
Abstract
OBJECTIVE:
This study aimed to assess the diagnostic value of human epididymis protein 4 (HE4) in the pleural effusion of lung cancer patients.
METHODS:
HE4 protein in the pleural effusion of 60 lung cancer patients was measured by electrochemiluminescence, in parallel with those from 56 patients with benign lung disease, and the association with malignant pleural effusion was evaluated.
RESULTS:
The level of HE4 in samples from lung cancer patients was significantly higher than the level for those with benign lung lesions (
CONCLUSION:
HE4 in the pleural fluid of lung cancer patients can be valuable in the diagnosis of malignant pleural effusion; however, it does not correlate with the prognosis of patients.
Introduction
Lung cancer has had the highest incidence and mortality of all malignancies in the world for the past few decades [1]. In China alone, 73,000 new cases are estimated to be diagnosed annually, accounting for one-third of the worldwide total [2]. Malignant pleural effusion (MPE) is a common symptom of advanced stages of cancer [3]. It is most commonly observed in lung cancer, with about one-third of the patients developing MPE [4]. At present, the most reliable approach to diagnose MPE is pathological tissue cytometry, but the positive rate is very limited [5]. Traditional tumor markers, such as carcinoembryonic antigen (CEA), carbohydrate antigen 125 (CA125), carbohydrate antigen 19-9 (CA19-9), and cell keratin 19 fragment (CYFRA21-1) are also used in the diagnosis of MPE, with a high specificity but a low sensitivity. Thus, these tumor markers are often used together to improve sensitivity [5]. A number of new tumor markers for the diagnosis of MPE have been identified in recent years, such as a high level of vascular endothelial growth factor (VEGF), which mediates MPE generation by increasing vascular permeability; however, the diagnostic efficacy needs to be improved [4].
Clinicopathological characteristics of the patients (
denotes the number of patients)
Clinicopathological characteristics of the patients (
Human epididymis protein 4 (HE4) is encoded by the gene WFDC2, which is located in the long arm of chromosome 6. It is a member of the protease inhibitor family and is usually expressed in the epithelia of normal reproductive and respiratory tracts. HE4 is frequently upregulated in gastric [6], endometrial [7], and peritoneal cancer [8] and in other malignancies. Of clinical importance, a high serum level of HE4 is an ideal marker for the early screening and differential diagnosis of epithelial ovarian cancer [9] as well as an independent prognostic marker for ovarian cancer patients [10].
HE4 is highly expressed in lung cancer [11], particularly in adenocarcinoma, which shows a significantly higher level of HE4 than other histopathological types. HE4 expression is often associated with a poor prognosis [12]. Thus, a high level of HE4 in the serum of patients has been used as a marker for the early diagnosis of lung cancer [13]. Importantly, increased HE4 in the serum also differentiates lung cancer from tuberculosis and pneumonia [14]. In addition, a high serum level of HE4 in patients with non-small cell lung cancer (NSCLC) correlates with tumor node metastasis staging of the tumor and a poorer 5-year survival than that for patients with low serum HE4. Therefore, the serum level of HE4 has been used as an independent prognostic marker for NSCLC patients [15]. In patients with advanced NSCLC, a higher serum level of HE4 is associated with a poorer response to chemotherapy and a poorer outcome, compared to patients with a lower HE4 level [16]. Similarly, using the HE4 level in the serum increases the sensitivity and specificity of the diagnosis of small cell lung cancer (SCLC), and improves the diagnostic efficiency when used in combination with other tumor indexes [17]. So far, research on the relationship between HE4 and lung cancer has been mainly focused on serology, and little is understood about the clinical significance of HE4 in pleural effusion. Therefore, in this study, HE4 in the pleural effusion of lung cancer patients was measured and its value in the diagnosis of MPE was determined.
Patient recruitment
This study was approved by the Institute Research Ethics Committee of the Cancer Center of Nanjing Medical University, Jiangsu, China. Informed consent was obtained from individual participants before their pleural effusion samples were used.
