
Abstract
BACKGROUND:
Increasing evidence have shown that miRNAs play an important role in the development and progression of non-small cell lung cancer (NSCLC).
OBJECTIVE:
In this study, we aimed to analyze serum exosomal miR-216b expression in NSCLC patients and its potential clinical significance.
METHODS:
A total of 105 NSCLC patients and 60 healthy controls were enrolled, and quantitative reverse transcription polymerase chain reaction (qRT-PCR) was performed to detect serum exosomal miR-216b expression.
RESULTS:
The results demonstrated that serum exosomal miR-216b levels were significantly lower in NSCLC patients compared to controls. In addition, receiver operating characteristic analysis revealed that serum exosomal miR-216b had better diagnostic accuracy than CEA, CYFRA21-1 or SCCA. Moreover, serum exosomal miR-216b levels in early-stage NSCLC patients were dramatically increased after surgical resection, and patients with low serum exosomal miR-216b expression had higher lymph node metastasis probability. Furthermore, low serum exosomal miR-216b expression was closely associated with poor prognosis. Finally, multivariate analysis showed that serum exosomal miR-216b could serve as an independent predictor of NSCLC.
CONCLUSIONS:
Collectively, serum exosomal miR-216b might be used as a potential diagnostic and prognostic biomarker for NSCLC.
Introduction
Lung cancer is one of the most frequent types of human cancer and the leading cause of cancer death all around the world [1]. Lung cancer can be divided into small cell lung carcinoma and non-small cell lung carcinoma (NSCLC), and NSCLC accounts for approximately 80–85% of all lung cancers [2, 3]. The main treatment approach for this malignancy is surgical resection which is not suitable for patients having advanced or metastatic disease [4]. Unfortunately, most of NSCLC patients are diagnosed at the advanced or metastatic stage, leading to unfavorable prognosis with a poor 5-year survival rate [5, 6]. Therefore, more efforts should be made to discover effective and reliable tumor markers for NSCLC diagnosis and predicting its prognosis.
MicroRNAs (miRNAs) are a class of small non-coding RNAs and bind to the 3’ untranslated region of target messenger RNA (mRNA), resulting in either modulation of translation efficiency or degradation of the mRNA [7]. MiRNAs play an important role in diverse biological processes, such as proliferation, growth, metastasis, apoptosis, and differentiation [8]. Exosomes are small membrane-enclosed extracellular vesicles (30–100 nm) and contain proteins, RNAs, DNAs and lipids [9]. Emerging evidence has shown that miRNAs in the exosome are in an unexpectedly stable form compared to those which are not contained in exosomes [10]. Up to date, some circulating exosomal miRNAs were found to be abnormally expressed in NSCLC, and acted as either oncogenes or tumor suppressors. For instance, serum exosomal miR-17-5p expression was significantly higher in NSCLC patients, indicating that miR-17-5p could be used in NSCLC diagnosis [11]. Low serum exosomal miR-146a-5p expression was found in NSCLC patients and correlated with shorter survival, suggesting that serum exosomal miR-146a-5p might act as a prognostic prediction biomarker [12].
MiR-216b had been reported to function as a tumor suppressor gene in many cancer types, including NSCLC [13, 14, 15]. However, the clinical significance of serum exosomal miR-216b in NSCLC had not yet been explored. In this study, serum exosomal miR-216b levels in NSCLC patients were evaluated, and then the associations between serum exosomal miR-216b expression and clinical data of NSCLC cases were further analyzed.
Materials and methods
Ethics statement
The current study had been approved by the Ethical Committee of Guangxi Medical University. Written informed consent was obtained from all participants. All samples were handled and made anonymous according to the ethical and legal standards.
