
Abstract
BACKGROUND:
The Controlling Nutritional Status (CONUT) score, a novel immuno-nutritional index, was reported as a predictor of overall survival (OS) in some tumors.
OBJECTIVE:
We aimed to investigate the association between baseline CONUT Score and clinical outcomes in patients with multiple myeloma (MM).
METHODS:
We performed a retrospective analysis of 245 patients with MM. The CONUT score was determined prior to therapy.
RESULTS:
Among the entire cohort, the complete remission rate was markedly higher in the low-CONUT (
CONCLUSIONS:
The CONUT score was a predictor of OS in MM patients especially in cases with both low ISS staging and CONUT score. The baseline CONUT score may be an early and practical indicator of the efficacy of anti-myeloma treatment.
Introduction
Multiple myeloma (MM) is a malignant disorder of plasma cells that mainly occurs in elderly patients, being diagnosed at a median age 70 years [1]. With the rapid evolution of very active new therapies for MM in recent decades, the survival of affected patients has significantly improved [2]. However, there are patients who experience disease progression and relapse.
The prognosis of patients with MM is highly variable according to different tumor characteristics, the microenvironment and host factors. Several prognostic indices such as the International Staging System (ISS) and revised ISS (R-ISS) have been established and have stratified prognosis of patients with MM [3, 4]. Nevertheless, the current prognostic staging systems do not take into account the role of the patient’s immune-nutritional status in MM treatment.
Malnutrition is known to be associated with worse clinical outcomes and the severity of chemotherapy-related toxicity in cancer patients [5, 6]. The Controlling Nutritional Status (CONUT) score is now used as an immuno-nutritional index to detect undernourished patients in the hospitalized population [7]. The score is based on the values of serum albumin, total cholesterol (TC) and lymphocyte count. It has been reported to associate with poor survival in patients with solid tumors and hematological malignancies [8, 9, 10, 11, 12]. Recently, two studies from Japan have reported that CONUT score is a useful prognostic indicator in patients with MM [13, 14]. This needs to be confirmed in other patient cohorts. Furthermore, the impact of the CONUT score on the response to treatment in MM patients is very limited. Therefore, we performed a retrospective study to investigate the association between baseline CONUT score and clinical outcomes of patients with MM.
Patients and methods
Patients
We performed a single-center retrospective analysis of 376 consecutive patients with symptomatic MM who were diagnosed between January 1, 2007 and December 31, 2017. Patients who refused or abandoned any treatment (
Clinical and laboratory information
All clinical data regarding patients recruited were obtained from medical charts, electronic records and telephone interviews by the trained staff members. Data were collected with the following items: age, gender, M protein type, ISS stage, white blood cell count, hemoglobin, lymphocyte count, TC, World Health Organization (WHO) performance status, lactate dehydrogenase (LDH), albumin, and creatinine at diagnosis, and information concerning treatment and response. The CONUT scores, used to assess immuno-nutritional status, were calculated from the serum albumin concentration, total peripheral lymphocyte count, and TC concentration, as previously described [7]. Treatment for each patient was determined by the physician, the patient, or their family. Treatment responses were evaluated according to IMWG criteria [15].
Statistical analyses
All analyses were performed using SPSS statistical software (version 19.0; IBM Corp., Armonk, NY, USA).
Patients characteristics of patients between three CONUT score groups
Patients characteristics of patients between three CONUT score groups
Ig, Immunoglobulin; ISS, International Staging System; WBC, White blood cell count; T-Chol, Total cholesterol; LDH, lactate dehydrogenase; NUL, normal upper limit; CONUT score, Controlling Nutritional score; WHO, World Health Organization.
Patient characteristics
A total of 245 patients with newly diagnosed MM were included in the analysis. The median age of patients in this study was 65 (range, 33–83) years. There were more men (
The baseline characteristics of the patients stratified according to the CONUT score are presented in Table 1. High CONUT scores were associated with lower white blood cell count, lower lymphocyte, lower hemoglobin level, lower albumin level, lower TC level, and elevated LDH. Patients in the highest CONUT score group were older (
Response and CONUT score
Most patients received bortezomib (
Treatment response in patients with different baseline CONUT score (
The median OS of the entire cohort was estimated as 48 months (95% CI: 41.2–54.8). We analyzed the impact of CONUT score on the survival of patients. The 3-year OS estimates for the low-CONUT group, mid-CONUT group and high-CONUT group were 81.7%, 59.8%, and 33.5%, respectively. The 5-year OS estimates of the three groups were 65.1%, 38.9% and 16.6%, respectively. The CONUT score is an important prognosis factor for MM, and patients with CONUT score
Overall survival according to the CONUT score at diagnosis. CONUT, controlling nutritional status.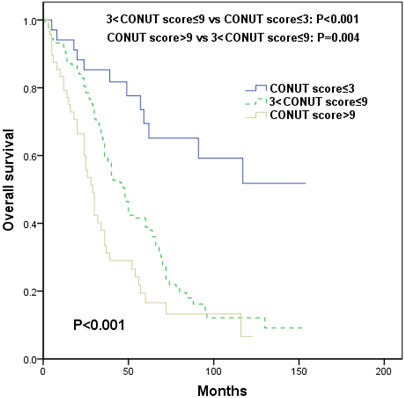
Among the whole cohort, the ISS stage was stage I in 2 patients, stage II in 111 patients, and stage III in 132 patients. Although the patients with an ISS
We then examined the effect of the CONUT score on OS in the different ISS stages patients. CONUT score was assessed separately for ISS stages II and III, as shown in Fig. 3. We did not analyze the OS for the ISS I stage due to the few cases (only two). The median OS of patients with CONUT score
We further analyzed whether the CONUT score could improve the prognostic impact of ISS stages. We stratified the patients according to combining ISS stage and CONUT score into four different groups. The ISS-CONUT very low-risk group was defined as ISS
Univariate and multivariate analysis of factors associated with overall survival
Univariate and multivariate analysis of factors associated with overall survival
Abbreviations: ISS, international staging system; WHO, World Health Organization; LDH, lactate dehydrogenase; NUL, normal upper limit; CONUT, controlling nutritional status; OS, overall survival; OR, odds ratio; CI, confidence interval.