From October 2015 to May 2017, 116 patients with pleural effusion, including 60 malignant and 56 benign cases, were recruited from the Affiliated Jiangning Hospital of Nanjing Medical University, China. Malignancy was confirmed by pleural effusion shedding cytology, fiberoptic bronchoscopy pathological biopsy, percutaneous lung puncture cytology, and other approaches, and patients with pleural effusion caused by other malignancies were excluded. The 56 benign cases were confirmed by pathology, cytology, or pathogenic microbiological examination.
Sample collection and analysis
Pleural effusion samples were collected prior to cancer treatment by conventional aseptic puncture, and 15 mL of each sample was centrifuged at 2,000
Statistical analysis
Data were processed using the Statistical Package for the Social Sciences (Version 23.0), and presented as mean
The level of HE4 in the pleural effusion of lung cancer patients was significantly higher than that in pleural effusion originating from tuberculosis and inflammation (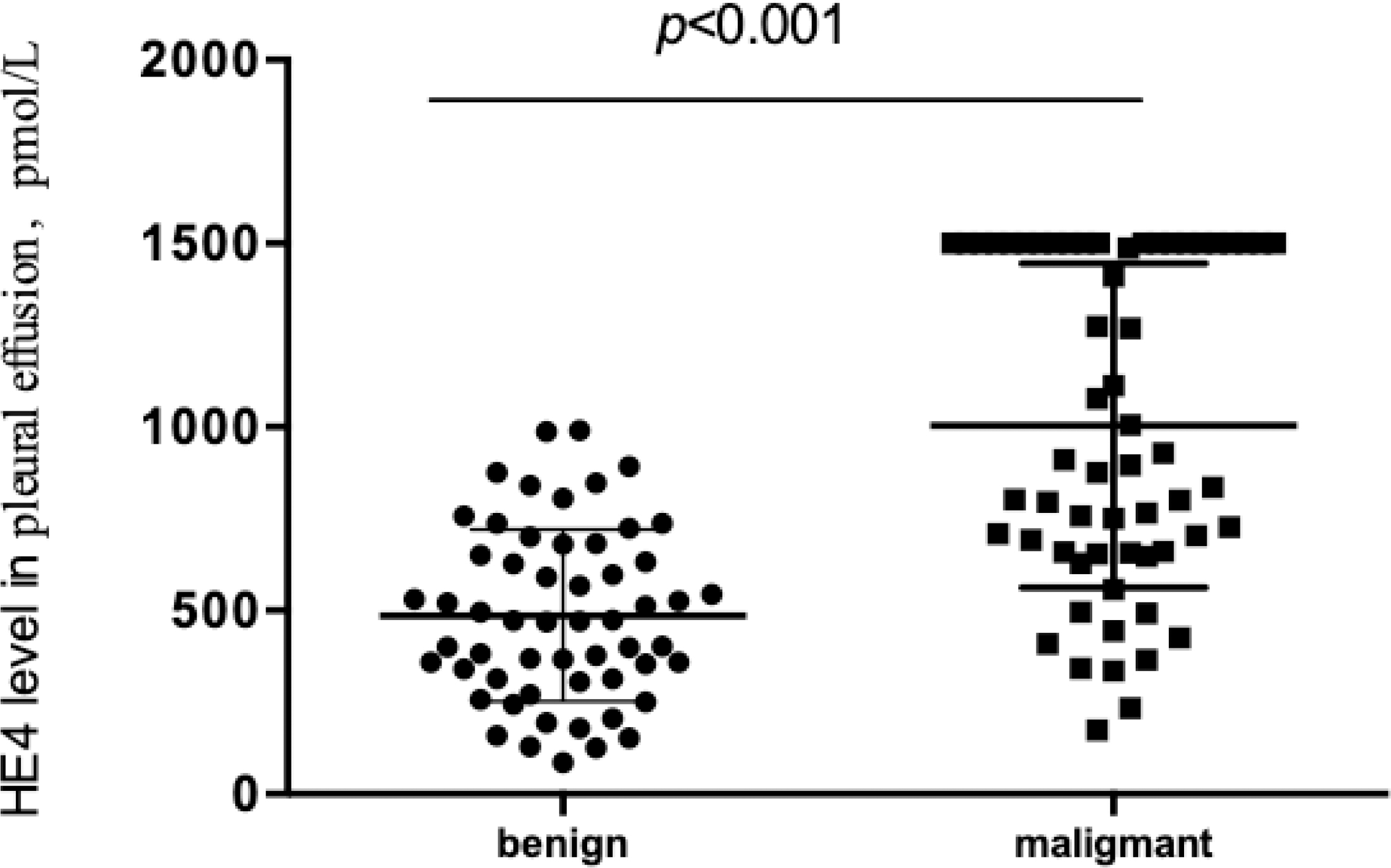
