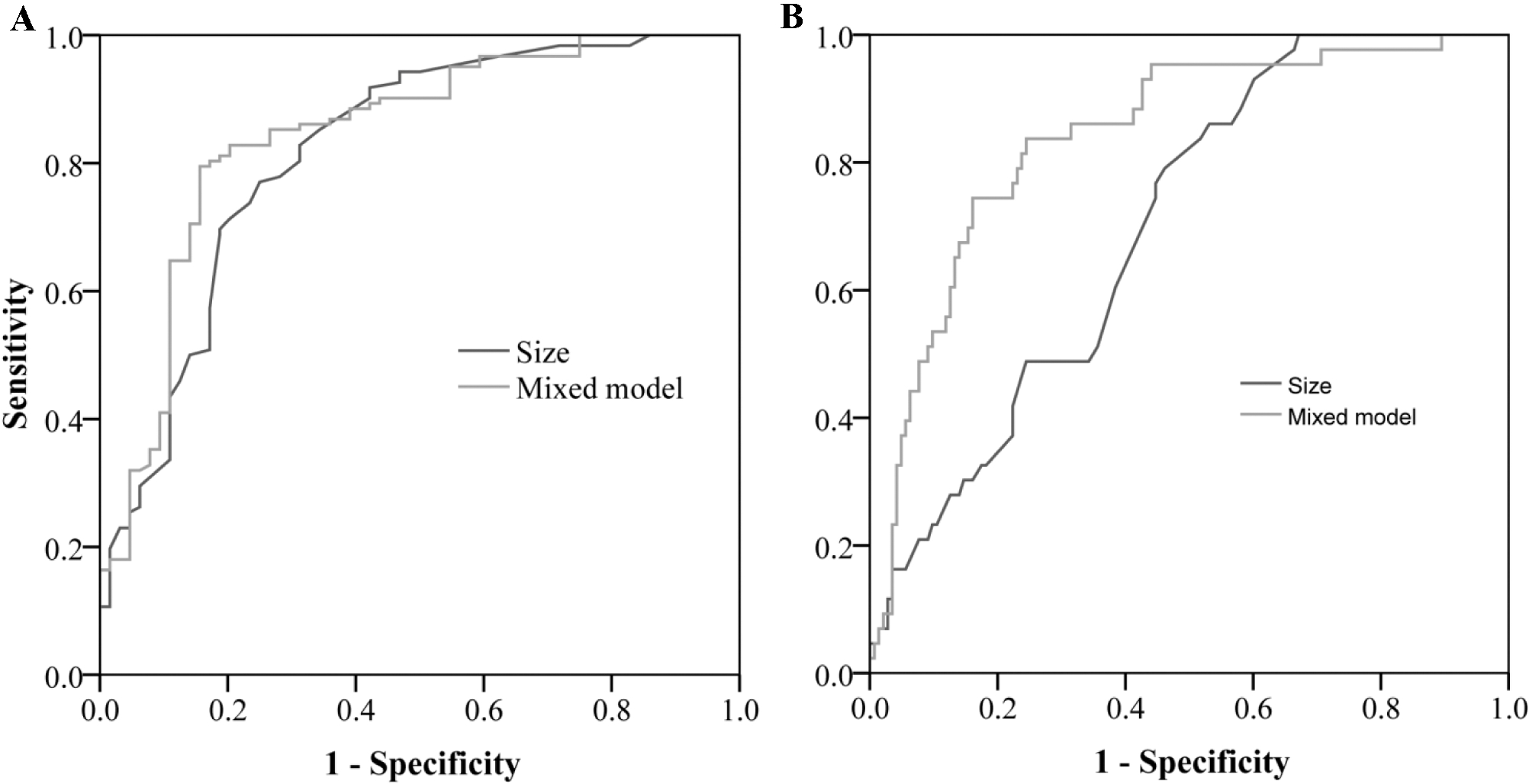
To visualize the multivariate logistic regression, the nomogram model was constructed in predicting the G2/G3 PNENs (Fig. 2A) or G3 PNENs (Fig. 2B). The performance of the nomogram was measured by the area under the ROC curves (AUC). In the prediction of G2/G3 PNENs, the AUC of the nomogram model was 0.84 (95% CI, 0.77–0.91), and the AUC of tumor size was 0.70 (95% CI, 0.62–0.78). The AUC value revealed a high performance of tumor grade discrimination using the combined nomogram (Fig. 3). Similar results were observed in nomogram model in predicting the G3 PNENs. The AUC of the nomogram was 0.84 (95% CI: 0.78–0.91) which was higher than the AUC of tumor size (AUC
The pathological grade of PNENs is marked related with the treatment strategies and the prognosis [1]. Many studies have shown that the medical images and the radiological texture analysis are valuable for the identification of PNENs grade [4, 5, 6, 7, 8]. However, there are few studies reported the association between clinical presentations and PNENs grade, especially the common symptom in pancreatic diseases, abdominal pain. In this study, we found that abdominal pain was the independent predictors of G2/G3, G3 PNENs or PanNEC. In addition, we also developed two nomogram models based on pain and other clinical characteristics which showed high performance to predicting the G2/G3 or G3 PNENs.
