
Abstract
BACKGROUND:
The 21-gene recurrence score (RS) assay has been validated to predict the risk of disease-free survival in estrogen receptor (ER)-positive, human epidermal growth factor receptor 2 (HER2)-negative early breast cancer patients. However, its relation with locoregional recurrence (LRR) risk is unclear.
OBJECTIVE:
This study aimed to explore the ability of RS to predict LRR risk.
METHODS:
Consecutive ER-positive, HER2-negative, pT1, pN0-1, and M0 early breast cancer patients were analyzed retrospectively. According to RS, patients were divided into low- (RS
RESULTS:
A total of 1558 patients were enrolled: 354 (22.7%), 788 (50.6%), and 416 (26.7%) patients in the low-, intermediate-, and high-risk groups, respectively. The median follow-up time was 53 months, and 2, 8, and 14 LRR events were observed in the low-, intermediate-, and high-risk groups, respectively (
CONCLUSION:
The 21-gene RS assay was significantly associated with the risk of LRR in ER-positive, HER2-negative early breast cancer patients. Among patients with different nodal statuses and patients receiving mastectomy, RS remained predictive of the risk of LRR.
Abbreviations
Introduction
Breast cancer is a group of heterogeneous diseases that has various biological and clinical characteristics. Therefore, identifying early breast cancer patients with a high risk of recurrence and selecting the optimal therapy are of great importance [1]. Currently, the treatment decision-making of early breast cancer patients still relies largely on traditional clinical and pathological characteristics. While personalized treatment is increasingly emphasized, integrating multigene assays into early breast cancer patient care has gained growing research interest.
Among estrogen receptor (ER)-positive, human epidermal growth factor receptor 2 (HER2)-negative early breast cancer patients, the 21-gene recurrence score (RS) assay has become one of the most commonly used multigene assays [2, 3]. Several studies have demonstrated the predictive value of 21-gene RS for distant metastasis in both lymph node negative and positive patients [4, 5]. RS was recommended by both the National Comprehensive Cancer Network (NCCN) and American Society of Clinical Oncology (ASCO) guidelines in the management of ER-positive, HER2-negative early breast cancer patients.
Locoregional recurrence (LRR) is a significant predictor of distant recurrence among breast cancer patients [6, 7]. Currently, the risk of LRR is mainly evaluated according to traditional clinicopathological factors (including patient age, tumor grade, TNM stage, and molecular subtypes). However, the association of LRR and multigene assays remains controversial. Studies exploring the association between RS and LRR risk have reached different conclusions. Several researchers found that RS was a significant predictor of LRR in both node-negative and node-positive patients [8, 9, 10], while some found no significant association between RS and the risk of LRR [11]. And some had found that applying a 21-gene RS assay with different cutoffs could be predictive of LRR [12]. Meanwhile, with the development of comprehensive treatment, the prognosis of breast cancer has been improved a lot in the past decades, including a decrease in the LRR [13, 14].
Based on the above issues, our study aims to evaluate the relationship between 21-gene RS and the risk of LRR among early breast cancer patients that were treated in the modern era and to assess their association in patients with different nodal statuses and breast surgery types.
Materials and methods
Patient population
We retrospectively reviewed consecutive patients treated in Comprehensive Breast Health Center, Ruijin Hospital from January 2009 to December 2017. Female patients with pT1-pT3, pN0-pN1, M0 ER-positive, HER2-negative invasive early breast cancer were included. Other inclusion criteria included receiving either mastectomy or lumpectomy with negative margins and undergoing 21-gene RS assay testing. Patients with bilateral breast cancer, pT4 disease, metastatic breast cancer, previous exposure to systemic therapy, and previous or concurrent malignant disease were excluded from the study. The last follow-up date was 31
Study design and end points
Traditional clinicopathological factors and follow-up information were retrieved from the database, including age, type of surgery, pathology, grade, pT status, pN status, immunohistochemistry (IHC) expression of ER, progesterone receptor (PR), HER2, Ki67, RS, and date and type of events. ER expression
The primary endpoint was LRR, defined as the incidence of in-breast, ipsilateral chest wall, or regional nodal recurrence. Second endpoints included breast cancer-free interval (BCFI) and breast cancer-specific survival (BCSS). BCFI was defined as the time from surgery to contralateral breast cancer, any recurrence, any metastasis, and death from breast cancer. BCSS was defined as the time from surgery to death caused by breast cancer [24].
