
Abstract
Background
Radical mastectomy remains the cornerstone procedure for the treatment of breast cancer (BC). However, traditional radical surgeries often lead to complications such as local numbness, pulling sensations, and atrophy of the pectoralis major muscle. In contrast, BC radical surgeries that preserve more tissue have shown potential in reducing these complications. This retrospective study aims to analyze case data from our institution, focusing on the methods of surgeries that preserve more tissue and evaluating the safety and reliability of the follow-up results.
Methods
A retrospective observational study was conducted on cases diagnosed with BC between May 2018 and July 2019 at our institution. The cases were divided into three different surgical groups and followed up for a period of 5 years. The follow-up results were then discussed within each group.
Results
A total of 315 cases diagnosed with BC underwent regular follow-ups. The statistical analysis revealed an average age of 45 years and an average tumor size slightly over 2.2 cm, with early-stage BC (Stage I and II) accounting for 90.2% of the cases. The overall survival (OS) and disease-free survival times in the group undergoing total mastectomy with tissue preservation were comparable to those in the traditional radical mastectomy group and the breast-conserving plus radiotherapy group. Moreover, the complication rate, particularly the incidence of chest wall numbness and pulling sensations, was lower in the total mastectomy with tissue preservation group compared to the traditional radical mastectomy group. The overall average follow-up time was 64.4 months, with a recurrence and metastasis rate of 15.6% and an OS rate of 92.7%.
Conclusion
Based on our follow-up results, total mastectomy with more tissue preservation demonstrates comparable efficacy to breast-conserving surgery and traditional radical mastectomy. It can reduce some complications associated with traditional radical mastectomy and is beneficial for subsequent immediate and delayed breast reconstruction. This approach may be suitable for most patients with early to mid-stage breast cancer who do not wish to undergo breast-conserving surgery.
Introduction
Despite the rapid advancements in comprehensive breast cancer (BC) treatment, surgery remains the primary therapeutic approach. Radical mastectomy, introduced by Halsted 1 in 1894, has been a fundamental procedure in BC treatment. Modified surgical approaches, such as those introduced by Patey 2 in 1948 and Auchincloss 3 in 1963, aimed to improve patients’ quality of life by preserving the major pectoral muscle while removing the minor pectoral muscle. The NSABP-B04 study, 4 using the Halsted procedure as a control group, showed that the outcomes of the modified radical mastectomy were consistent with those of the radical mastectomy. In recent years, numerous studies5,6 have shown that early-stage BC patients can achieve comparable long-term survival outcomes with breast-conserving surgery plus local radiotherapy, offering the advantages of reduced surgical trauma and improved esthetic satisfaction. Breast-conserving surgery has become increasingly prevalent in clinical practice. However, due to concerns about malignancy, apprehension regarding radiotherapy, and individual preferences, many patients with early- or intermediate-stage BC still choose total mastectomy as their preferred initial treatment. The widely used radical mastectomy technique involves complete removal of the subcutaneous glandular tissue and a range of tissue, including the pectoralis major fascia, followed by suturing the incision to directly attach the skin to the surface of the pectoralis major muscle. This procedure can lead to complications such as local skin necrosis, significant numbness and pulling sensations, adhesion and atrophy of the pectoralis major muscle, and unsightly outcomes. Additionally, it poses challenges for delayed reconstruction. Preserving more subcutaneous tissue and pectoralis major fascia during surgery can reduce these complications and facilitate delayed reconstruction. However, further clinical data is needed to support the safety and reliability of this approach.