Patients and serum samples
In this study, a total of 105 patients with NSCLC and 60 healthy volunteers were enrolled. None of the patients had received any radiation therapy or chemotherapy prior to the surgery. Tumor stages were determined by tumor-node-metastasis (TNM) staging system according to the 2002 International Union against Cancer guidelines. Among all NSCLC cases, 54 cases were at stage I/II, whereas 51 patients were at stage III/IV. The clinical variables of the NSCLC subjects were presented in Table 1. Sixty healthy volunteers who were on a regular visit to our hospital were recruited for routine physical examination. The controls were matched to the NSCLC cases by age and sex. These healthy subjects had no history of cancer as well as unremarkable blood test, liver/kidney function, and chest X-ray examination. The NSCLC and healthy control samples were collected and processed in an identical manner. Peripheral venous blood samples were obtained prior to any treatment and withdrawn from NSCLC subjects and healthy controls. Blood samples were centrifuged at 3,000 g for 10 minutes, and the supernatant was collected and stored at
Clinical variables of 105 NSCLC patients and serum exosomal miR-216b expression
Clinical variables of 105 NSCLC patients and serum exosomal miR-216b expression
Exosomes were isolated from serum samples using the ExoQuick Exosome Precipitation Solution (SBI, Mountain View, CA, USA) according to the manufacturer’s instructions. Briefly, the serum was thawed on ice and centrifuged at 3,000 g for 15 min to remove possible cell debris. Then, the supernatant was mixed with one-fourth volume of ExoQuick solution and were incubated at 4
Exosomal RNA isolation and quantitative reverse transcription PCR
Total exosomal RNA was isolated from serum with the mirVana PARIS kit (Life Technologies, New York, USA) according to the manufacturer’s protocols. RNA quantity and quality were determined by an Agilent 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA) according to the manufacture’s instruction. During the RNA isolation, 2
Tumor biomarkers detection
Carcinoembryonic antigen (CEA), cytokeratin 19 fragment 21-1 (CYFRA21-1), and squamous cellcarcinoma-related antigen (SCCA) were widely used as tumor biomarkers for NSCLC. Electrochemiluminescent immunoassay (ECLIA; Hoffman-La Roche Ltd., Basel, Switzerland) was used to detect CEA and CYFRA21-1 expression levels. Chemiluminescent microparticle immunoassay (CMIA, ARCHITECT SCC assay; Abbott Laboratories, Abbott Park, IL, USA) was used to detect SCCA expression levels.
Statistical analysis
All statistical analyses were performed using GraphPad Prism 8.0.2 (GraphPad Software, Inc., La Jolla, CA, USA) and MedCalc 12.1.4.0 (MedCalc, Mariakerke, Belgium). Mann-Whitney U-test was used to compare serum exosomal miR-216b expression level between different groups. Chi-square test was carried out to evaluate the association between serum exosomal miR-216b expression and clinical variables. Receiver operating characteristic (ROC) curves were constructed and the area under the ROC curve (AUC) were used to assess the discriminatory power of serum exosomal miR-216b and each individual tumor biomarker (CEA, CYFRA21-1 and SCCA). Similarly, ROC analysis was performed to estimate the diagnostic accuracy of the combined signature which included serum exosomal miR-216b, CEA, CYFRA21-1 and SCCA. Overall survival (OS) time was calculated from the date of diagnosis to death or last follow-up. Disease-free survival (DFS) time was calculated from the date of diagnosis until the first evidence of relapse or last follow-up. Kaplan-Meier method was performed to plot the OS and DFS curves. Multivariate Cox proportional hazards regression models were used to estimate the hazard ratios (HR) for OS and DFS.
