The etiology of prostate cancer (PCa) is multi-factorial including environmental and genetic factors. Present study evaluates the association between level of pesticides, stress level and CYP1A1 gene polymorphism with PCa patients.
METHODS:
A case control study was conducted with 102 PCa patients and age match symptomatic ( 107) and asymptomatic benign prostatic hyperplasia (BPH, 70) patients. Pesticide level was characterized by Gas Chromatography. The oxidative stress and scavenging mechanisms were determined by biochemical method. Two polymorphisms of CYP1A1 gene, rs4646903 and rs1048943, were analyzed by polymerase chain reaction (PCR) followed by restriction fragment length polymorphism and allele specific PCR method.
RESULTS:
Higher level of pesticide namely beta-hexachlorocyclohexane (-HCH), Malathion, Chlorpyrifos and Fenvalerate were found in PCa group (all value: 0.05). Kruskal Wallis H test depicted that level of -HCH and Malathion significantly correlated with higher grade of PCa (all 0.05). The PCa Patients with simultaneously low antioxidant activity and high stress level tended to suffer worst clinical outcomes. Dominant model of rs4646903 and rs1048943 suggested that substitution is associated with a higher risk of PCa (OR: 2.2, CI: 1.6–3.8, : 0.009 and OR: 1.95, CI: 1.1–3.4, : 0.026; respectively) and this risk was also influenced by smoking and pesticide exposure.
CONCLUSION:
Environmental and genetic factors are reported to raise risk; person with high level of these pesticides especially in high risk genotype might be more susceptible to PCa.
Prostate cancer (PCa) is a commonly diagnosed malignant tumor that occurs in aging men. In developed European countries, it is recognized as the most common solid tumor, with the highest incidence rate [1]. Incidence of PCa in Indian population is very low than United States and European nations. But, as a result of migration, changing lifestyle, increasing awareness regarding PCa, more and more cases are being discovered and at this time PCa is the second most frequently diagnosed cancer in metro cities of India [2].
Risk factors of PCa are multi-factorial, including age, environmental factors like pesticides and metals, family or personal history of cancer, smoking, tobacco chewing etc. Environmental pesticides are subject to serious concern because of broad range of toxicity. In the majority of cases human exposure is unintentional and unintended. Pesticides are lipophilic in nature, they remains in environment and body for a long period [3]. Due to their long biological half life, these compounds are widely persistent and even more noxious to human. Studies also suggested that several pesticides and their derivatives have both estrogenic and androgenic effects that disrupt the normal physiological function of endogenous hormone and may act as tumor promoter [3, 4, 5].
Loss and gain of gene function may manipulate disease susceptibility in an individual. Any variation of xenobiotic metabolizing enzyme, which is responsible for detoxification of environmental xenobiotics may have evident effect on metabolism of environmental carcinogens in the human body. Cytochrome p450 (CYP) 1A1 is a phase I enzyme required for the metabolism of steroids, xenobiotic chemicals and different potential genotoxic compounds [6]. CYP1A1 gene is located on chromosome 15q24.1 and has seven exons and six introns. Among all variant alleles of CYP1A1 gene, four polymorphic alleles m1, m2, m3 and m4 have been studied mostly for the association with different cancer [3, 6, 7]. The gene situated at position 3801 (rs4646903T C) in the 3’-non-coding region is involved in different cancers, including head-and-neck cancer, Breast cancer and PCa [4, 6], and m2 (rs1048943A G) has been correlated with lung cancer in Chinese population [8]. To date, data supporting that CYP1A1 polymorphism contributing to pesticides-associated PCa are scanty and controversial. The present study was designed to evaluate the role of pesticides, induced oxidative stress metabolism and CYP1A1 gene polymorphism in the etiology of PCa. In this study, m3 and m4 variant are excluded because m1 is prevalent in African-American and m4 was almost negligible in Asian population [7].
