
Abstract
BACKGROUND:
Immune-enhancing nutrition (IMN) strengthens the systematic inflammatory response and the immune system. Neutrophil to lymphocyte ratio (NLR) and absolute lymphocyte count (ALC) are affected during cancer therapies.
OBJECTIVE:
We carried out an analysis of the dynamic changes in NLR and ALC over time in cancer patients with or without IMN supplementation.
METHODS:
88 cancer patients receiving concurrent chemoradiotherapy (CCRT) were randomized into regular diet group, and regular diet and IMN group.Generalized estimation equation models were used to assess associations between patient’s characteristics, IMN, and dynamic changes in NLR and ALC over time.
RESULTS:
NLR and ALC at pre-CCRT were significantly associated with dynamic changes in NLR (adjusted
CONCLUSION:
Dynamic negative changes in both markers were demonstrated throughout CCRT. There were non-significant trend in promising changes in both NLR and ALC values in the whole group in IMN supplementation.
Keywords
Introduction
The majority of patients receiving concurrent chemoradiotherapy (CCRT) have poor nutritional statuses [1, 2, 3] associated with deteriorated lymphoid tissue and subsequent weakening of the immune function [4]. In addition to the disease factor, CCRT itself also induces inflammation and immunological suppression that may cause other treatment-related toxicities [1, 2, 3].
The sufficiency of energy and protein intake is an important nutritional management option for patients receiving CCRT [2, 3]. Nutritional supplementation improves several nutritional markers, such as albumin and prealbumin levels, lymphocyte count, etc. [5].
Immune-enhancing nutrition contains specific supplements that can moderate the inflammatory and immune responses [3, 6, 7]. Immune-enhancing nutritional supplementation is thought to strengthen the systematic inflammatory response and the immune system, which are known to be involved in the treatment response, progression, and prognosis in cancer patients [2, 3, 8, 9]. A study on immune-enhancing nutrition has shown that dietary arginine, glutamine, and omega-3 fatty acid supplementation in immunocompromised patients (including cancer patients) improved immunity and decreased inflammation markers [10].
Although the inflammation response and immunity can be measured via many laboratory tests, the most sophisticated ones are not widely available in real-life practice. Complete blood count (CBC), a routine laboratory test accessible to most hospitals, can be used to evaluate inflammation and immunity [11]. The neutrophil to lymphocyte ratio (NLR; the percentage of neutrophils divided by the percentage of lymphocytes from a CBC test) is an inflammation-based score that is used as a predictor for the prognosis and survival of cancer patients. An increase in NLR is associated with poor prognosis and lower survival of head and neck, esophageal, and cervical cancers [12, 13, 14, 15, 16], and unfavorable outcomes in various other cancers [17]. In addition, NLR is associated with the nutritional status: a higher NLR is found in patients who are malnourished compared with those with a normal nutritional status [18].
Lymphocytes have an essential function in the cancer-related immune response, and the absolute lymphocyte count (ALC; the number of lymphocytes circulating in peripheral blood) is a prognostic factor for clinical outcomes of cancer patients [19, 20, 21]. Lymphopenia, a condition in which lymphocytes decrease to less than the normal value, is considered as a sign of immunosuppression [22] and is an independent predictor of chemotherapy-associated toxicity as well as mortality [23, 24, 25, 26, 27, 28]. Both radiotherapy and chemotherapy can negatively impact lymphocyte count [29, 30, 31]. In addition, patients with low ALC have a worse response to therapy and shorter progression-free survival [32, 33, 34, 35].
In our previous study, nutrition counseling combined with immune-enhancing nutritional supplementation agents (arginine, glutamine, and fish oil) reduced the deterioration of nutritional status and also the severity of CCRT toxicity [8]. However, the relationship between immune-enhancing nutritional supplementation and practical inflammation and immunity markers NLR and ALC has rarely been studied in cancer patients undergoing CCRT. In this study, we carried out an analysis of the dynamic changes in NLR and ALC over time to evaluate the impact of immune-enhancing nutritional supplementation agents on cancer patients undergoing CCRT.