Results
Decreased expression of serum exosomal miR-216b in NSCLC
QRT-PCR was carried out to measure serum exosomal miR-216b levels in 105 NSCLC patients and 60 healthy controls. As shown in Fig. 1, serum exosomal miR-216b expression levels in NSCLC patients were significantly lower than those in controls (
Serum exosomal miR-216b levels were lower in NSCLC patients compared to controls.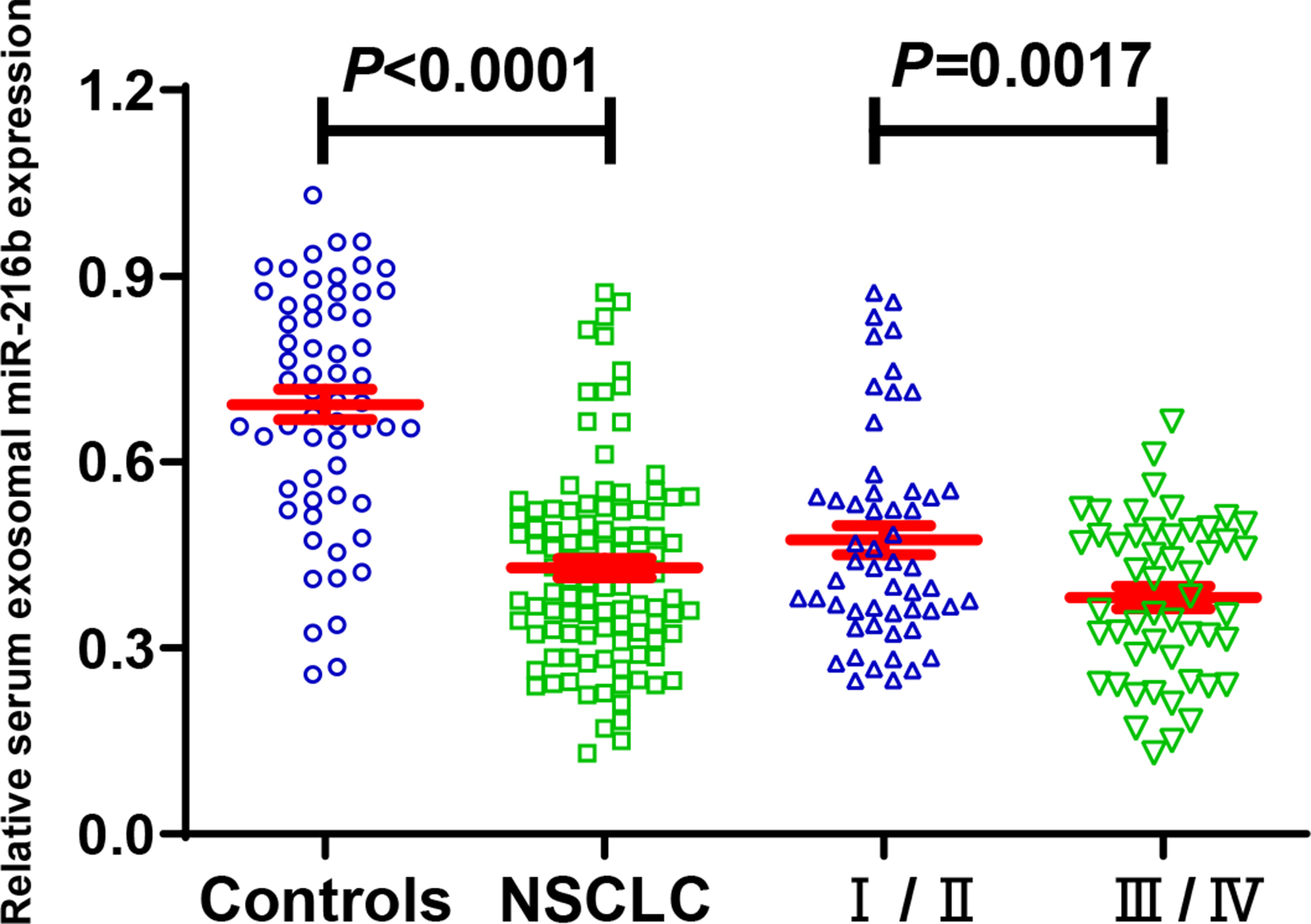
ROC analysis was performed to assess the diagnostic accuracy of serum exosomal miR-216b, CEA, CYFRA21-1 and SCCA. Figure 2A showed serum exosomal miR-216b could well differentiate NSCLC patients from normal controls with an AUC of 0.840, the sensitivity and the specificity were 86.7% and 75.0%, respectively. CEA had a sensitivity of 83.8% and a specificity of 74.0% for identifying NSCLC cases from controls with an AUC of 0.808 (Fig. 2B). The AUC of CYFRA21-1 diagnosis of NSCLC was 0.813, with a sensitivity of 81.0% and a specificity of 73.3% (Fig. 2C). The AUC for SCCA was 0.698, the sensitivity and specificity was 71.4% and 68.3%, respectively (Fig. 2D). Serum exosomal miR-216b showed better performance than other three tumor makers. In addition, the combination of serum exosomal miR-216b and the tumor makers (CEA, CYFRA21-1 and SCCA) produced an increased AUC of 0.925 and achieved higher specificity of 88.3%, higher sensitivity of 89.5% (Fig. 2E).