Materials and methods
Chemicals
Standards of pesticide namely, alpha-hexachlorocy- clohexane (-HCH), beta-(-HCH), malathion, chlorpyrifos, -endosulfan; dichlorodiphenyldichloroethylene (pp-DDE), dichloro diphenyltrichloroethane (pp-DDT), -ensosulfan, cypermethrin, and fenvalerate were procured from Sigma Aldrich (St. Louis, Mo., USA), having purity higher than 98%. Lichrosolv HPLC grade hexane was obtained from Merck Pvt. Ltd., Mumbai, India.
Ethical statement and sample size
Necessary ethical clearance was obtained by the Institutional Research Ethics Committee (Reference code: 61th ECMII-BP25) of King George’s Medical University (KGMU), Lucknow, India. The sample size was calculated on the basis of mean difference of stress level in exposed benign prostatic hyperplasia (BPH) and PCa group. In a study Siddique et al. [9] reported that the mean ( SD) oxidative stress in BPH subject was 6.7 2.9 while 8.7 4.0 in PCa patients. For getting final sample size by assuming-Difference 5.0; standard deviation () 5.0; an equal number of case and control ( 1:1); 1.96 (Significant level at 5%) and 0.84 (power 80%). Then, the required sample size was calculated by using the following formula.
Here, Sample size of each group; ratio of control to case; Differences effect size; Significant level; power (80%). The calculated number of sample for this study was 63. But for statistical point of view we were enrolled 102 cases and 177 control subjects.
Study subjects
In total, 102 PCa patients and 177 age matched controls were enrolled in this study. Prostate specific antigen (PSA) is a tissue specific marker that is now widely used for assessment as well as follow-up of PCa patients. In this study, diagnosis of PCa was based on the level of serum PSA (Chemiluminescent Microparticle Immunoassay) followed by histopathological investigation (based on Gleason score). Only histopathologically confirmed cases were enrolled as PCa patients. Age match control subjects were subdivided into two groups: symptomatic BPH (S-BPH, 107) and asymptomatic BPH (A-BPH, 70). S-BPH was recruited on the basis of chest x-ray, urine and blood test for PSA, colon enema and abdominal ultrasound. Age matched asymptomatic BPH controls were randomly selected among healthy volunteers visiting the outpatient department (OPD) of Urology, King George’s Medical University for their annual physical examination. Subjects with history of acute/chronic prostatitis; liver failure and renal failure, diabetes mellitus were excluded from this study. A written informed consent was obtained from each subject prior to their inclusion in this study.
List of primer enzyme, PCR condition and product length
Gene
Primer
Restriction enzyme
Product length (base pair)
CYP1A1m1: rs4646903T C
F 5-AAGAGGTGTAGCCGCTGCACT-3 and
Msp1
AM-340, Wh-340, HM-200,
R 5-TAGGAGTCTCT-CATGCCT-3
Mh-140
CYP1A1m2: rs1048943A G
(mt)F-5-AAGTGTATCGGTGAGACCA-3,
NA (ASP)
205
(wt)F-5-GAAGTGTATCGGTGAG-ACCG-3 and
CommR-5-GTAGACAGAGTCTAGGCCTCA-3.
NA: Not applicable; ASP: Allele specific primer; AM: Amplified fragment; Wh: Wild type Normal homozygous; HM: Heterozygous mutant; Mh: Mutant homozygous.
All the subjects were asked about, age, family history of cancer, dietary habit (vegetarian/non vegetarian), pesticide exposure history (farmers who actively participated in pesticide mixing and application to control crop pest) and lifestyle factors like alcohol consumption (50 drink/year) and smoking. Smoking status was divided into non smoker and established cigarette smoker according to the detail questions which are as follows: “Have you smoked at least 100 cigarettes in your life?” and “Do you now smoke cigarettes?” those respondents considered as non smoker who smoked fewer than 100 cigarettes in their entire life and they have not smoked since 5 years. Current smoker consist of those respondents who report smoking more than 100 cigarettes in their lifetime, and currently smoke every day or some day. After written consent, 5 ml venous blood was collected from each participant and divided into three parts for pesticide quantification (1.5 ml), oxidative stress (1.5 ml) and genotyping (2 ml) and stored at 80C till analysis.