Data and Methods
General Data: This study enrolled cases of BC diagnosed and treated surgically at our hospital between May 2018 and July 2019. The inclusion criteria were as follows: (1) Female patients aged 18-70 years. (2) Pathologically confirmed invasive BC. (3) Clinical stages I, II, and IIIA. (4) Tumor size <5 cm. (5) Patients who underwent either total mastectomy or breast-conserving surgery. Exclusion criteria included: (1) Patients receiving neoadjuvant chemotherapy. (2) Patients undergoing palliative surgery. (3) Patients who underwent breast reconstruction or reshaping. (4) Pregnant or lactating patients. (5) Patients with concurrent malignancies. A total of 342 cases were included in the analysis. Postoperatively, comprehensive treatments such as chemotherapy, radiotherapy, targeted therapy, and endocrine therapy were administered based on the pathological findings and in accordance with the NCCN guidelines for BC diagnosis and treatment. Follow-up examinations were conducted every 3-6 months after disease onset. The follow-up period ended in December 2023, with 21 cases lost to follow-up (These patients have changed their place of residence and the hospital for follow-up examinations.) and 6 cases deceased due to unrelated causes (3 died in traffic accidents, 2 died from cerebrovascular accidents, and 1 died from ineffective treatment of acute abdomen), leaving a total of 315 valid datasets. Among these, there were 104 cases in the radical mastectomy group, 95 cases in the more subcutaneous tissue preservation group, and 116 cases in the breast-conserving surgery group. All the patients mentioned above were treated and followed up by the same group of surgeons. Surgical Methods:
2.1 Radical mastectomy, as illustrated in Figure 1, entails complete removal of the affected breast tissue, including the tumor, nipple, areola, and a portion of the skin along with the pectoralis major fascia. Approximately 0.5 cm of skin thickness is retained postoperatively. 2.2 The more tissue-preserving mastectomy, demonstrated in Figure 2, conserves 1-2 cm of skin and subcutaneous tissue based on the patient's subcutaneous fat thickness, while preserving the pectoralis major fascia. It involves the removal of the affected breast tissue, nipple, areola, and a portion of the skin. 2.3 Breast-conserving surgery involves excision of the tumor along with 1 cm of surrounding glandular tissue to ensure clear surgical margins. This procedure preserves the nipple, areola, and the remaining breast tissue. 2.4 All patients underwent sentinel lymph node biopsy (SLNB) in the ipsilateral axilla, and those with one or more positive sentinel lymph nodes (SLNs) underwent axillary lymph node dissection. The dissection extended to the L2 level of the axillary lymph nodes. Postoperative Treatment and Follow-up All patients underwent postoperative clinical staging and molecular classification based on paraffin pathology (Table 1) and received comprehensive treatment following the BC diagnosis and treatment guidelines. Hormone receptor-positive patients continued endocrine therapy for a duration of over 5 years, in addition to chemotherapy, depending on their clinical stage. HER2-positive patients received 1 year of targeted therapy with trastuzumab. Triple-negative breast cancer (TNBC) patients underwent regular follow-up after chemotherapy, based on their clinical stage. Patients who underwent breast-conserving surgery received postoperative radiotherapy. In the other two surgical groups, patients with three or more positive lymph nodes received postoperative radiotherapy, while the remaining patients did not undergo radiotherapy. The follow-up results are presented in Table 2. The reporting of this study conforms to STROBE guidelines.
7
Statistical analysis of the data was performed using SPSS 24. Count data are presented as cases, and intergroup comparisons were made using the Log-Rank χ2 test; measurement data with normal distribution are expressed as mean ± standard deviation. A P-value ≤ 0.05 was considered statistically significant. The disease-free survival (DFS) and overall survival (OS) rates among the three surgical groups were compared using the Kaplan-Meier method (Figure 3). Ethics and Informed Consent: This study has been approved by the Ethics Committee of the Second Affiliated Hospital of Fujian Medical University (Approval Number: 021,2018.03). All patients signed informed consent forms before treatment, agreeing that their treatment history and follow-up results may be used for clinical statistical research. The case images collected for this study have been obtained with the informed consent of the patients.