(a) ROC curve for serum exosomal miR-216b in 105 NSCLC patients and 60 controls. (b) ROC curve for CEA in 105 NSCLC patients and 60 controls. (c) ROC curve for Cyfra21-1 in 105 NSCLC patients and 60 controls. (d) ROC curve for SCCA in 105 NSCLC patients and 60 controls. (e) ROC curve for combination of serum exosomal miR-216b and tumor markers in 105 NSCLC patients and 60 controls.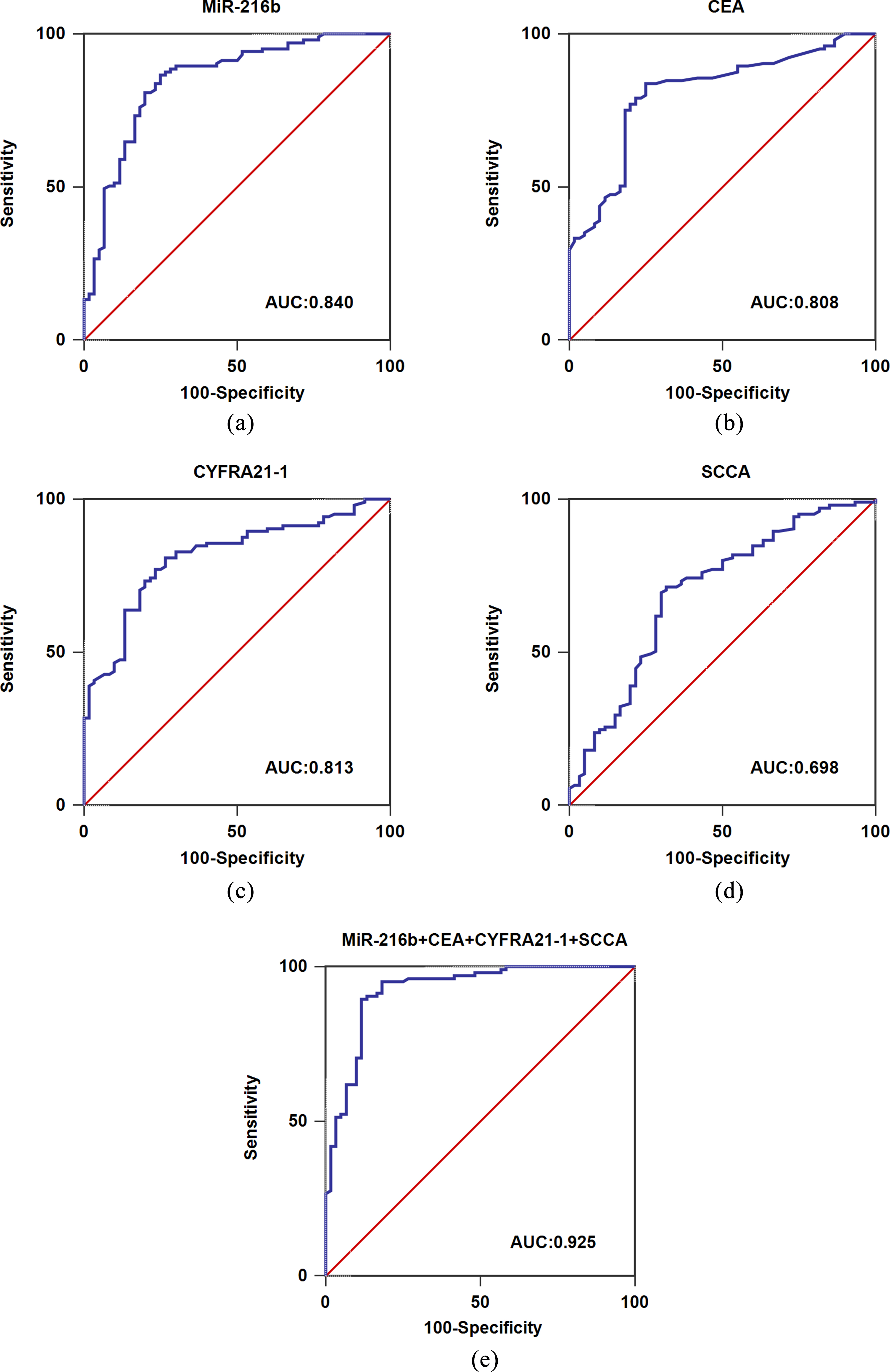
The optimal cut-off value (Youden index) for dividing the NSCLC cohort into high and low serum exosomal miR-216b expression group was determined based on the ROC curve which discriminated the NSCLC patients from healthy controls. All 105 NSCLC patients were classified into high serum exosomal miR-216b expression group (
Serum exosomal miR-216b levels in early stage NSCLC patients after surgery
Then, blood samples from 54 early-stage NSCLC subjects (I/II) were collected two weeks after their surgical resection. Compared to the pre-treatment samples, serum exosomal miR-216b levels were significantly increased (