Pesticides extraction and quantification
Extraction of organochlorine (OCPs) and organo- phosphate (OPPs) residue from blood was done according to method of Bush et al. [10]. The trace level pesticide (mg/ml or ppm) in the blood sample was analyzed by using Agilent technologies 7890A Gas Chromatograph, equipped with a micro Electron Capture Detector (ECD), capillary column DB-5MS (Perkin Elmer, CA, USA) of 30 m length, 0.25 mm i.d., 0.25 m thickness and in an auto injector Agilent technologies 7683B series split-less mode injector with an insert liner of 0.75 mm i.d. The gas chromatograph temperature was programmed as follows: injector temperature: 250C, oven temperature: initially ramped from 165C to 180C at a rate of 3C, 200C at a rate of 1.5C, 230C at a rate of 2C, 260C at a rate of 3.5C and finally to 280C at a rate of 6C per min withhold time of 1.5, 0.5, 0.5, 0.5, 2 and 2.5 min, respectively and electron capture detector temperature was at 300C.
Biochemical estimation
Reactive oxygen species (ROS) (n mole of malondialdehyde (MDA)/ml of plasma) were assessed by Ohkawa et al. [11] using thiobarbituric acid. The antioxidant system including superoxide dismutase (SOD), Catalase (CAT) and Glutathione (GSH) were also measured as per standard protocol [12, 13, 14, 15].
DNA isolation and genotyping
Genomic DNA was isolated by conventional phenol chloroform extraction method followed by ethanol precipitation and re-suspended in 1 mole Tris-EDTA buffer (pH: 8.0) and stored at 20C for further use. Genotyping of CYP1A1 at site rs4646903T C and rs1048943A G were carried out by single nucleotide polymorphism and allele specific polymerase chain reaction with specific primers and restriction enzyme (Table 1). Genotyping was done by using Applied Biosystem TaqMan SNP genotyping assay with stepOnePlus Real-time PCR system (Applied Biosystem, Foster City, USA).
Baseline characters of subjects
Variable
PCa
S-BPH
A-BPH
PCa vs S-BPH
PCa vs A-BPH
( 102),
( 107),
( 70),
OR (95% CI),
OR (95% CI),
(%)
(%)
(%)
value
value
Age
60
71
39
27
Reference
Reference
60
31
68
43
0.25 (0.14–0.44), 0.001
0.27 (0.144–0.52), 0.001
Tobacco consumption (smoking)
No
11 (10.8)
33 (30.8)
47 (67.1)
Reference
Reference
Yes
91 (89.2)
74 (69.1)
23 (32.8)
3.68 (1.7–7.8), 0.0004
16.9 (7.59–37.62), 0.001
Alcohol consumption
No
16 (15.7)
26 (24.3)
17 (24.2)
Reference
Reference
Yes
86 (84.3)
81 (75.7)
53 (75.7)
1.72 (0.86–3.44), 0.12
1.72 (0.80–3.7), 0.15
Family history (any type of malignancy)
No
97 (95.3)
–
–
Yes
5 (4.7)
–
–
Dietary habit
Non-vegetarian
35 (34.3)
28 (26.2)
18 (25.7)
Reference
Reference
Vegetarian
67 (65.7)
79 (73.8)
52 (74.2)
0.68 (0.37–1.22), 0.198
0.66 (0.33–1.30), 0.23
Occupational exposure of pesticides
Others
20 (19.6)
47 (43.9)
38 (54.2)
Reference
Reference
Farmer
82 (80.4)
60 (56.1)
32 (45.7)
3.21 (1.7–5.9), 0.002
4.86 (2.47–9.59), 0.001
PSA (ng/ml)
4
5
84
–
Reference
4–10
20
14
–
24 (7.74–74.41), 0.001
10–20
40
7
–
96 (28.69–321.2), 0.001
20
37
2
–
310 (57.65–1676), 0.001
PCa: Prostate cancer; S-BPH: Symptomatic BPH; A-BPH: Asymptomatic BPH; For Significance: 2 2 chi squire test was used; OR: Odds ratio; CI: Confidence interval; : Probability; : 0.05. In PSA: Univariate logistic regression analysis was used.
