
Abstract
BACKGROUND:
EGFR mutations widely exists in NSCLC patients, which are involved in cancer development.
OBJECTIVE:
The function of EGFR mutations in the resistance to TKI treatments of NSCLC was evaluated to provide theoretical support for the clinical management of NSCLC patients.
METHODS:
A total of 150 NSCLC patients including 118 patients with EGFR mutation and 32 without, were included in this study. The EGFR mutation status and subtypes were analyzed in recruited patients. The distribution of EGFR mutation subtypes and their association with clinicopathological features were also assessed. The prognostic value of EGFR mutation was evaluated by the overall survival of recruited patients. The function of EGFR mutation was estimated, in vitro, in the TKI resistant NSCLC cells with different subtypes of EGFR mutation.
RESULTS:
The exon 19 deletion was the most common subtype of EGFR mutation in the enrolled patients followed by the exon 21 L858R point mutation. The EGFR mutations were closely associated with the differentiation degree and the histological types of NSCLC cases. EGFR mutation was an independent prognostic factor of NSCLC with a close relationship with the overall survival of patients. The exon 20 T790M mutation results in the erlotinib resistance through the PI3K/Akt signaling pathway.
CONCLUSIONS:
The EGFR mutation is a critical factor in the prognosis and for the resistance to TKI treatment in NSCLC. The exon 20 T790M mutation was involved in the erlotinib resistance through PI3K/Akt signaling pathway.
Introduction
Non-small cell lung cancer (NSCLC) is a major histologic group of lung cancer accounting for 75–80% of all lung cancer, with increasing incidence and high mortality rates [1]. Most patients with NSCLC are diagnosed at an advanced stage and therefore are not eligible for surgical resection [2]. The lack of effective indicators of NSCLC development is the major cause of recurrence, metastasis, and resistance, which are closely associated with poor outcomes in patients [3]. Statisticsal evidence indicates that patients who develop recurrence or resistance show poor prognosis, with the latter showing a median survival of only 8–10 months [4].
Epidermal growth factor receptor (EGFR), a receptor tyrosine kinase, expressed in epithelial cells, has been reported to be aberrantly activated in tumor cells [5]. Furthermore, EGFR mutationis a major factor which is involved in the development of cancers [6]. The exon 19 deletion mutation, exon 21 L858R point mutation, and exon 20 T790M mutation are the most common and classical subtypes of EGFR mutations [7]. EGFR is among the most frequently mutated genes in NSCLC, making it a critical therapeutic target, and various agents targeting EGFR-mediated signaling have been employed in the clinical treatment of NSCLC [8, 9]. Currently, EGFR-tyrosine kinase inhibitor (EGFR-TKI) is considered the standard therapeutic strategy for patients with NSCLC in an advanced stage [10]. Emerging evidence suggested that TKIs were relatively safe and more effective than chemotherapy in NSCLC cases with EGFR mutations and they have been demonstrated to significantly improve the survival of such patients [10, 11, 12, 13, 14, 15]. However, resistance to TKI is a major issue that needs to be addressed to improve patient outcomes [16].
EGFR mutations have been reported to affect TKI resistance in previous studies, although the underlying mechanism remains unclear [17]. In this study, the clinical significance of three major EGFR mutations (exon 19 deletion mutation, exon 21 L858R point mutation, and exon 20 T790M mutation) was explored, and their role in TKI resistance and the potential underlying mechanism were investigated in vitro. This study is expected to provide novel insights into the application of EGFR inhibitors to improve NSCLC treatment efficiency.