Clinicopathological features of the patients
Sixty lung cancer patients with MPE were recruited for this study, together with 56 patients with benign pleural effusion caused by tuberculosis and inflammation. The clinicopathological characteristics of all patients are summarized in Table 1. The 60 lung cancer patients comprised 43 men and 17 women aged between 27 and 91 years with an average age of 66.71
Baseline characteristics of patients with malignant and benign pleural effusion
Baseline characteristics of patients with malignant and benign pleural effusion
Patients with lung adenocarcinoma showed significantly higher levels of HE4 in pleural effusion than those with squamous cell carcinoma (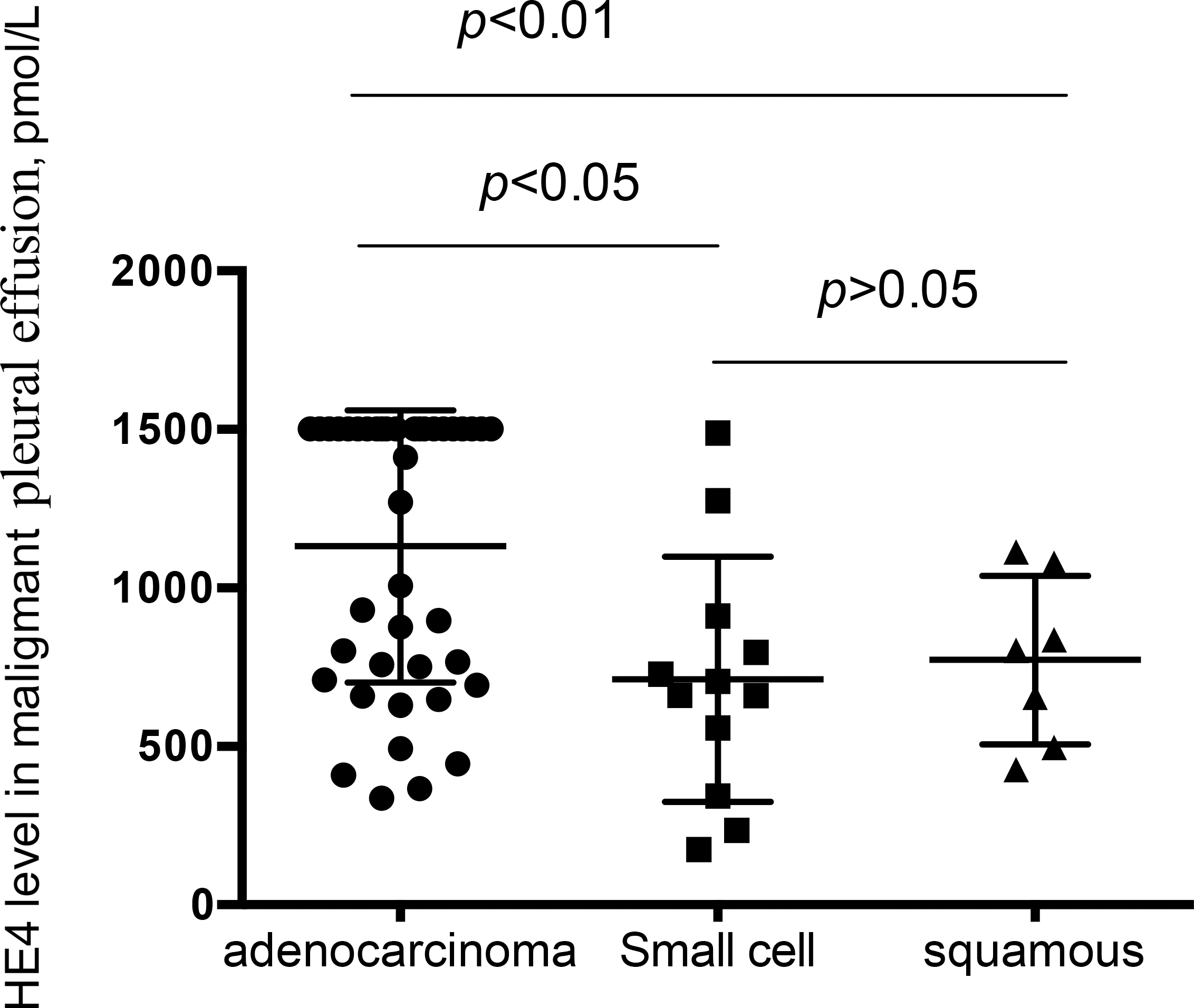
Correlation of serum HE4 level with the clinicopathological characteristics of the patients
There was no significant difference in HE4 level in pleural effusion resulting from tuberculosis and inflammation (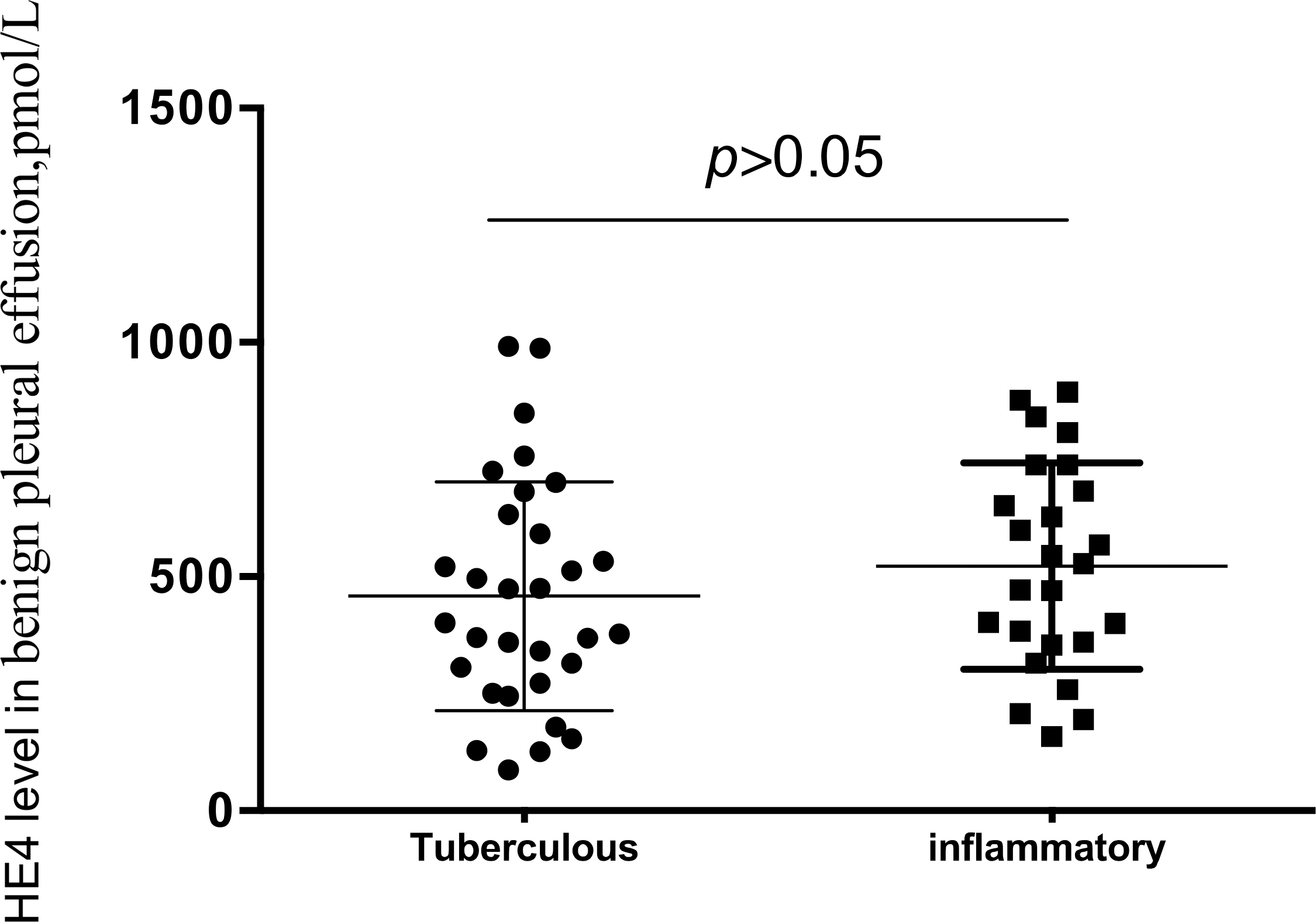