Distribution of pesticides in prostate cancer (PCa) and BPH control groups
Pesticides (ppm)
PCa
S-BPH control
A-BPH control
value
( 102)
( 107)
( 70)
25%
50%
75%
25%
50%
75%
25%
50%
75%
PCa Vs S-BPH
PCa Vs A-BPH
Malathion
1.21
2.20
3.95
0.68
1.26
2.06
0.77
1.16
3.74
0.001
0.09
Chlorpyrifos
0.21
0.29
0.75
0.14
0.22
0.27
0.11
0.22
0.40
0.002
0.14
-HCH
0.52
0.84
1.85
0.43
0.78
1.38
0.06
0.34
0.51
0.24
0.001
-HCH
0.01
0.01
0.04
0.01
0.003
54.2
0.01
0.002
0.04
0.023
0.611
-Endosulfan
0.45
0.51
0.80
0.45
0.57
0.85
0.07
0.33
0.49
0.57
0.001
pp-DDE
0.17
0.39
0.79
0.16
0.23
0.43
0.14
0.22
0.33
0.05
0.07
-ensosulfan
0.51
0.62
0.95
0.43
0.53
0.77
0.21
0.34
0.57
0.08
0.0001
DDT
0.48
0.69
0.86
0.55
0.70
0.95
0.15
0.34
0.57
0.55
0.002
Cypermethrin
0.26
0.56
1.42
0.39
0.62
0.96
0.28
0.51
0.69
0.66
0.244
Fenvalrate
0.86
1.24
2.03
0.51
0.98
1.56
0.38
0.56
0.90
0.04
0.0001
S-BPH: Symptomatic BPH; A-BPH: Asymptomatic BPH. For significance calculation Mann Whitney U test was used; 0.05.
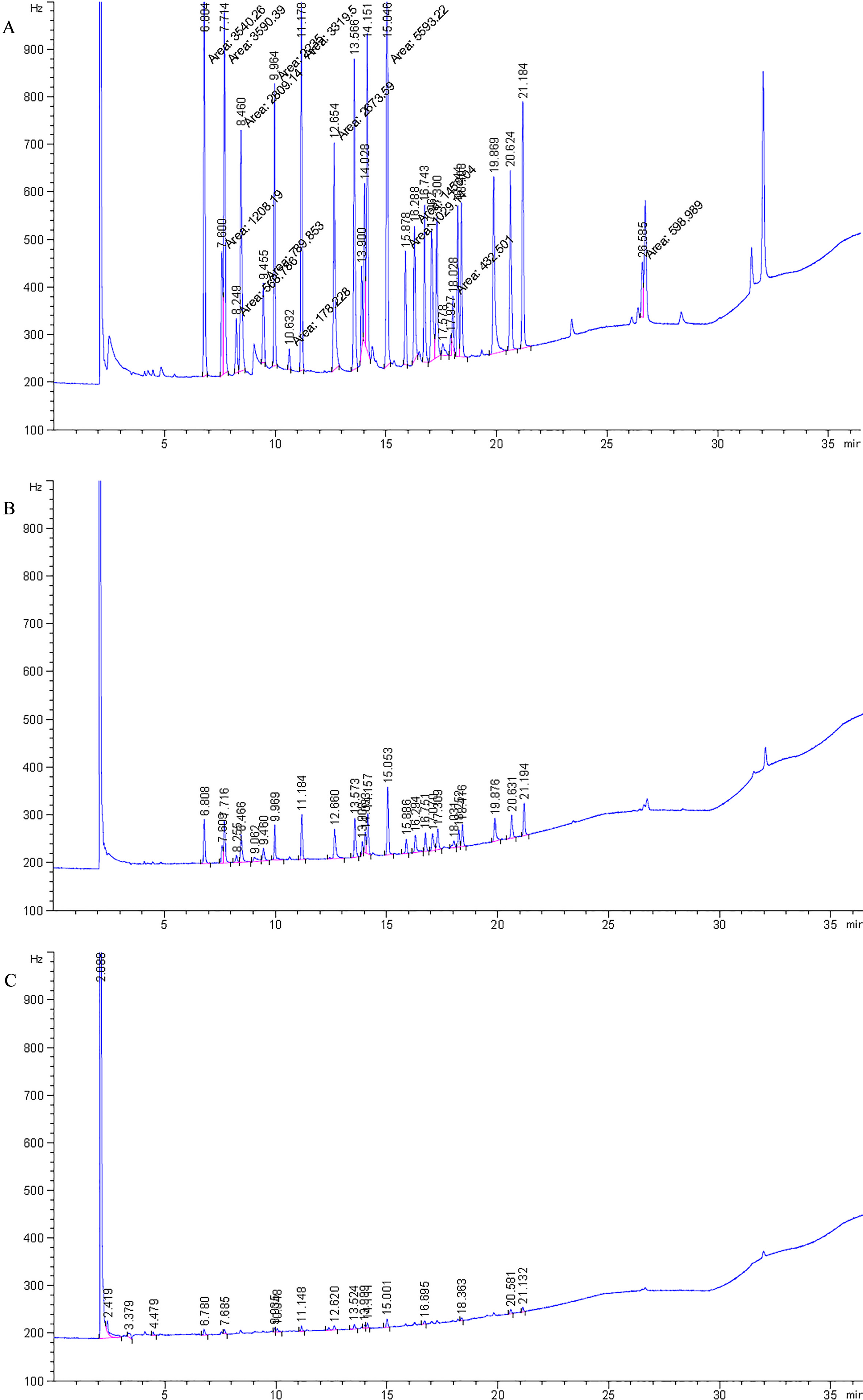