Multivariate analyses of variables for overall survival and disease-free survival in NSCLC patients
Multivariate analyses of variables for overall survival and disease-free survival in NSCLC patients
(a) Comparison of serum exosomal miR-216b expression before and after surgery in 54 early stage NSCLC patients. (b) Serum exosomal miR-216b was of potential prognosis value for lymph node metastasis after surgery.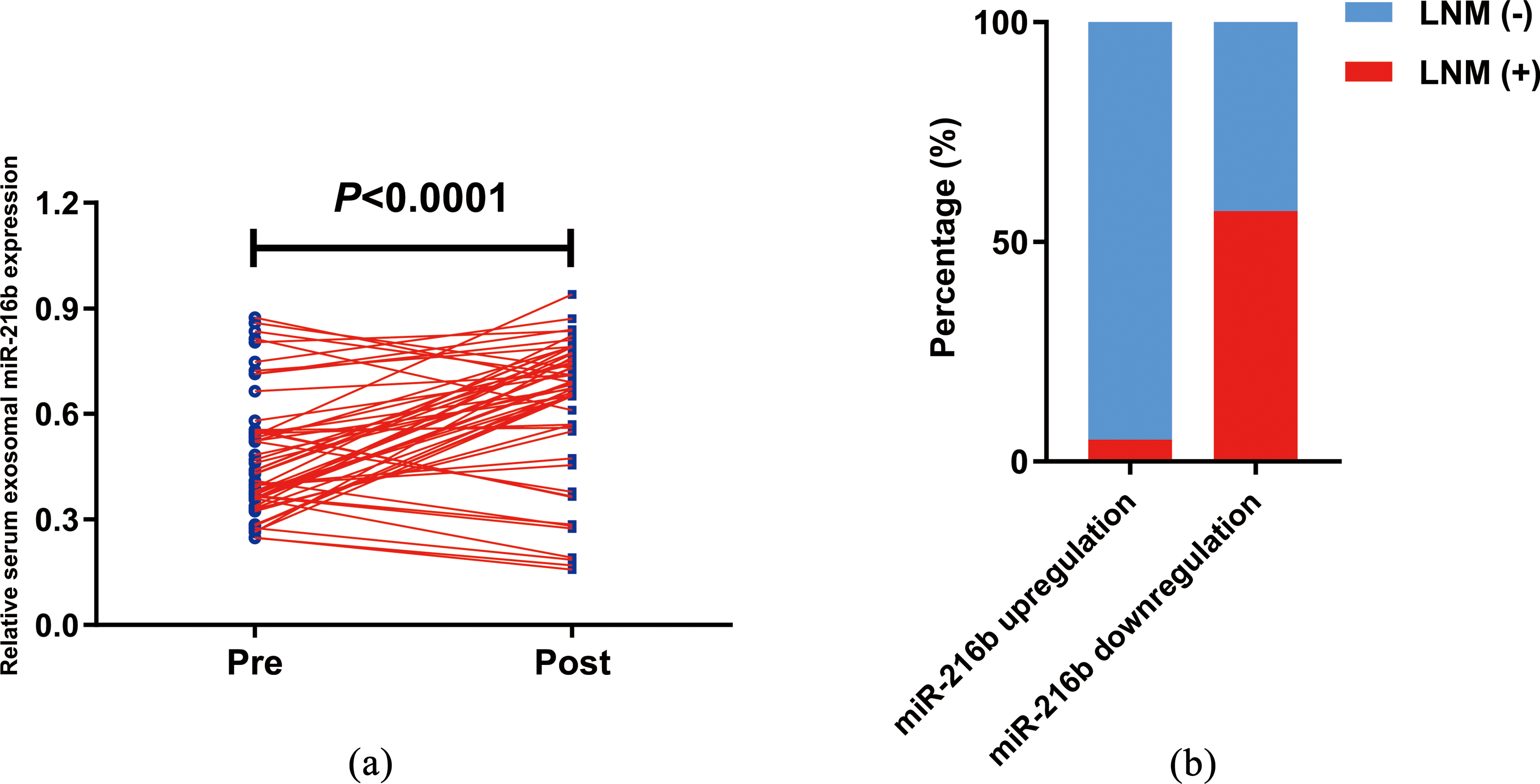
Kaplan-Meier survival revealed that low serum exosomal miR-216b expression was closely associated with a shorter OS (
(a) Low serum exosomal miR-216b expression was associated with shorter OS. (b) Low serum exosomal miR-216b expression was associated with shorter DFS.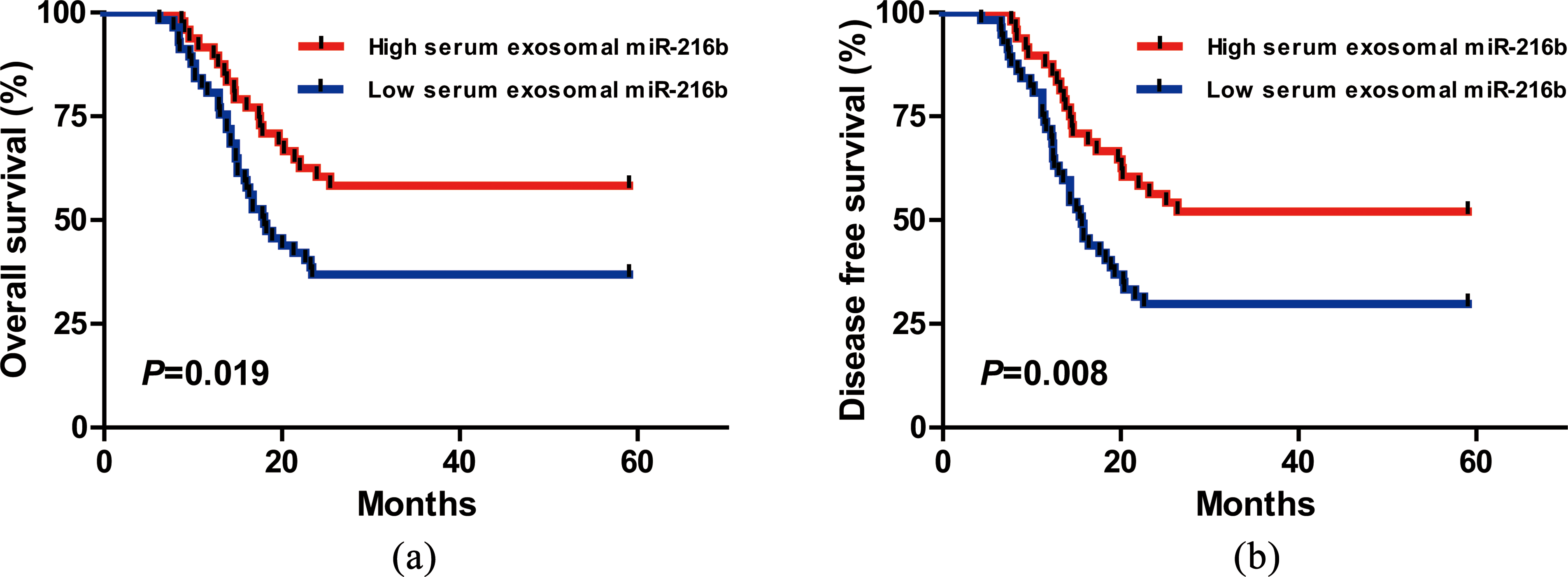
To date, identification of novel and reliable blood-based biomarkers for the diagnosis, prevention and treatment of NSCLC are urgently required. To the best of our knowledge, this was the first study to analyze the clinical value of serum exosomal miR-216b in NSCLC. The results of our study showed serum exosomal miR-216b expression levels in NSCLC cases were significantly higher than those in controls. In addition, ROC analysis showed serum exosomal miR-216b could well differentiate NSCLC patients from healthy control, and the combination of serum exosomal miR-216b and the tumor makers (CEA, CYFRA21-1 and SCCA) showed better diagnostic power than each marker alone. Moreover, serum exosomal miR-216b levels in early-stage NSCLC patients were dramatically increased after surgical resection, and lymph node metastasis probability in miR-216b downregulation group was much higher than in miR-216b upregulation group. Furthermore, serum exosomal miR-216b downregulation was closely associated with worse clinical parameters and shorter survival. Finally, serum exosomal miR-216b was confirmed to be an independent predictor of OS/DFS of NSCLC patients. Our findings were in line with previous studies [13, 14, 15], and demonstrated that miR-216b functioned as a tumor suppressor in NSCLC.