Results
Table 1 illustrates the fundamental characteristics of the enrolled patients, including postoperative pathological classification and clinical staging, among other relevant details. Among these, 64.8% of patients had negative axillary SLNs, with an average number of SLNBs exceeding three. Patients in stages I-II accounted for 90.2%. The demographic for the breast-conserving group predominantly included perimenopausal patients, with an age range of 25-50 years, an average age of 40 ± 5.7 years, and an average tumor size of 2.16 ± 0.82 cm. The traditional radical treatment group had the highest mean age, standing at 49 ± 6.3 years, with an average tumor size of 2.45 ± 1.1 cm. Both the axillary lymph node metastasis rates and the proportion of early-stage (I and II) patients were comparable across all three groups. Luminal A and B type patients underwent long-term endocrine therapy subsequent to surgery, whereas HER2-positive patients received a year of targeted therapy postoperatively. TNBC patients were subjected to routine follow-ups after receiving adjuvant chemotherapy as part of their treatment. All patients in the breast-conserving group received whole-breast radiotherapy postoperatively, and only those in the other two groups with three or more axillary lymph node metastases were administered chest wall and axillary radiotherapy. Following a BC diagnosis, all patients attended our hospital's outpatient clinic for follow-ups at intervals of every 3-6 months. The median follow-up duration was recorded as 64.4 months.
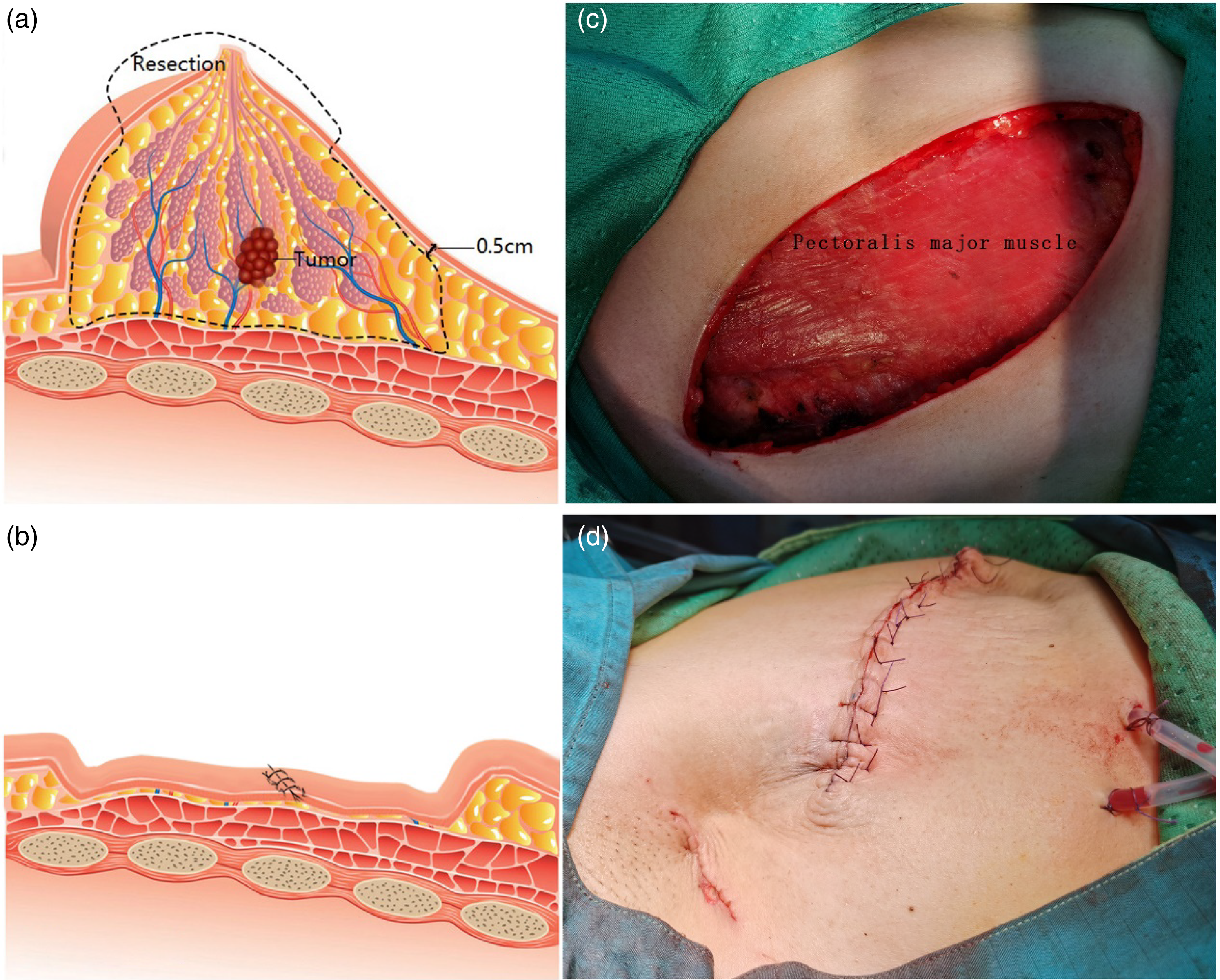
(a) The excision range for the traditional radical mastectomy in breast cancer treatment encompasses the surgical area which includes the removal of skin at least 2 cm beyond the tumor surface and the separation of the skin flap while preserving the subdermal vascular network, followed by the excision of the entire breast and the pectoralis major fascia. (b) Post-traditional