GC chromatogram of detected pesticides in Prostate cancer (A), Symptomatic BPH (B) and Asymptomatic BPH (C).
Distribution of pesticides in prostate cancer patients
Pesticides (ppm)
Low risk
Intermediate risk
High risk
value
GS 5 & 6
GS 7
GS 8 & 9
( 19)
( 47)
( 36)
Malathion
1.68 (0.80–3.72)
2.08 (0.99–3.89)
3.58 (1.71–4.17)
0.042
Chlorpyrifos
0.27 (0.18–0.71)
0.28 (0.21–1.67)
0.29 (0.18–0.59)
0.742
-HCH
0.67 (0.55–1.68)
0.78 (0.41–1.77)
1.00 (0.65–2.16)
0.24
-HCH
0.01 (0.001–0.024)
0.02 (0.009–0.04)
0.02 (0.008–0.04)
0.04
-endosulfan
0.45 (0.42–0.73)
0.51 (0.41–0.81)
0.56 (0.46–0.84)
0.444
pp-DDE
0.46 (0.25–0.54)
0.29 (0.14–0.72)
0.43 (0.21–1.07)
0.508
-ensosulfan
0.52 (0.45–0.63)
0.66 (0.48–0.103)
0.69 (0.58–0.97)
0.245
DDT
0.49 (0.29–0.93)
0.72 (0.51–0.85)
0.65 (0.47–0.98)
0.359
Cypermethrin
0.74 (0.40–1.52)
0.59 (0.31–1.45)
0.51 (0.23–1.27)
0.616
Fenvalrate
1.38 (0.97–5.13)
1.33 (0.68–5.05)
1.21 (0.86–4.57)
0.754
GS: Gleason Score; N is varying in pesticides. Value in Median (inter-quartile). Kruskal-Wallis H Test was used to calculate significance level; 0.05.