Analysis of survival in patients with multiple myeloma. (a) OS according to the ISS. (b–c) OS by ISS stages II and III with the CONUT score 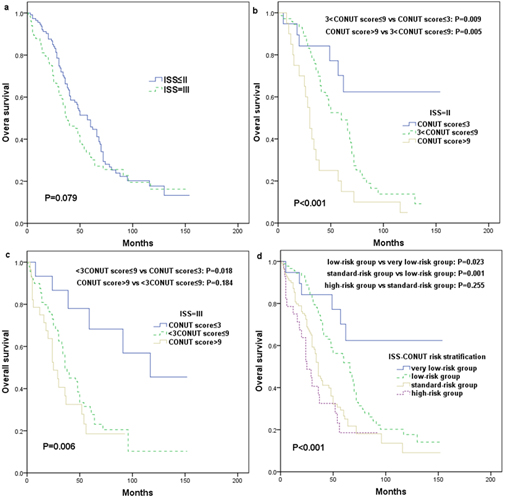
Results of the univariate and multivariate analyses for factors influencing OS in newly diagnosed patients with MM were reported in Table 2. In univariate analysis, older age (
Discussion
In recent years, the CONUT score as a simple, objective and inexpensively measured parameter of immuno-nutritional status has attracted attention. By studying the characteristics of 245 real-world patients, we found that the OS rate of the low-CONUT group was significantly higher than that of the mid-CONUT group or high-CONUT group, and the CONUT score was an independent prognosis in newly diagnosed MM patients, which is in agreement with previous investigations [13, 14].
Okamoto et al. [13] retrospectively analyzed the CONUT score in 64 Japanese patients with symptomatic MM. In this study, the median age at diagnosis was 66 years, and the CONUT score
Recent reports showed that the prevalence of malnutrition and its risk among cancer patients were positively associated with the disease stages, about 60% of advanced cancer patients were malnourished [17, 18]. In the present study, 55.9% patients had CONUT scores
Poor status of nutrition is associated with the response to chemotherapy and the development of side effects and toxicity of therapy-related, which also are factors associated with the rise of healthcare costs for managing cancer patients [17, 18, 20]. Therefore, early nutritional status screening and assessment may be important to provide comprehensive algorithms for individualized clinical treatment in cancer patients. In our study, the CR rate of initial therapy was markedly higher in the low-CONUT group compared to the mid-CONUT group or high-CONUT group, suggesting that the baseline CONUT score could become an early and practical indicator of the efficacy of anti-myeloma treatment.
The OS rate of our patients tended to be relatively shorter than those previous reports [21, 22, 23]. Our cohort had a very lower transplantation rate and short course novel agents use [24], which likely better reflected the variation in the systems of care provision, financing and clinical practice patterns for MM patients in the real-world setting. Interestingly, the ISS was unable to identify any clear value in the outcomes for OS in our series. This was possibly due to small number and uneven distribution of the patients. In contrast, the addition of CONUT score to the ISS further defined prognosis particularly in stage II and III patients. We thus combined the ISS stage and CONUT score to propose an algorithm, which could possibly improve the predictive value of the ISS staging system and assist in individualized treatment.
Our study had some limitations. First, it was a collection of retrospective data from a single center with possible selection bias. Second, we did not evaluate any treatment differences. Third, the data of fluorescence in situ hybridization (FISH) or cytogenetics were lacking in our cohort. In addition, the CONUT score did not have a standardized cut off, and the cut-off values of CONUT score as a prognostic marker for cancer patients were varied with reports.
In conclusion, the CONUT score was a useful predictor of OS and treatment response in MM patients. The CONUT score could be combined with ISS staging system to identify patients with survival outcome. Further investigations focused on this subject are warranted.
Footnotes
Acknowledgments
The authors thank all of the doctors and nursing staff of Department of Hematology in Wuxi people’s Hospital for their dedicated patient care.
Conflict of interest
The authors declare no conflict of interest.
Author contributions
Conception: Hongfeng Guo.
Interpretation or analysis of data: Xin Zhou, Yan Lu, Jun Xia, Jingjue Mao, Jing Wang.
Preparation of the manuscript: Hongfeng Guo, Xin Zhou, Yan Lu.
Revision for important intelectual content: Hongfeng Guo, Xin Zhou, Yan Lu.
Supervision: Hongfeng Guo.