Materials and methods
Patients
This study obtained approval from the Ethics Committee of Affiliated People’s Hospital of Jiangsu University. A total of 150 NSCLC patients were included in this study from 2013 to 2015. Among the enrolled patients, a total of 118 patients diagnosed with EGFR mutant-positive advanced or recurrent NSCLC received first/second-generation EGFR-TKI treatments, and another 32 NSCLC patients were confirmed as EGFR wild-type. The clinical information of all patients was completed and available. A 5-year follow-up survey was conducted to obtain the survival information of the participants. Serum samples were collected from each patient and stored in liquid nitrogen at
EGFR mutation analysis
The EGFR mutations were detected by a Scorpion Amplification Refractory Mutation System, a highly sensitive PCR-based test system covering 29 EGFR mutations from exon 18 to exon 21. DNA was extracted from collected samples with the help of Qiagen QIAamp Circulating Nucleic Acid Kit (Qiagen, Germany). According to the manufacturer’s protocol, the assay was performed with 80 ng DNA and the EGFR 29 Mutation Detection Kit (Amoy Diagnostics, China).
Cell culture and cell transfection
A549 (EGFR wild-type), PC9 (exon 19 deletion mutation), H1975 (exon 20 T790M mutation), and H3255 (exon 21 L858R point mutation) cell lines were obtained from American Type Culture Collection. All cells were cultured in RPMI 1640 medium (Invitrogen, USA) supplemented with 10% fetal bovine serum (FBS) at 37
Cells were transfected with pcDNA 3.1-EGFR or EGFR-siRNA using Lipofectamine 2000 Reagent (Thermo Fisher Scientific, Inc.) following the manufacturer’s instructions, to overexpress or silence EGFR, respectively.
Erlotinib resistance assessment
Cells (A549, PC9, H1975, and H3225 cells) were seeded into 96-well plates supplemented with FBS containing the culture medium supplemented with FBS and exposed to various concentrations of erlotinib. After incubation for 0, 24, 48, and 72 h, CCK8 reagent (Dojindo, Japan) was added to each well, followed by a 1-h incubation. Thereafter, the absorbance at 450 nm of each well was detected using a microplate reader. The IC
Association of EGFR mutations with the clinicopathological features of NSCLC cases and the distribution of major subtypes of EGFR mutations
Association of EGFR mutations with the clinicopathological features of NSCLC cases and the distribution of major subtypes of EGFR mutations