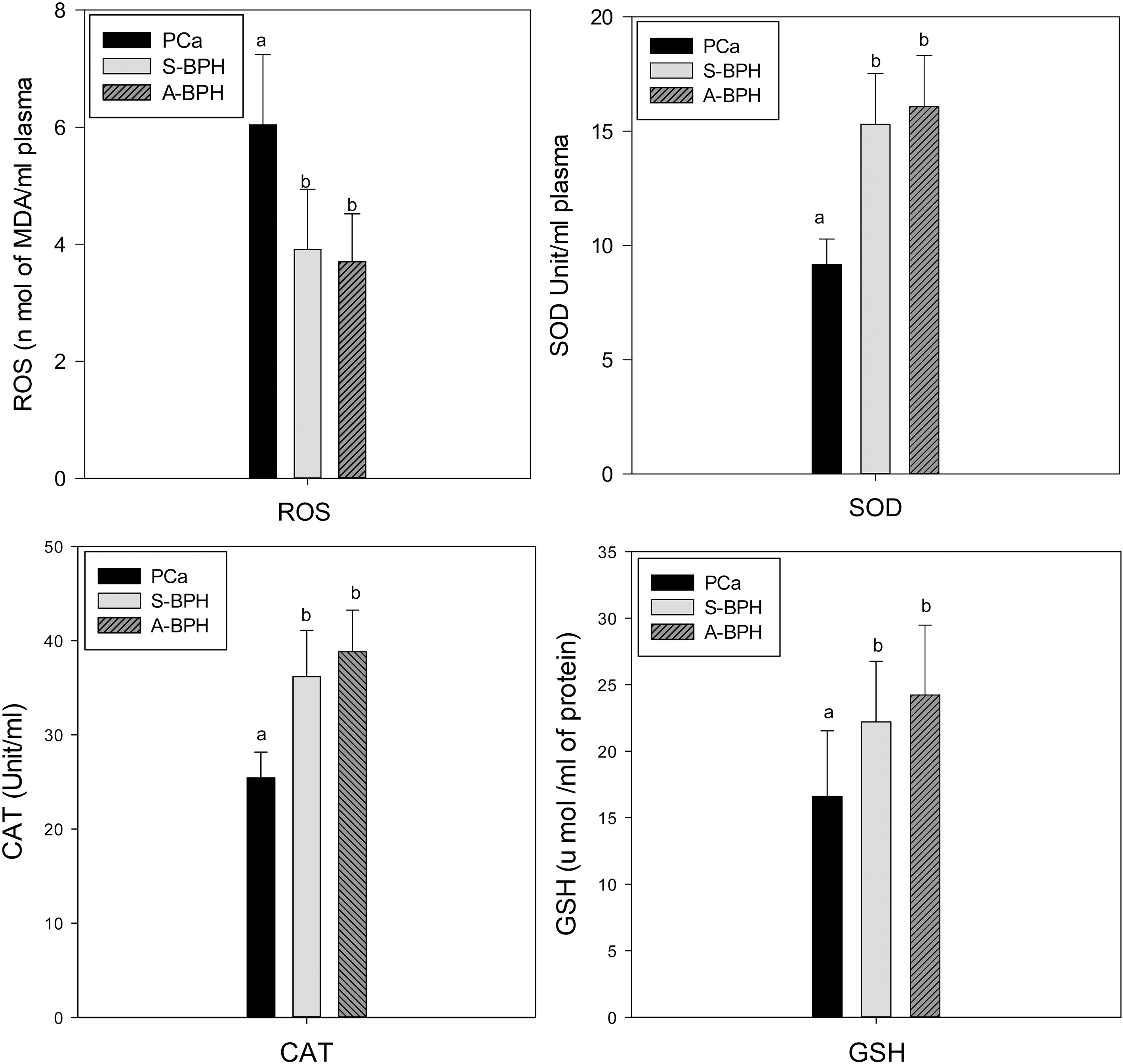
Distribution of ROS and Antioxidants (SOD, CAT, GSH) in PCa and Symptomatic and Asymptomatic BPH control. Significance was calculated by post hoc Tukey one way ANOVA test at 0.05.