Electrochemiluminescence analysis revealed an average of 1004.56
HE4 level in MPE was unrelated to the sex and age of the patients (
HE4 level (
) in patients with benign lung lesions and clinicopathological parameters
HE4 level (
ROC curve of HE4 to predict malignant pleural effusion.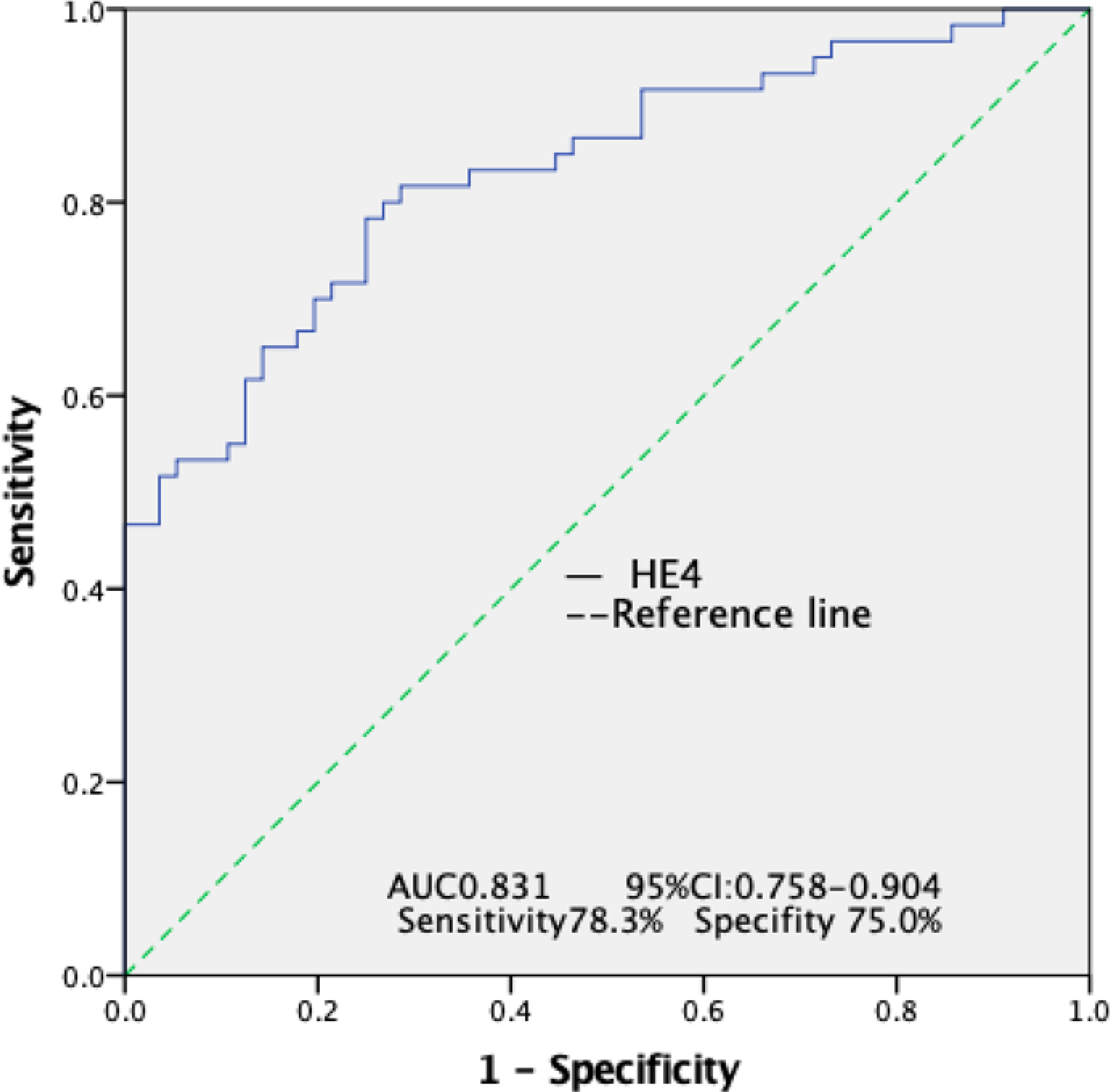
To evaluate the diagnostic efficiency of the HE4 concentration for MPE, a receiver operating characteristic (ROC) curve was plotted and is shown in Fig. 4. The area under the curve (AUC) for the HE4 level was 0.831 and the confidence interval (CI) was 0.758–0.904. When the HE4 level was 652.2 pmol/L, the sensitivity was 78.3% and the specificity was 75%. Considering CEA and CA125 are two commonly used biomarkers for lung cancer, we also examined the levels of CEA and CA125 in pleural effusion in parallel with that of HE4 to assess their association and compare their diagnostic efficiencies. As shown in Table 3, the concentration of HE4 was associated with that of CEA but not CA125. The sensitivities of CEA and CA125 for MPE were 70.0% and 81.67%, respectively, comparable to that of HE4.