TKI: tyrosine kinase inhibitor.
The transfected cells were collected in the PBS buffer solution and lysed with RIPA buffer (Life Technologies, USA). The proteins were transferred to a polyvinylidene fluoride (PVDF) membrane for 2 h and then blocked with 5% nonfat milk for 1 h. Thereafter, the membrane was incubated with the primary antibody at 4
Statistical analysis
All data are represented as mean value
The Kaplan-Meier curves of NSCLC patients with (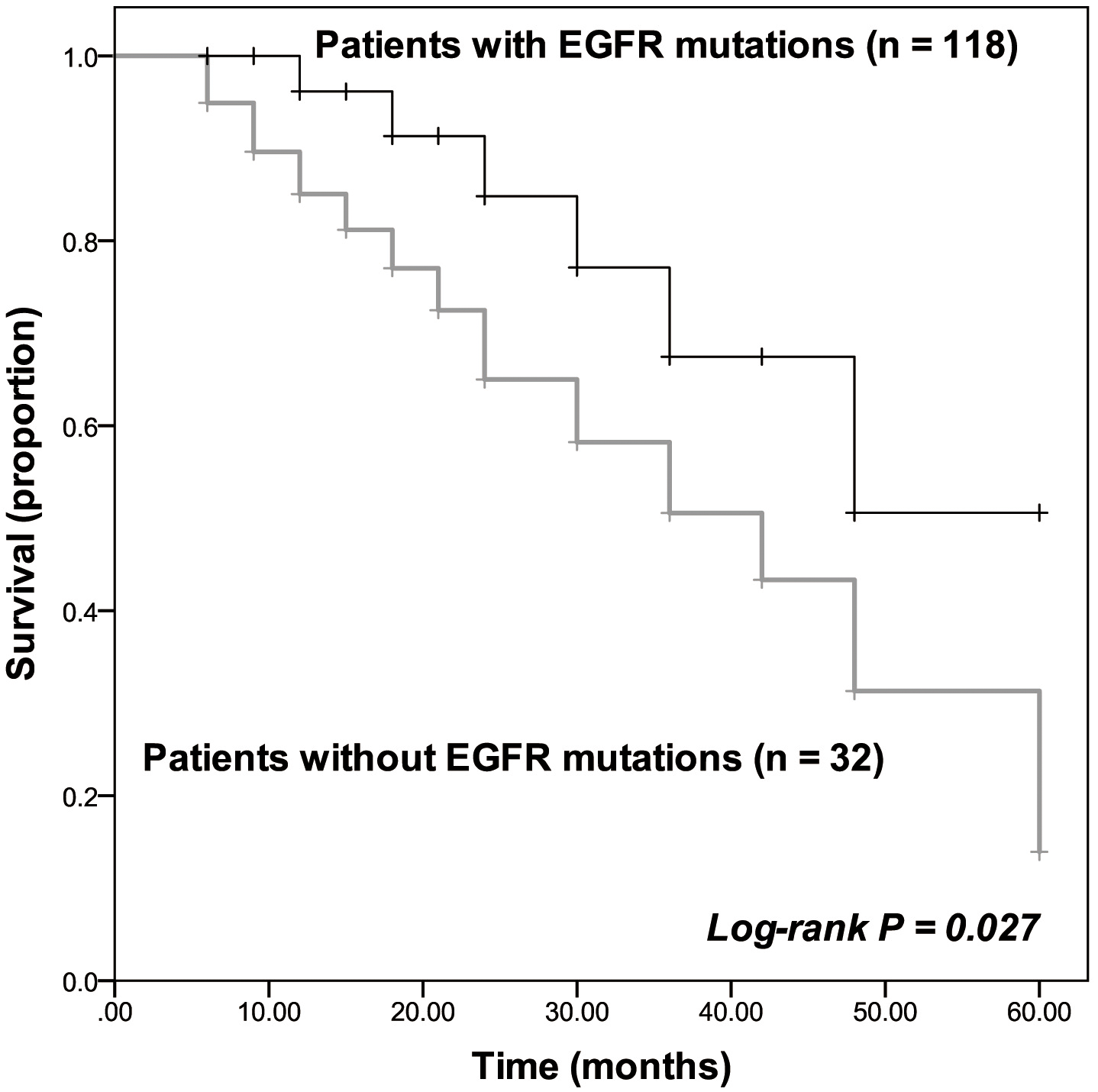
The dose-dependent experiments of erlotinib in A549 (A), PC9 (B), H1975 (C), and H3255 (D) cells. The inhibition of cell viability by erlotinib was dose-dependent with the IC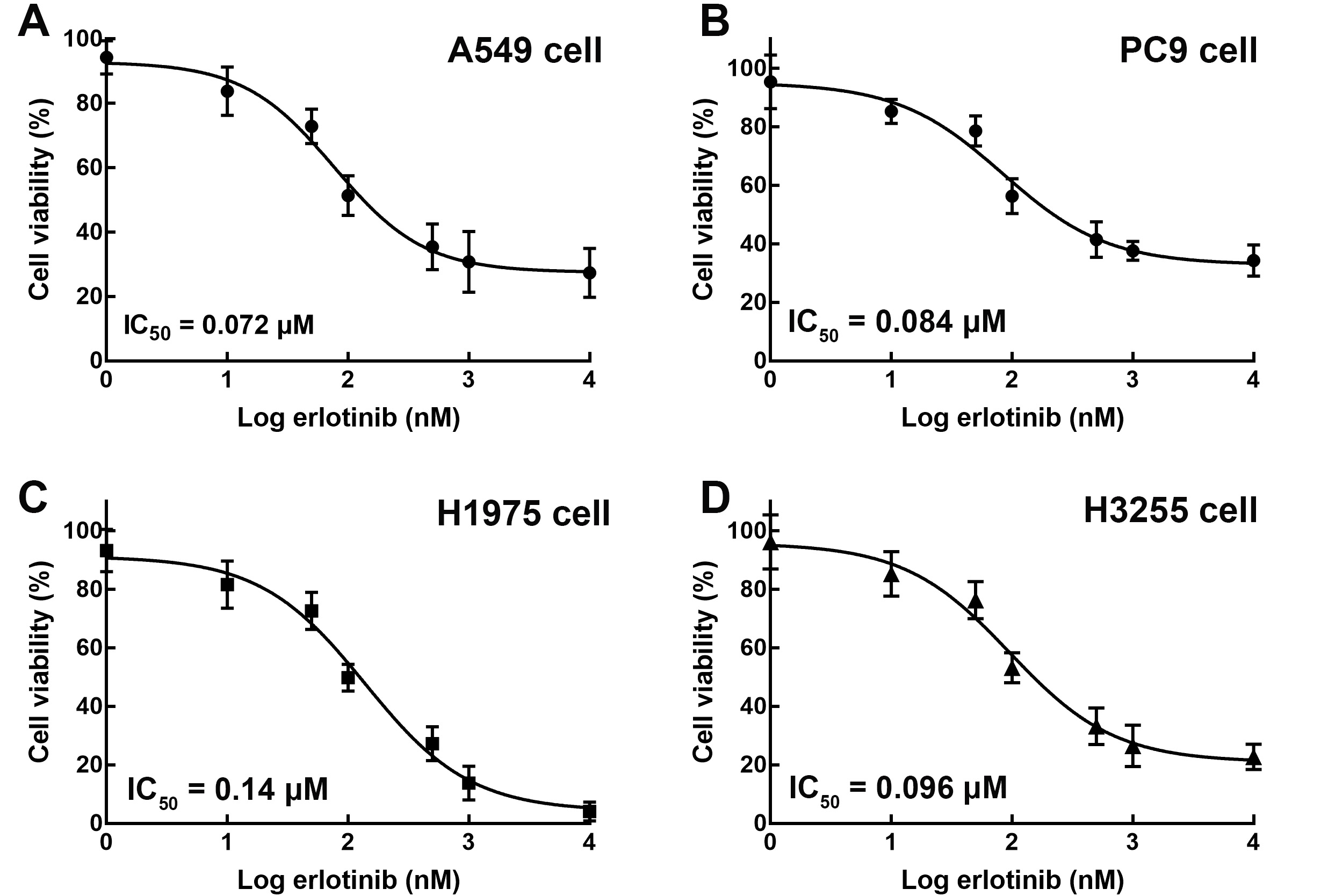
EGFR mutations were closely associated with the degree of differentiation and the histological subtypes of NSCLC cases
The clinical features of the recruited NSCLC patients are summarized in Table 1. Of the recruited 150 patients, 118 found to possess EGFR mutations and 32 without EGFR mutations. The EGFR mutantion subtypes were exon 19 deletion (
Effect of erlotinib on the proliferation of A549 (A), PC9 (B), H3255 (C), and H1975 (D) cells. The proliferation of A549, PC9, and H3255 cells was dramatically inhibited by the treatment of erlotinib, while H1975 was not affected by erlotinib. 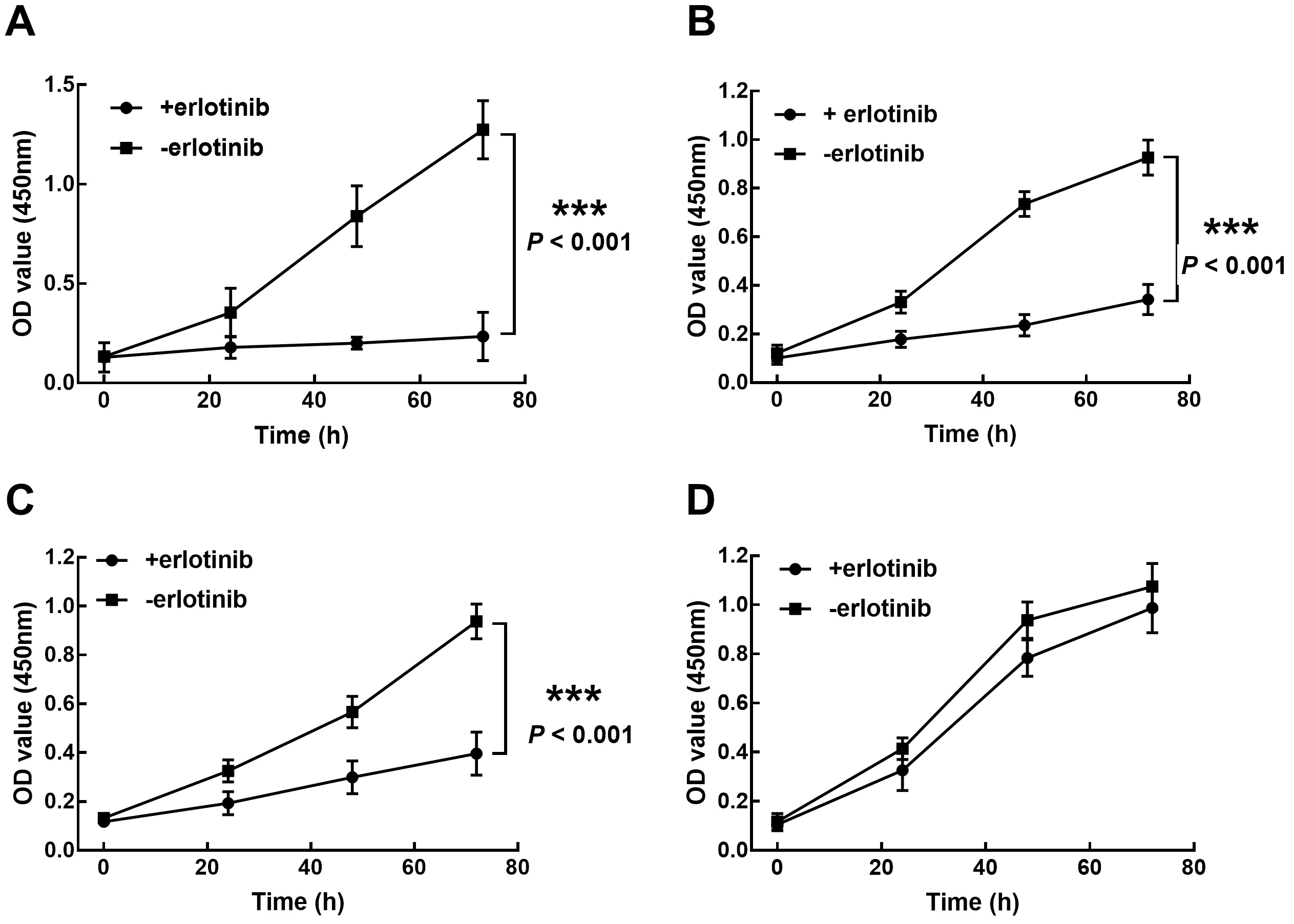