Median and interquartile range of the neutrophil to lymphocyte ratio and absolute lymphocyte count before and during CCRT
Median and interquartile range of the neutrophil to lymphocyte ratio and absolute lymphocyte count before and during CCRT
Abbreviations: ALC, absolute lymphocyte count; CCRT, concurrent chemoradiotherapy; IQR, interquartile range; NLR, neutrophil to lymphocyte ratio;
Patients
We obtained data from our prospective analysis of patients enrolled in a multicenter, randomized control study conducting between December 2013 and February 2015 among three cancer centers: Chiang Mai University Hospital, Prince Songklanagarind University Hospital, and Maharat Nakhonratchasima Hospital [9]. Eighty-eight cancer patients who received definitive CCRT, including 40 head and neck cancer patients, 28 esophageal cancer patients, and 20 cervical cancer patients were included in the study. Head and neck cancer patients received 60–70 Gy concurrent with weekly cisplatin 40 mg/m
Ethics approval and consent to participate
All subjects provided the institutional approved informed consents. This study was approved by each institutional ethics committee (i.e., Chiang Mai University Hospital, Prince Songklanagarind University Hospital and Maharaj Nakhonratchasima Hospital).
NLR and ALC measurements
NLR was calculated at each treatment visit (pre-CCRT, mid-CCRT, and end-CCRT) by dividing the percentage of neutrophils by the percentage of lymphocytes.
ALC was calculated as white blood cell count
NLR and ALC percent changes from pre-CCRT to mid-CCRT or end-CCRT: NLR or ALC %change
Statistical analysis
Patient characteristics at pre-CCRT were compared between the two groups (group A and group B) using the Chi-square or Fisher’s exact test for categorical variables and Mann-Whitney test for continuous variables. Median NLR and ALC were compared between the two groups (group A and group B) using the Mann-Whitney test. NLR and ALC between the three treatment visits (i.e., pre-CCRT, mid-CCRT, and end-CCRT) were compared using the Friedman test. Percent changes of NLR and ALC from pre-CCRT to mid-CCRT and end-CCRT were compared between the two groups (group A and group B) using the Mann-Whitney test. Univariable and multivariable generalized estimation equation (GEE) models were used to assess the association between dynamic changes of NLR and ALC over time and the following characteristics: gender, cancer site (i.e., head and neck, esophageal, or cervical cancer), age, body mass index (BMI) at pre-CCRT, and study group (group A and group B). Clinically relevant variables or covariates from univariable analyses with
Median and interquartile range of the neutrophil to lymphocyte ratio over time according to treatment visit for concurrent chemoradiotherapy. NLR, neutrophil to lymphocyte ratio; 
Patient characteristics at pre-CCRT, including age, gender, weight, height, body mass index, albumin, hemoglobin, tumor sites, tumor grade, tumor stage and Eastern Cooperative Oncology Group (ECOG) performance status were compared between groups A and B, as reported in Supplementary Table S1. There were no significant differences in characteristics at pre-CCRT between the two groups (
Table 1 reports the medians for NLR and ALC at pre-CCRT compared with mid-CCRT and end-CCRT for all patients and each cancer site. Overall, median NLRs at mid-CCRT and end-CCRT were higher than those at pre-CCRT (6.54 at mid-CCRT and 7.90 at end-CCRT compared to 2.26 at pre-CCRT;
As shown in Fig. 1, NLRs at pre-CCRT, mid-CCRT, and end-CCRT were not significantly different between groups A and B for all cancer sites, except that the median NLR value of esophageal cancer patients at pre-CCRT in group A was higher than in group B. However, the difference between the two groups was not statistically significant throughout the CCRT course (Fig. 1c). There were no statistically significant differences in the median ALCs between the two groups for overall patients, esophageal cancer patients, and cervical cancer patients (Fig. 2). For the head and neck cancer patients, ALC at end-CCRT was higher in group B compared with group A (
Percentage changes in the neutrophil to lymphocyte ratio and absolute lymphocyte count from pre-CCRT to mid-CCRT and end-CCRT (