ROC curve of HE4 to predict lung adenocarcinoma.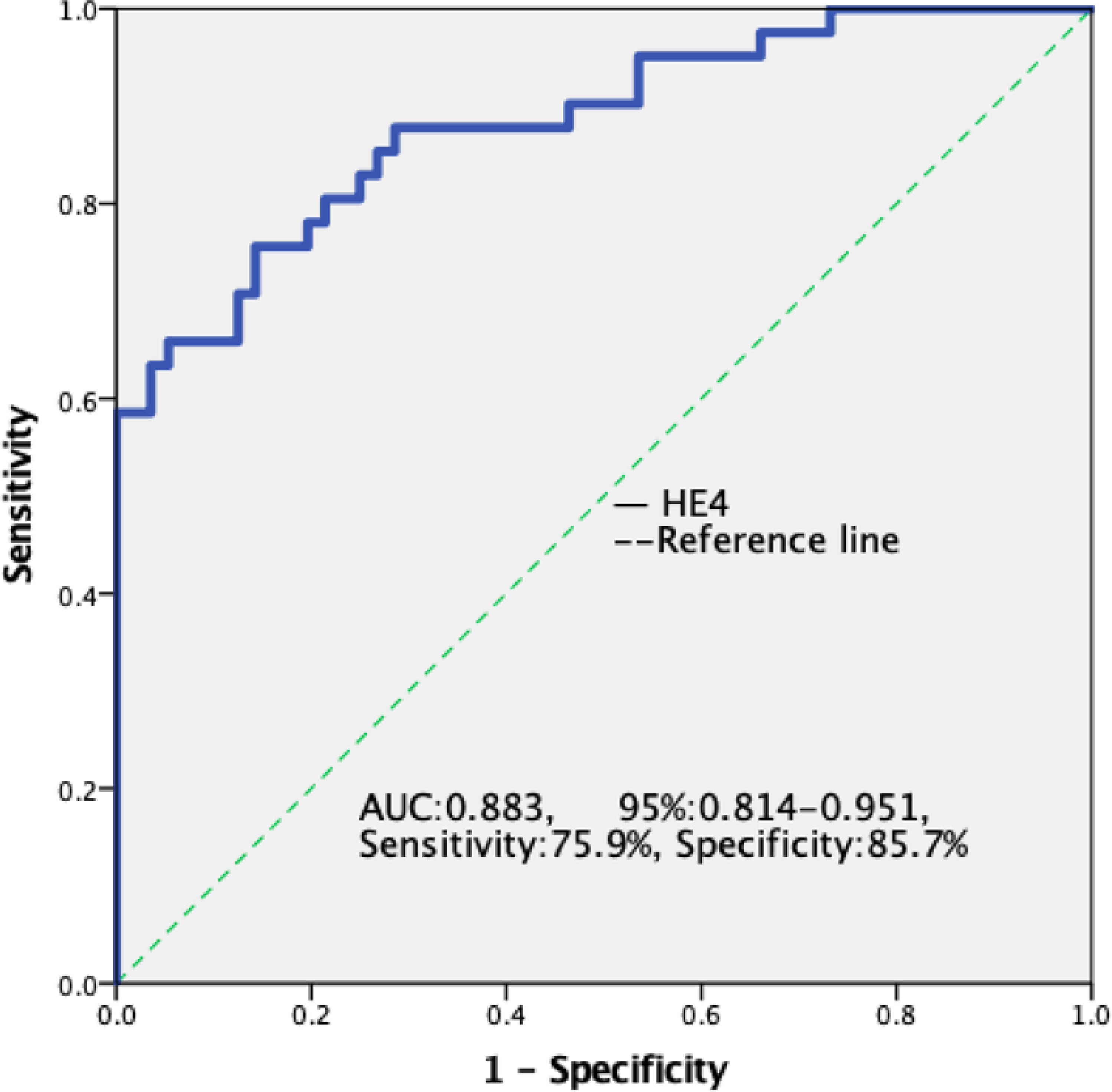
Kaplan-Meier analysis of the accumulative survival of lung cancer patients with high and low levels of HE4 in pleural effusion, 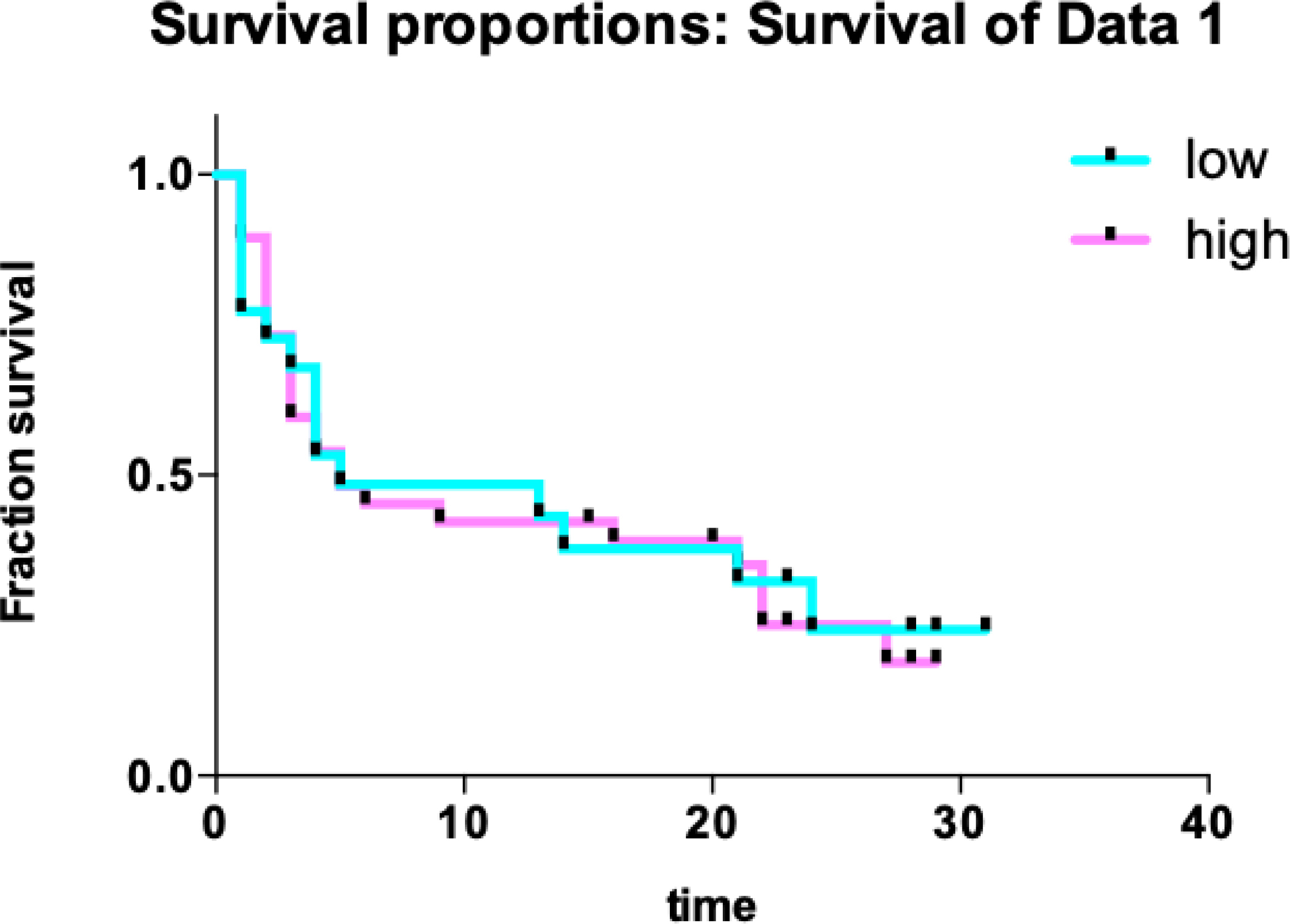
To further evaluate the value of HE4 in the diagnosis of lung adenocarcinoma, the ROC for lung adenocarcinoma against benign pleural effusion was plotted (Fig. 5), and the AUC value was found to be 0.883. When the HE4 level was 744.05 pmol/L, the sensitivity was 75.9 % and the specificity was 85.7%. To assess the correlation of the HE4 level with the prognosis, lung cancer patients were classified into two subgroups using the HE4 value of 652.2 pmol/L at the maximum Youden index as a threshold and the survival rates of the groups were compared (Fig. 6). The survival periods for the patients with low and high HE4 were 13.33
Discussion