Effect of EGFR on the expression level of PI3K, Akt, p-Akt with 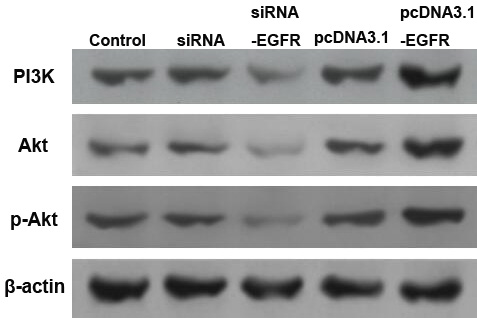
The survival of the recruited patients has been depicted by the Kaplan-Meier curve. Patients without any EGFR mutation showed a relatively poorer survival rate than those with EGFR mutation (log-rank
Association of EGFR mutation with the overall survival of NSCLC patients
Association of EGFR mutation with the overall survival of NSCLC patients
NSCLC cell lines with different EGFR mutation subtypes were employed to evaluate the function of EGFR mutation in erlotinib resistance. In the presence of various concentrations of erlotinib, the H1975 cell (exon 20 T790M mutation) showed a relatively higher IC
EGFR is involved in erlotinib resistance through the PI3K/Akt signaling pathway
The knockdown of EGFR in H1975 cells showed a notable inhibitory effect on the expression level of PI3K and Akt proteins. In contrast, the overexpression of EGFR enhanced the PI3K and Akt levels (Fig. 4). Therefore, it was speculated that EGFR participated in the resistance to erlotinib through the PI3K/Akt signaling pathway.