Statistical analysis
Log-rank tests were performed to assess the relationship between RS and the risk of LRR, BCFI, and BCSS. Kaplan-Meier estimates were conducted to demonstrate the cumulative incidence rates of LRR, BCFI, and BCSS events. Log-rank tests and Kaplan-Meier estimates were also conducted in subgroup analyses. Cox regression models were conducted to examine the prognostic value of RS and other clinicopathological factors. All statistical analyses were performed by SPSS version 18.0 (SPSS, Inc., Chicago, IL). A
Results
Patient and tumor characteristics
Overall, 1558 patients with ER-positive, HER2-negative disease were enrolled in this study (Fig. S1). Table 1 provides detailed information on the patient and tumor characteristics. At the time of diagnosis, 1070 patients (68.7%) were over 50 years old. Eight hundred ninety-seven patients (57.6%) received mastectomy, and 661 patients (42.4%) received lumpectomy. There were 1085 patients (69.6%) diagnosed with pT1 tumors and 1324 patients (85.0%) with pN0 disease. High ER and PR expression was found in 1434 patients (92.0%) and 1045 (67.1%) patients, respectively. Meanwhile, 788 patients (50.6%) had Ki-67
Patient characteristics
Patient characteristics
Abbreviations: RS, recurrence score; ER, estrogen receptor; PR, progesterone receptor; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma.
With a median follow-up time of 53 months, 24 LRR events were eventually observed among enrolled patients. Table S2 provides the detailed event type of LRR according to the 21-gene RS category. Two patients (0.6%) with low RS risk experienced LRR, while 8 (1.0%) and 14 (3.4%) patients with intermediate and high RS experienced LRR, respectively. Among the high-risk RS patients who experienced LRR, 6, 5, and 3 patients experienced local recurrence, regional recurrence, and both local and regional recurrences, respectively.
Association between 21-gene RS and LRR