88)
Percentage changes in the neutrophil to lymphocyte ratio and absolute lymphocyte count from pre-CCRT to mid-CCRT and end-CCRT (
Abbreviations: ALC, absolute lymphocyte count; CCRT, concurrent chemoradiotherapy; NLR, neutrophiltolymphocyte ratio;
Median and interquartile range of absolute lymphocyte count over time according to treatment visit of concurrent chemoradiotherapy. ALC, absolute lymphocyte count; 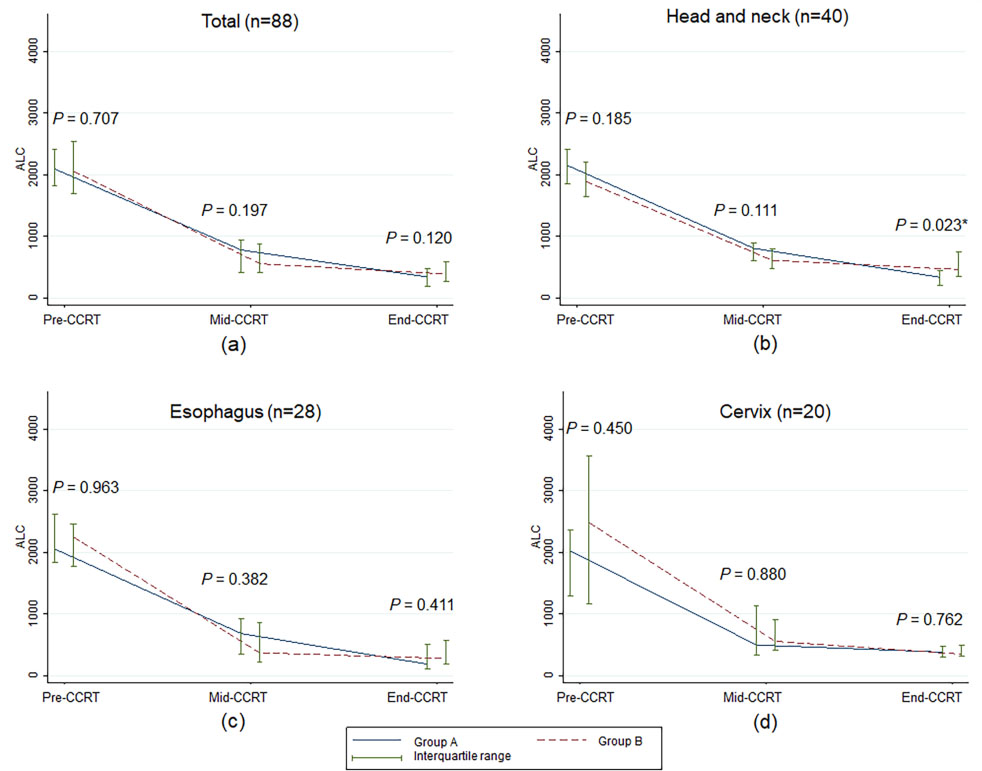
In Table 2, it can be seen that NLR increased throughout CCRT compared to pre-CCRT in both groups. The NLR value of patients in group B increased less, although the change was not statistically significant. ALC decreased during CCRT compared to pre-CCRT in the two groups; the decrease in patients in group B was less, although the change was not statistically significant.
A GEE model was used to identify factors associated with NLR and ALC changes over time in Table 3. At the multivariate level, NLR at pre-CCRT was independently associated with an increase in NLR over time. NLR during CCRT increased by 1.08 (95% confidence interval [95% CI]: 0.64–1.52) for each unit increase in pre-CCRT NLR in which a higher NLR level at pre-CCRT was significantly associated with a higher NLR after CCRT (
Factors associated with neutrophil to lymphocyte ratio change overtime using generalized estimation equation models
Abbreviations: 95% CI, 95% confidence interval;
Factors associated with absolute lymphocyte count change overtime using generalized estimation equation models
Abbreviations: 95% CI, 95% confidence interval;
After adjusting for the study groups, NLR at pre-CCRT, and cancer sites, we found that NLR at mid-CCRT increased 5.33 times compared to pre-CCRT, and NLR at end-CCRT increased 8.79 times compared to pre-CCRT (adjusted
Several markers are routinely used to evaluate nutrition status of patients. Serum albumin is one of nutrition parameters commonly used in clinical practice which may predict prognosis of patients. For example, hepatocellular carcinoma patients with low serum albumin level resulted in a worsening liver function and poor clinical outcomes [36]. In addition, white blood cells including neutrophils and lymphocytes are frequently measured in cancer patients, particularly during active anticancer treatment. In this study, we demonstrated the dynamic changes of practical prognostic factors for inflammation and immunity by using NLR and ALC calculated from CBC, which is a routine laboratory test. We also showed the effect of immune-enhancing nutritional supplementation on NLR and ALC during CCRT.
NLR significantly increased throughout the course of CCRT for all cancer types, which signifies increasing inflammation as an undesirable effect of both radiotherapy and chemotherapy treatment. Our finding is consistent with Sunpaweravong et al. [37], who evaluated the anti-inflammatory effect of immune-enhancing nutrition on esophageal cancer during CCRT by using C-reactive protein (CRP) and tumor necrosis factor-alpha (TNF-
Median ALC at pre-CCRT of all patients in the present study was 2,070 cells/
Based on the results of our study, radiotherapy and chemotherapy had a significant adverse effect on NLR and ALC during CCRT. Radiotherapy induces both apoptosis and non-apoptotic cell death to cancer cells. Apoptosis is a power-driven form of cell death that is either controlled or initiated in reaction to particular stimuli (e.g., cytokines) [41] or stimulated by cellular stress or injury [42]. Turrel et al. [43] summarized that the decline in ALC observed in cancer patients could be caused by a decreased production of lymphocytes. Chemoradiotherapy also significantly increases inflammation, and damage-associated molecular patterns are present after tissue damage from the radiation and activated pro-inflammatory immune system [44]. Elevated inflammatory cytokines also have been reported in cancer treated with radiotherapy and chemotherapy [45, 46]. In our multivariate analysis, pre-CCRT NLR and pre-CCRT ALC were associated with NLR and ALC values during CCRT, respectively. Moreover, the time point during CCRT was associated with both NLR and ALC levels. Thus, we should keep NLR at pre-CCRT as low as possible and ALC at pre-CCRT before CCRT as high as possible.