radical mastectomy for breast cancer, the local wound is sutured, and the skin flap is directly opposed to the surface of the pectoralis major muscle. In patients with big Body Mass Index (BMI), a “Mediterranean-like” depression often persists superficially. (c) The wound surface after traditional radical mastectomy for breast cancer reveals a skin flap thickness of approximately 0.5 cm, and it is evident that the pectoralis major fascia has been removed. (d) The appearance following traditional radical mastectomy for breast cancer exhibits a noticeable local depression.

(a) The surgical procedure for breast removal with more tissue preservation involves the excision of skin at a distance of at least 2 cm from the tumor surface. The breast tissue is removed while maintaining a skin flap thickness of 1-2 cm, and the pectoralis major fascia is preserved. (b) Following breast removal with an emphasis on tissue preservation, the local wound is meticulously aligned, allowing the skin flap to be affixed to the surface of the pectoralis major muscle. Adequate tissue is retained beneath the wound surface to provide coverage. (c) After the breast removal with a focus on tissue conservation, the skin flap measures approximately 1-2 cm in thickness, and the integrity of the pectoralis major fascia is fully maintained. (d) The postoperative appearance after breast removal with a commitment to tissue preservation shows no evidence of local depression.

Survival proportion by three surgical group for disease-free survival (a) and overall survival (b).
Patients and Tumor Characteristics

TNBC, negative breast cancer; SLN, sentinel lymph node; SLNB, sentinel lymph node bio.
Complications and Prognosis
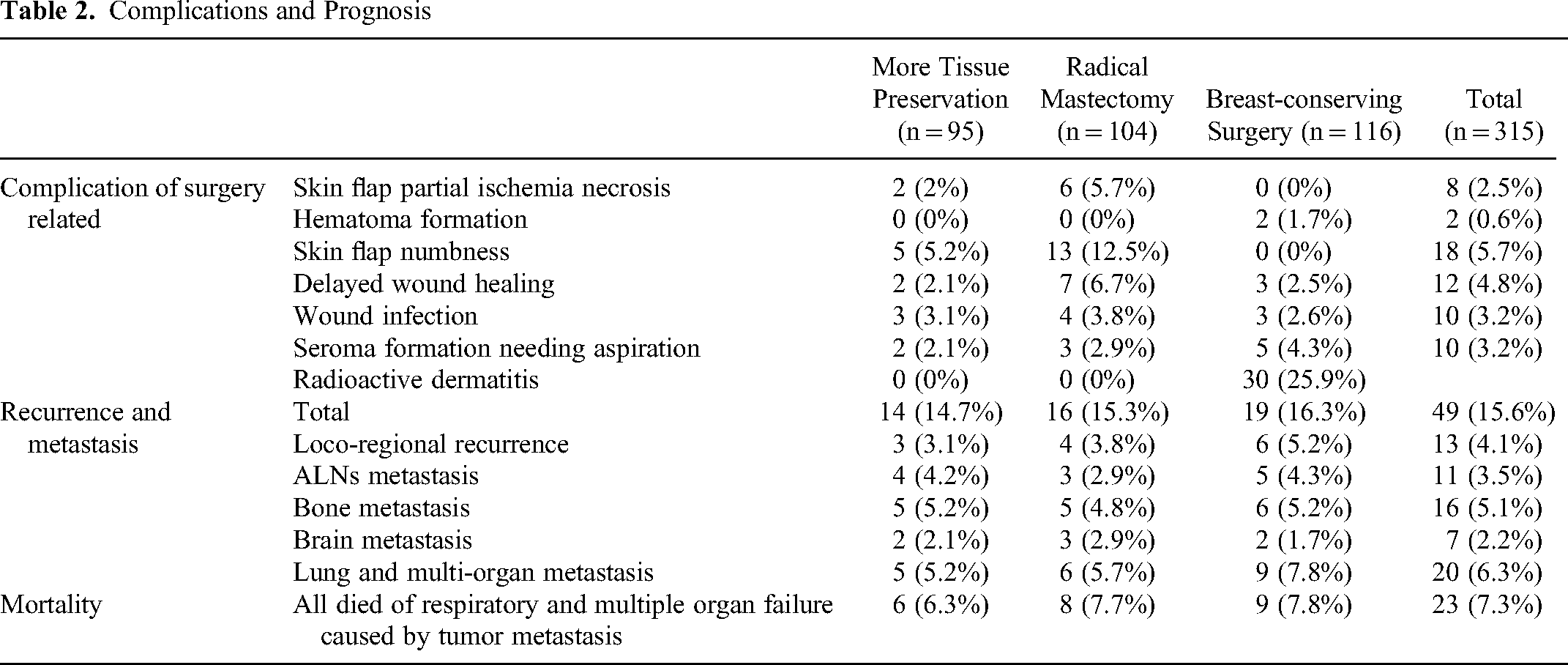