Some studies reported that tumor cells can invade the perineurium in the pancreatic ductal adenocarcinoma (PDAC) [10, 14, 16]. Several studies also showed nerve invasion is common in PNENs [17, 18, 19]. The incidence of nerve invasion was ranged from 10% to 20.0% in PNENs. Our data was 9.7% (17 cases) which was slightly lower than previous published data. Many factors may affect the incidence, such as sample size and number of low grade PNENs. The mechanism of nerve invasion in PNENs has not been clarified. In our study nerve invasion was significantly associated with a higher grade of PNENs (data not shown). PanNEC shares some common features with PDAC [20]. We speculated that PanNEC cells may have similar biological behaviors with PDAC, including nerve invasion. In addition, the high proliferation ability of G2/G3 tumor may also enhance nerve invasion. How PNENs cells, especially for PanNEC cells, invade nerve need further exploration.
The association between pain and nerve invasion in PDAC has been reported in many studies [16, 21]. Our data indicated that pain was associated with PNENs grade. Nerve invasion may play critical role because our data showed a weak association between nerve invasion and pain in PNENs (OR
Nomogram is one of the widely accepted models in clinical studies to predict treatment efficiency, cancer recurrence and prognosis, which can provides a rapid and simple graphical interpretation of numeric statistics [22, 23]. Moreover, nomogram can calculate individual risk by synthetically considering all independent risk factors and give individualized predictions [24, 25]. Previous studies suggested the combined nomogram model for preoperative prediction of the PNENs grade may facilitate the treatment and affect prognosis [4, 26]. Therefore, we developed nomogram models which is beneficial to personalized treatment decisions to predict the grade of PNENs. Age, tumor size and pain were the determinant factors in our model. Our model had acceptable performance. Some studies also reported that the size is good indicator in the differentiation PNENs grade or malignancy [27, 28, 29, 30, 31, 32]. Our results were similar with the previous reports. Moreover, our data showed the combination model was better than model using size alone in identifying G2/G3 PNENs. Our study supplied a tool for physicians to simply predict PNENs grade. The physicians may make a treatment plan based on our model. However, the final diagnosis of tumor grade should be based on histological examinations. Our study provided a reference for the clinical diagnosis and treatment.
Our study has several limitations. First, we did not perform an external validation because we did not have additional independent population. Second, the image features (such as the enhanced images) and the clinical data (such as the chromogranin A, CgA) were not included. Third, the sample size in our study was not large. A study with large sample size is need to confirm our findings. Fourth, we divided G3 PNENs into PanNEN G3 and PanNEC G3 only based on the ki67 index (
In conclusion, our study is the first one to report an association between abdominal or back pain and the grade of PNENs. This study has identified pain might be an associated factor of the grade of PNENs. We also identified several independent risk factors (sex, age and size) to develop a nomogram model for predicting the grade of PNENs. Our data showed that nomograms based on clinical information may be a powerful numerical tool for predicting the grade of PNENs. Further studies are needed to confirm our nomogram model.
Funding
This study was funded by Jiangsu Provincial Hospital of Chinese Medicine Peak Academic Talent Project (NO: y2018rc04) and Medical development and Medical Assistance Foundation of Jiangsu Province Hospital of Chinese Medicine.
Author contributions
Conception: Xiao Chen and Zhongqiu Wang.
Interpretation or analysis of data: Cheng Wang, Tingting Lin, Xin Chen and Wenjing Cui.
Preparation of the manuscript: Cheng Wang, Tingting Lin and Xin Chen.
Revision for important intellectual content: Xiao Chen, Xin Chen and Zhongqiu Wang.
Supervision: Xiao Chen.
Footnotes
Acknowledgments
None.
Conflict of interest
The authors declare that they have no conflict of interests.