Among the 1558 patients, RS was significantly associated with the risk of LRR (
Multivariate Cox regression analysis of predictors of locoregional recurrence
Multivariate Cox regression analysis of predictors of locoregional recurrence
Abbreviation: RS, recurrence score.
Locoregional recurrence (LRR) by 21-gene recurrence score (RS).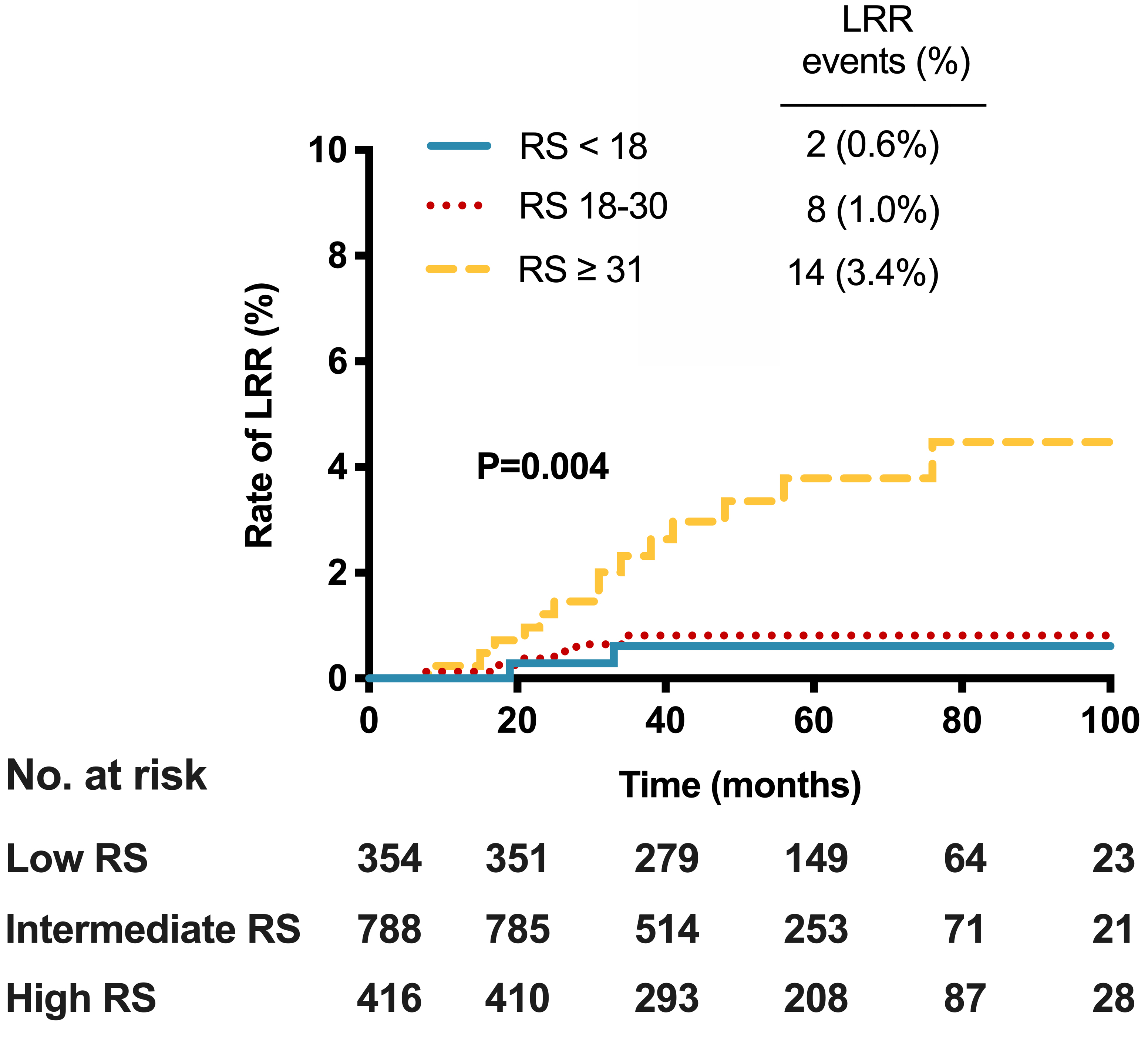
Locoregional recurrence (LRR) by 21-gene recurrence score (RS) in A) patients with pN0 disease; B) patients with pN1 disease; C) patients receiving mastectomy; D) patients receiving lumpectomy.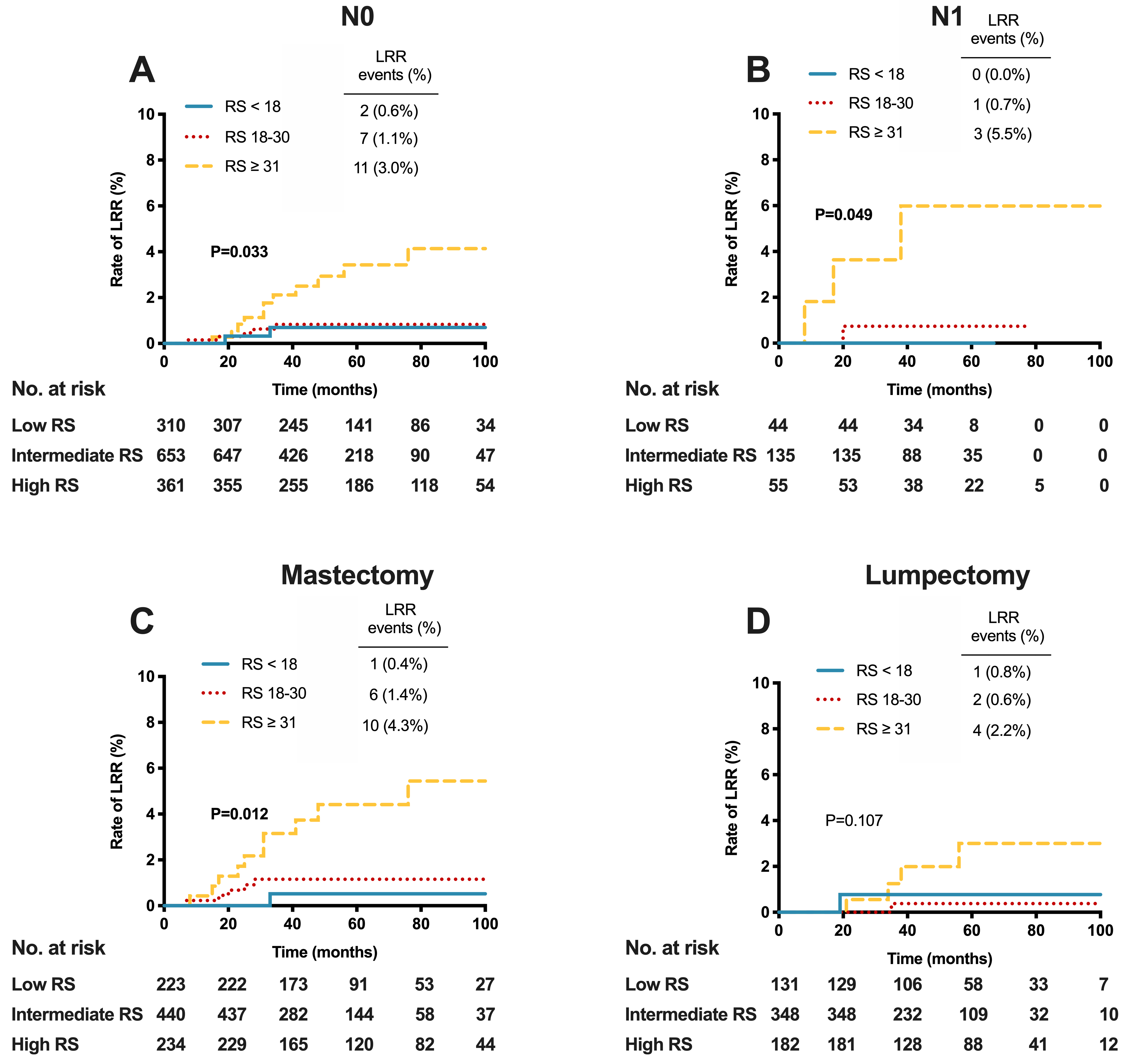
Cumulative incidence of A) breast cancer-free interval (BCFI) and B) breast cancer-specific survival (BCSS) events by 21-gene recurrence score (RS).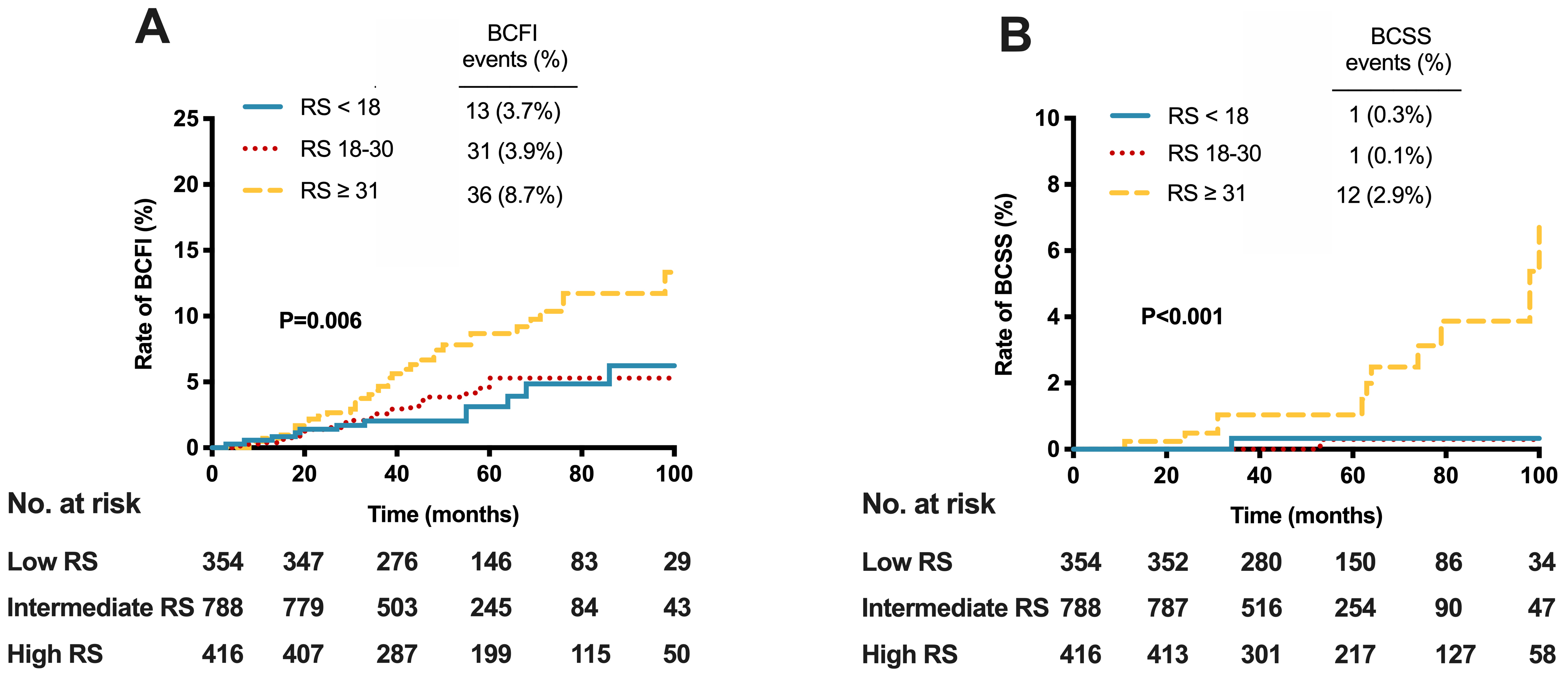
The associations between RS and LRR according to different nodal statuses and breast surgery types are listed in Fig. 2. In node-negative patients, there were 2 (0.6%), 7 (1.1%), and 11 (3.0%) LRR events in the low-, intermediate-, and high-risk RS groups, respectively (
Eventually, a total of 80 patients experienced BCFI (breast cancer-free interval, defined as the time from surgery to contralateral breast cancer, any recurrence, any metastasis, and death from breast cancer) events, and 14 patients experienced BCSS (breast cancer-specific survival, defined as the time from surgery to death caused by breast cancer) events (Fig. 3). The cumulative incidence rate of BCFI was 3.7%, 3.9%, and 8.7% for low, intermediate, and high RS patients, respectively (
Discussion
Our study, including 1558 consecutive patients with 21-gene RS results, demonstrated that 21-gene RS was significantly correlated with the risk of LRR among ER-positive, HER2-negative early breast cancer patients. Patients with high RS were at greater risk of LRR than patients with low RS. Moreover, among pN0 or pN1 patients and patients receiving mastectomy, RS remained associated with LRR.