Table 2 delineates the postoperative complications and follow-up outcomes at 64.4 months. The traditional radical mastectomy group exhibited a higher prevalence of local skin flap ischemia and necrosis, as well as a greater incidence of postoperative chest wall numbness when compared to the other treatment groups. The breast-conserving cohort frequently experienced wound seroma; however, flap necrosis and chest wall numbness were infrequent. Conversely, there was a heightened rate of radiodermatitis due to radiotherapy, affecting 25.9% of patients. This manifested primarily as blistering, erythema, pruritus, and tightness of the chest wall skin. No instances of radiation pneumonitis were observed among those receiving radiotherapy; only imaging follow-ups implied minor pulmonary interstitial fibrosis. Within the follow-up duration, 49 patients encountered local recurrence and metastasis, culminating in an overall recurrence risk of 15.6%, with the peak period for recurrence occurring between 24 and 36 months. Of these cases, 10 patients with recurrence or metastasis were clinically staged at 3A, presenting a notably elevated recurrence risk in comparison to stages I-II (32.3%VS13.7%). There were 23 patient fatalities during the follow-up period, all attributable to tumor metastasis to organs such as the lungs and brain, resulting in respiratory and multi-organ failure.
A cohort of 315 BC patients was enrolled in the study, with a median follow-up period of 64.4 months. During this time, 23 patients succumbed to BC, and 49 patients experienced recurrence or metastasis. The 5-year OS rate was recorded at 92.7%, and the DFS rate stood at 84.4%. Within the cohort, 95 patients underwent breast-conserving surgery with an emphasis on tissue preservation, 104 patients received traditional radical mastectomies, and 116 patients were treated with breast-conserving surgery. The respective 5-year DFS rates for these groups were 85.3%, 84.6%, and 83.6% (χ2 = 0.113, P = 0.737 > 0.05), while the 5-year OS rates were 93.7%, 92.3%, and 92.2% (χ2 = 0.194, P = 0.659 > 0.05), respectively. No significant differences in DFS and OS were observed among the three treatment groups.