Apart from the inflammation marker, NLR is used as a prognostic factor in cancers. Higher pretreatment NLR is correlated with worse OS in oropharyngeal cancer treated and worse disease-free survival and OS in esophageal cancer with radiotherapy [47, 48, 49]. High post-RT NLR is associated with poor OS and PFS in nasopharyngeal cancer and higher recurrent rate in breast cancer [39, 50]. Similarly, ALC is used as prognosis factor and nutritional status assessment. Low post-RT ALC links to the deteriorated OS in oropharyngeal cancer [51]. ALC is also used as a part of the formulae to evaluate nutritional status which also associates with prognosis in cancer patient. Serum albumin and ALC are used to calculate prognostic nutritional index (PNI). The same lab tests with an additional ratio of current weight and ideal body weight are used for Geriatric Nutritional Risk Index (GNRI). Caputo et al. [52] demonstrated that low PNI (
Another study using different and more novel inflammatory markers (CRP and TNF-
Immune-enhancing nutrition may be one of key facet in cancer management. Other novel treatment might also be beneficial. Metronomic approach may be associated with improved nutritional status in patients with head and neck cancer [55] as well as patients with hepatocellular carcinoma [56].
This study has some limitations, the first being the diversity of cancer sites, as mentioned previously, since the values of NLR and ALC vary in the different primary cancers [57, 58]. A focused study on each particular cancer site might reveal more detail on the dynamic changes of these values. The second potential limitation is that we did not measure other more novel inflammation markers such as CRP, interleukin-6 (IL-6), and TNF-
Our results indicate that the pre-CCRT NLR and ALC values were affected by CCRT, thereby confirming the results of Machon et al. [38] that immune-enhancing nutritional supplementation before CCRT can lower these inflammation markers. A future study to confirm that immune-enhanced nutritional supplementation improves these pre-CCRT inflammation and immunity marker is being planned as a prospective trial.
The recovery of NLR and ALC after CCRT also a potential subject for further investigation. Since we did not measure ALC and NLR during follow-up after CCRT and immune-enhancing nutritional supplementation was stopped immediately at the end of CCRT, the effect of the supplementation in this period cannot be evaluated. This is one of the limitations of our study and it would be interesting to investigate whether allowing continual immune-enhancing nutritional supplementation would enable recovery from treatment-related lymphopenia caused by CCRT since it takes some time for the normal cells to recover from the effects of both treatment modalities.
Conclusions
Dynamic detrimental changes in NLR and ALC levels were demonstrated throughout CCRT. Pre-CCRT values of both markers were significant predictors for a favorable change. There were noticeable promising changes in both NLR and ALC values in patients receiving immune-enhancing nutritional supplementation, although the differences were not statistically significant. The effect of immune-enhancing nutritional supplementation on pre-CCRT NLR and ALC should be evaluated in a future randomized study.
Author contributions
Conception: Imjai Chitapanarux and Nontiya Homkham
Interpretation or analysis of data: Imjai Chitapanarux and Nontiya Homkham
Preparation of the manuscript: Imjai Chitapanarux, Nontiya Homkham, Pooriwat Muangwong, Veeradej Pisprasert, Patrinee Traisathit, Rungarun Jiratrachu and Pattawee Chottaweesak
Revision for important intellectual content: Imjai Chitapanarux, Nontiya Homkham, Pooriwat Muangwong, Veeradej Pisprasert and Patrinee Traisathit
Supervision: Imjai Chitapanarux
Supplementary data
The supplementary files are available to download from
sj-docx-1-cbm-10.3233_CBM-210086.docx - Supplemental material
Supplemental material, sj-docx-1-cbm-10.3233_CBM-210086.docx
Footnotes
Acknowledgments
We acknowledge Northern Thai Research Group of Radiation Oncology (NTRG-RO), Faculty of Medicine and Chiang Mai University for supporting the current study. The nutritional supplementation and blenderized diet in this study was supported by Thai Otsuka Pharmaceutical Company, Bangkok, Thailand [grant number: CNN-ISS-2013].