While early breast cancer patient care requires increasing individualization, adjuvant treatment decision-making has been increasingly guided by tumor biological characteristics. Since 21-gene RS has been proven to predict distant recurrences, researchers have explored the association between RS and LRR. Mamounas et al. first found that RS could predict the risk of LRR in node-negative patients [8]. Subsequently, they confirmed a similar association between RS and LRR in node-positive patients [9]. In contrast, Solin et al. found that RS failed to predict LRR in the whole cohort but was related to the risk of LRR when RS was calculated as a continuous variable among the hormonal receptor-positive subgroup [11]. Moreover, Jegadeesh et al.’s study demonstrated that 21-gene RS
Currently, the value of postmastectomy radiotherapy (PMRT) among pN1 patients is still controversial [9, 25]. Russell et al. pointed out that although the survival benefit from additional PMRT had been confirmed in some studies [26], the development of effective systemic therapy had improved the outcome of pN1 disease and reduced the magnitude of PMRT’s value [27]. Current studies have come to various conclusions in terms of PMRT in pN1 patients [13, 28, 29, 30]. Therefore, further subgroup analyses were conducted in different node or breast surgery subgroups. In both pN0 (
The overall incidence rate of LRR was 1.5% in our study, which was relatively low compared with previous studies. One reason may be the relatively short follow-up time, which may be considered a limitation of our study. However, the 2005 EBCTCG overview demonstrated that approximately three-quarters of the LRRs occurred in the first 5 years after randomization [26]. The 25-year follow-up analysis of the NSABP B-04 trial showed that 81.6% and 89.5% of LRRs occurred during the first 5 years for pN0 and pN1 patients receiving mastectomy, respectively [31]. Another possible explanation for the low LRR incidence rate might be the late surgery year (2009–2017) compared with previous studies, such as Mamounas’s study, which enrolled patients treated in the 1980s and 1990s. During our study period, adjuvant treatment, including chemotherapy such as anthracycline or taxane, radiotherapy, and endocrine therapy such as aromatase inhibitor, was well developed, and effective systemic therapy was standardly administered in our center. Modern treatment advances have been proved to improved disease outcome including LRR. McBride et al. found that PMRT reduced the rate of LRR in patients treated in the early era (1978–1997), while failed to benefit patients treated in the later era (2000–2007) [14]. As Mamounas’s study was derived from the NSABP B-14 and B-20 trials, patients who received different treatment strategies were included (chemotherapy plus tamoxifen, tamoxifen alone, or placebo alone), leading to a high overall incidence of LRR (8.4%) compared with our study, where enrolled patients were treated with endocrine therapy plus chemotherapy when appropriate. As the effectiveness of local and systemic treatment increases, better LRR control has been achieved; thus, it is important to accurately weigh the absolute benefit from excess local treatment against potential toxicity. Finally, the retrospective study design and single-center patient cohort may be considered other limitations of this study.
In conclusion, this study demonstrated that RS was significantly associated with the risk of LRR for ER-positive, HER2-negative early breast cancer patients, and among patients with different nodal statuses and patients receiving mastectomy, RS remained predictive of the risk of LRR, which may be used to guide future individualized local therapy.
Author contributions
Conception: XC, KS and YZ.
Interpretation or analysis of data: YZ, WG and XC.
Preparation of the manuscript: YZ and WG.
Revision for important intellectual content: YZ, WG, XC and KS.
Supervision: XC and KS.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/CBM-210274.
sj-docx-1-cbm-10.3233_CBM-210274.docx - Supplemental material
Supplemental material, sj-docx-1-cbm-10.3233_CBM-210274.docx
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81772797); Shanghai Municipal Education Commission – Gaofeng Clinical Medicine Grant Support (No. 20172007); and Ruijin Hospital, Shanghai Jiao Tong University School of Medicine – “Guangci Excellent Youth Training Program” (No. GCQN-2017-A18). The funders had no role in the study design, data collection, data analysis, article writing, or article submission.