Discussion
BC, the most prevalent malignancy among women, has ascended to the highest rank in terms of incidence rate across all female-specific cancers. 8 The seminal concept proposed by Fisher et al 9 in the 1990s, which regards BC as a systemic disease, gained widespread acceptance. Over the past two decades, advancements in chemotherapy, targeted therapy, endocrine therapy, and radiotherapy have significantly improved the survival rates for BC patients. Since 1990, 10 mortality rates from BC have declined by two-thirds. An increasing number of studies11,12 suggest that breast-conserving surgery is associated with local recurrence rates, DFS rates, and OS rates that are comparable to, or even slightly better than, those of modified radical mastectomy. Consequently, breast-conserving surgery has emerged as a preferred surgical approach for BC. 6 Despite this, total mastectomy remains the treatment of choice in many regions, and a significant number of patients still opt for this procedure upon diagnosis. Due to concerns over recurrence, fear of death, limitations in healthcare provision, and economic considerations, the actual application of breast-conserving treatment in clinical practice is suboptimal. In 2019, the results of the CSBrS-005 study 13 indicated that the proportion of breast-conserving surgery for early-stage BC in China accounted for a mere 15%. Within our hospital, such procedures constitute only one-third of all operations for early-stage BC. As postoperative survival extends and quality of life improves, many patients who chose total mastectomy have come to regret their decision and are often troubled by the numbness on the chest wall after the removal of the breast. For many women, the loss of a breast can lead to a significant loss of confidence and may even precipitate anxiety and depression, profoundly impacting their lives. In response, numerous patients elect to undergo breast reconstruction to restore the shape of the breast and regain their self-assurance.
Clinically, the conventional radical mastectomy for BC involves the excision of the entire breast, including the axillary and pectoralis major fascia. The ACOSOG Z0011 clinical trial 14 established the efficacy of SLNB in evaluating axillary lymph node metastasis in BC patients. Additionally, other large-scale clinical trials15,16 have demonstrated that for patients with early-stage BC and a low-tumor burden in the SLN; SLNB alone is sufficient to control both local and distant recurrences. This approach has spared over 60% of patients from the trauma associated with axillary lymph node dissection, significantly reducing the incidence of postoperative lymphedema. Preserving more tissue is undeniably advantageous for patients. Pyfer et al 17 analyzed the early postoperative outcomes of 11 645 BC patients and found that the total complication rate, poor wound healing, infection, and bleeding were significantly lower in the breast-conserving group compared to those who underwent total mastectomy with implant reconstruction. Flanagan et al 18 retrospectively analyzed 3233 patients who underwent breast-conserving surgery or implant reconstruction for early-stage BC and found that satisfaction with the breast and quality of life scores were significantly higher in the breast-conserving surgery group than in those who had total mastectomy with implant reconstruction. Therefore, for patients who opt for total mastectomy over breast conservation, can preserving more subcutaneous tissue under the condition of ensuring a safe tumor margin (1-2 cm from the tumor) provide a therapeutic effect equivalent to traditional radical surgery? A retrospective analysis of nearly 5 years of follow-up results from 95 patients at our hospital revealed that preserving more subcutaneous tissue (1-2 cm from the skin) showed no difference in DFS and OS rates compared to the traditional radical excision group. Similarly, no differences were observed compared to the breast conservation plus radiotherapy group. However, in terms of postoperative complications and satisfaction with the local appearance, the group that preserved more subcutaneous tissue showed significant improvement over the traditional radical group. While ensuring therapeutic effects, preserving more subcutaneous tissue also reduces the difficulty and complications of subsequent breast reconstruction, alleviating the financial burden on patients.