Discussion
In clinical practice, TKIs such as gefitinib, erlotinib, and osimertinib, are included in effective therapeutic strategies for NSCLC patients, reducing progression and improving the overall survival [18]. However, resistance is a serious problem that affects therapeutic efficiency and threatens patients’ outcomes. EGFR mutations have been considered a favorable predictive factor of TKI treatment efficiency [15, 19, 20]. Understanding the mechanism between EGFR mutation and TKI resistance could provide theoretical support for the clinical management of patients with NSCLC.
A majority of patients with NSCLC have been reported to harbor EGFR mutations [21]. Consistently, in this study, 118 of 150 patients with NSCLC were revealed to possess EGFR mutations. The identified EGFR mutations were found to be closely associated with the differentiation degree and histological subtype of NSCLC, indicating the potential functional role of EGFR mutation in NSCLC progression. The exon 19 deletion was found to be the most common EGFR mutation subtype in the present study, followed by exon 21 L858R point mutation, which is consistent with previous studies [7]. A comparison of the survival between patients with or without EGFR mutations showed that those with the mutations were associated with better overall survival and EGFR mutation was also demonstrated to be a critical factor in the prognosis of patients. There have been conflicting reports regarding the prognostic role of EGFR mutations. Liu et al. focused on the association between EGFR mutation and the prognosis of 131 patients with lung adenocarcinoma and found that the mutations did not have significant prognostic value but were associated with other positive prognostic factors [22]. Contrastingly, Izar et al. showed that EGFR mutations and tumor size are significant prognostic factors in NSCLC, which is consistent with the present results [23]. In this study, the patients with EGFR mutations received TKI treatments; hence, the difference in the survival between patients with and without EGFR mutations was speculated to be an effect of TKIs. In fact, determining the recurrence-free survival rates of patients ia a more reasonable method to evaluate the prognostic value of a specific biomarkerand this should be investigated in future studies [24].
Different EGFR mutations showed different resistance to TKI treatments [25]. In previous studies, H3255 has been demonstrated to be sensitive to TKI treatment, with the cell viability being almost totally suppressed by gefitinib [26]. H1975 cells showed relatively high resistance to erlotinib, as their proliferation was unaffected by erlotinib, which significantly inhibited the viability of PC9 and H3255 cells. Therefore, erlotinib may be ineffective for patients with NSCLC with exon 20 T790M mutation. The exon 20 T790M mutation was reported to increase the affinity for ATP, which may cause erlotinib resistance in the H1975 cell [27]. Additionally, the PI3K/Akt signaling pathway was demonstrated to be regulated by EGFR, which was hypothesized as the potential molecular mechanism underlying the function of EGFR mutation in erlotinib resistance.
The relatively small sample size, which might affect the results, is a limitation of the current study. Therefore, a larger sample size is needed in future investigations to verify the present conclusion. Furthermore, due to the heterogeneity of different EGFR mutations, the mechanism underlying the function of other EGFR mutation subtypes needs to be explored.
From the above findings, study shows that the EGFR mutations are closely associated with the clinical features and prognosis of patients with NSCLC. The incidence of exon 19 deletion is higher than that of exon 21 L858R and exon 20 T790M mutations. Importantly, the exon 20 T790M mutation mediates erlotinib resistance through the EGFR/PI3K/Akt signaling pathway.
Author contributions
Conception: Hao Ding and Yuxing Chen.
Interpretation or analysis of data: Yuanyang Zhao and Li Zhu.
Preparation of the manuscript: Huaying Huang and Chenyang Liu.
Revision for important intellectual content: Feng Zhang and Cunxi Zhang.
Supervision: Cheng Jin.
Funding
This study was supported by Zhenjiang Social Development Project (No. SH2018077).
Footnotes
Acknowledgments
Not applicable.