It remains challenging to diagnose MPE and common biomarkers are still elusive. This necessitates further efforts toward the identification of markers or marker panels that can improve the sensitivity and specificity of the diagnosis of MPE. In this study, the level of HE4 in pleural effusion resulting from lung cancer was analyzed in comparison with those from tuberculosis and inflammation. The association of the HE4 level with the malignancy of the pleural effusion and the histopathological features of lung cancer was assessed to evaluate the potential of this protein in the diagnosis of lung cancer.
Our results demonstrated a significant increase of HE4 in MPE, differentiating it from pleural effusion resulting from tuberculosis and inflammation. This is mirrored by its elevation in the serum of lung cancer patientss [18, 19]. The results suggest that the HE4 level in pleural effusion can be used as a biochemical marker to identify patients with MPE. Plotting the ROC curve for malignant against benign pleural effusion demonstrated an AUC value of 0.831. When an HE4 level of 652.2 pmol/L was used, the sensitivity and specificity were 78.3% and 75%, respectively. Noticeably, this threshold is considerably lower than the previously recommended value [20]. This is not surprising as the cutoff values for MPE can be variable [20].
Furthermore, patients with lung adenocarcinoma demonstrated significantly higher levels of HE4 in pleural effusion than those with other histopathological types of lung cancer, highlighting the correlation of HE4 level in pleural effusion with the histopathology of lung cancer. This result is in accord with previous observations using serum samples, which demonstrated a significant correlation of serum HE4 level with histological type, TNM stage, and lymph node metastasis [16]. The ROC curve of lung adenocarcinoma against benign pleural effusion showed an AUC value of 0.881. At an HE4 level of 744.05 pmol/L, the sensitivity was 75.9% and the specificity was 85.7%, suggesting using the HE4 level in pleural effusion could significantly improve the diagnosis of lung adenocarcinoma. On the contrary, in pleural effusion caused by tuberculosis and inflammation, no significant difference was found in HE4 level. In addition, in pleural fluid with benign and malignant origins, the levels of HE4 are unrelated to sex, age, and smoking history.
In this study, the efficiency of the HE4 level in pleural effusion in predicting the prognosis of lung cancer was also investigated. Kaplan-Meier survival analysis showed no significant differences in the survival of patients with high and low levels of HE4. This is inconsistent with the results of a previous study using patient serum in which a higher HE4 level (
In summary, our data suggest that patients with MPE have a higher level of HE4 than those with pleural effusion from tuberculosis and inflammation. In particular, patients with lung adenocarcinoma tend to have a higher level of HE4 in pleural effusion than those with squamous cell carcinoma and small cell carcinoma. Our results suggest that HE4 in pleural effusion can be employed as a biomarker in the diagnosis of malignant lung cancer.