In clinical practice, we meticulously craft treatment plans that are responsive to the unique circumstances of BC patients. For those who undergo breast-conserving surgery, adjuvant whole-breast radiotherapy directed at the affected side is an imperative component of treatment. Radiotherapy can instigate local skin inflammatory responses and occasion radiation pneumonitis, with the potential to escalate to local skin fibrosis and pulmonary interstitial fibrosis in severe instances. Iyer et al's 19 retrospective analysis revealed that 24% of the patient cohort treated with neoadjuvant concurrent chemoradiotherapy for locally advanced BC experienced grade 3 skin toxicity reactions. A prospective, multicenter SECRAB trial 20 evaluated the optimal sequencing of concurrent versus sequential chemoradiotherapy in early-stage invasive BC patients, disclosing that 24% of patients within the concurrent therapy arm suffered from moderate to severe acute skin reactions, as opposed to 15% in the sequential therapy group. Within our patient cohort, during total mastectomy procedures, we preserved a flap thickness ranging from 1 to 2 cm, contingent upon the patient's breast dimensions and subcutaneous fat layer. The surgical incision was strategically designed to excise the maximum amount of skin enveloping the tumor surface feasible, to ensure an ample tumor-free margin. Employing this technique for total mastectomy significantly curtailed the incidence of local flap necrosis and postoperative numbness and tautness of the skin on the ipsilateral side. Postoperatively, with the exception of patients presenting with more than three lymph node metastases who were administered chest wall radiotherapy, the remaining individuals abstained from radiotherapy. The outcomes indicated that the risk of local recurrence and distant metastasis did not augment in comparison to the other two groups. Consequently, these patients also circumvented the collateral risks associated with radiotherapy.
Summary of the significance of preserving more subcutaneous tissue: For patients with early-stage BC who are unwilling to undergo breast-conserving surgery, preserving more subcutaneous tissue can reduce postoperative complications such as local numbness, pulling sensation, and muscle atrophy. It also provides additional skin flap options for patients who choose delayed breast reconstruction in the later stage. For some patients with early-stage BC who choose subcutaneous gland excision and immediate breast reconstruction, preserving more subcutaneous tissue can result in fewer post-reconstruction complications and a more natural and full appearance of the breast. Through follow-up results of postoperative patients, data on safety and reliability can provide references for clinical physicians and patients in treatment decision-making.
In conclusion, we assert that in the contemporary era, characterized by increasingly sophisticated multidisciplinary approaches to BC treatment, surgeons should not be singularly focused on the exhaustiveness of radical surgery. Rather, judiciously preserving tissue in accordance with the patient's specific condition does not impinge upon the therapeutic efficacy for BC, while simultaneously providing enhanced protection and consideration for the patient's well-being.
Limitations of this study: 1. This study is an observational retrospective study, and patients voluntarily chose three different surgical options based on their condition (mainly referring to the clinical stage of the tumor) at the time of admission, rather than being a randomized, double-blind clinical study. The conclusions drawn may be more suitable for early-stage BC patients. 2. According to the American Cancer Society's research report 21 on BC survival, the 5-year survival rate is 91%, the 10-year survival rate is 84%, and the 15-year survival rate is 80%. The 5-year survival rates for the Local stage (invasive cancer confined to the breast) and Regional stage (cancer that has spread to surrounding tissue and/or lymph nodes) are 99% and 86%, respectively. In this study, the overall 5-year survival rate is 92.7%, with Regional stage cases accounting for approximately 35.2%. However, it is unclear whether there are differences in DFS and OS among the three groups of patients in longer follow-up periods (10 years, 15 years). 3. Due to limitations in sample size, this study did not group and discuss patients of different age groups, subtypes, and pathological stages, and therefore did not yield relevant observational results. 4. This study is a single-center clinical observational follow-up result, and more data from multiple centers and more cases are needed to support the reliability of this observational result.
Conclusion
Based on our follow-up results, total mastectomy with more tissue preservation demonstrates comparable efficacy to breast-conserving surgery and traditional radical mastectomy. It can reduce some complications associated with traditional radical mastectomy and is beneficial for subsequent immediate and delayed breast reconstruction. This approach may be suitable for most patients with early to mid-stage BC who do not wish to undergo breast-conserving surgery.
Footnotes
Acknowledgments
We would like to express our sincere thanks to all those who have lent us hands in the course of writing this paper.
Author Contributions
Study concept and design: Yinghui Liang. Acquisition of data: Yinghui Liang. Analysis and interpretation: Wenting Li. Study supervision: Yinghui Liang and Wenting Li.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study has been approved by the medical ethic commission of Second Affiliated Hospital of Fujian Medical University. (approval no. 021, 2018.03). All patients provided written informed consent prior to enrollment in the study.