Some previous studies have reported that miR-216b was abnormally expressed in this malignancy. For instance, Wang et al. found that miR-216b expression was markedly downregulated in NSCLC tissues and cells, ectopic expression of miR-216b inhibited cancer cell proliferation, invasion and migration through regulating FOXM1 [13]. Likewise, miR-216b downregulation was found both in NSCLC tissue and cell lines, miR-216b overexpression significantly suppressed the carcinogenesis by silencing SOX9 expression [14]. MiR-216b upregulation significantly stimulated cisplatin-dependent mitochondrial apoptosis and dramatically enhanced the ability of cisplatin to promote NSCLC cell apoptosis [15]. Thus, miR-216b downregulation might contribute to the development and progression of NSCLC.
The tumor suppressive role of miR-216b had been studied in many cancer types besides NSCLC. For example, decreased miR-216b expression was observed in hepatocellular carcinoma patients and closely associated with aggressive clinical variables, miR-216b overexpression exhibited a significant tumor-suppressive effect on cancer cell growth and migration [16, 17]. Jana et al. revealed that miR-216b upregulation greatly attenuated cell proliferation, migration and invasion in breast cancer by directly targeting SDCBP, and vice versa [18]. In glioma, miR-216b expression was remarkably decreased in cancerous tissues and cell lines, enforced miR-216b expression significantly repressed cancer cell growth and invasion in vitro and inhibited the carcinogenesis in vivo. Both FoxM1 and AEG-1 were its downstream target genes [19, 20]. In addition, He et al. showed miR-216b was significantly underexpressed both in cervical cancer cells and tissues, and its downregulation was negatively correlated with clinical outcomes. MiR-216b upregulation or FOXM1 inhibition dramatically suppressed tumorigenicity of cervical cancer [21]. In nasopharyngeal carcinoma (NPC), miR-216b expression was markedly decreased in NPC cell lines and tissue samples, overexpression of miR-216b inhibited NPC cell viability in vitro and tumor growth in vivo mice experiment [22]. In clear cell renal cell carcinoma, miR-216b upregulation not only significantly reduced cancer cell proliferation and invasion, but also inhibited tumor growth in vivo [23]. MiR-216b expression was significantly lower in pancreatic cancer tissues than in adjacent normal tissues, and miR-216b upregulation or KRAS knockdown suppressed cell viability and increased cell apoptosis [24]. Moreover, miR-216b expression was significantly reduced in both tissues and cell lines of pancreatic ductal adenocarcinoma (PDAC), and in vitro evidence showed that miR-216b overexpression greatly restrained cell growth, migration and invasion by directly targeting ROCK1 [25]. Sun et al. demonstrated that enforced miR-216b expression resulted in decreased proliferation, migration in melanoma cells both in vitro and in vivo, and FOXM1 overexpression significantly reversed the anti-tumor activities of miR-216b [26]. In colorectal cancer (CRC), miR-216b expression was significantly reduced both in CRC tissues and cell lines, and miR-216b downregulation was highly associated with worse clinical variables as well as shorter survival. Upregulated miR-216b expression markedly suppressed CRC cell proliferation, invasion, migration and angiogenesis through HMGB1-mediated JAK2/STAT3 pathway [27] or SRPK1 [28].
Conclusions
Taken together, our data provided convincing evidence that serum exosomal miR-216b downregulation was associated with unfavorable prognosis in NSCLC, and it might serve as a reliable non-invasive biomarker for NSCLC diagnosis and prognosis.
Footnotes
Acknowledgments
This study was supported by the Key Research and Development Program of Guangxi (Guangxi Science No: AB18221080).