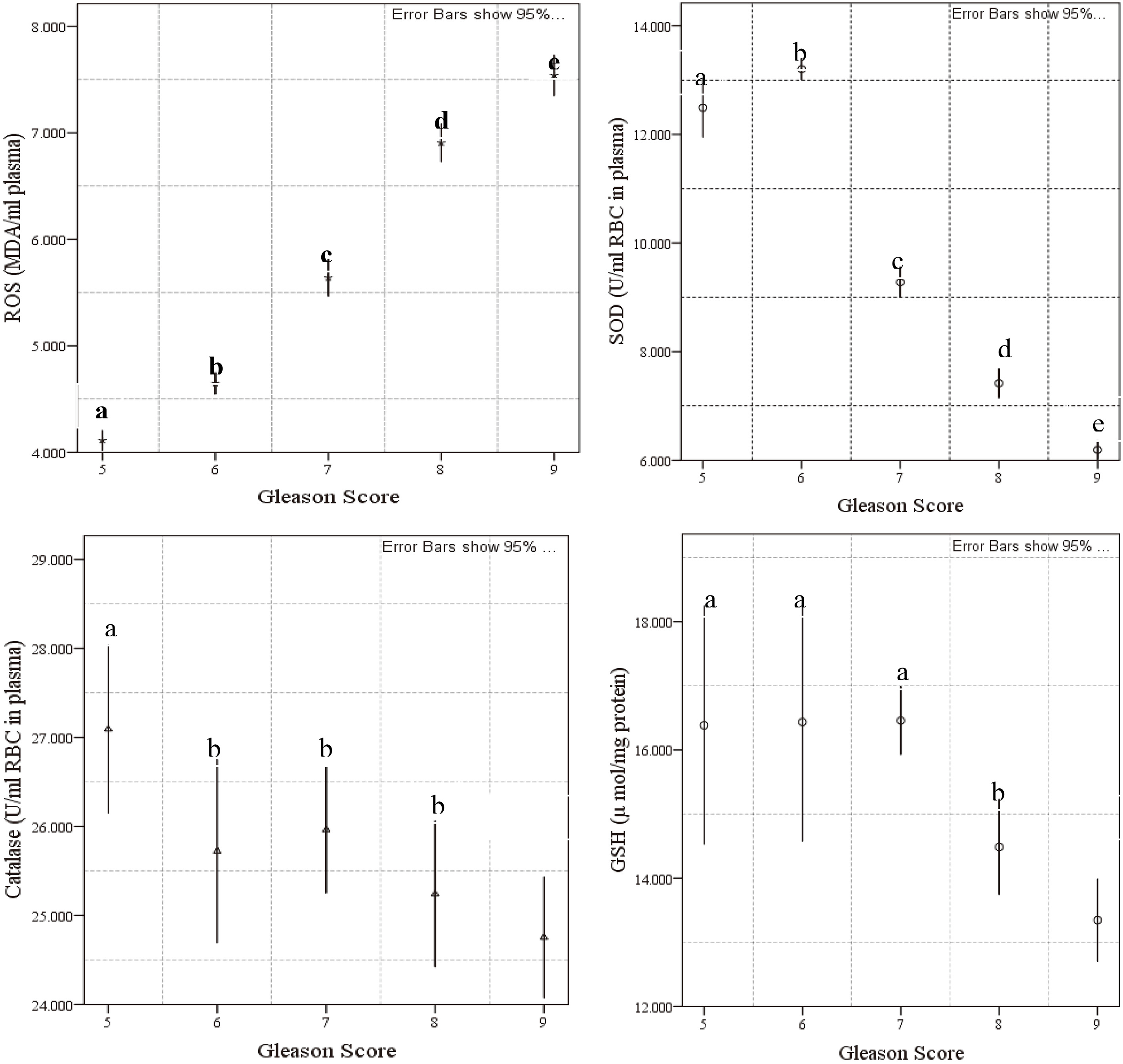
Distribution of ROS and antioxidants (SOD, Catalase, and GSH) in PCa. Different alphabets in separate figure showed significant variation. Significance was calculated by post hoc Tukey one way ANOVA at 0.05.
Statistical analysis
For continuous data, normality was tested using Kolmogorov Smirov test. For non normal continuous data, test, mann whitney U test/kruskal wallis H test were used to compare the groups as appropriate [16]. Categorical data were presented in frequency and percentage. For PSA, Univariate binary logistic regression analysis was used to calculate unadjusted odds ratio (OR) and 95% confidence interval (CI) in different variables between case controls. One way analysis of variance (ANOVA) followed by Tukey post hoc test were applied on multiple comparisons between the stress metabolism and Gleason score (GS). The genotypic data are in Hardy-Weinberg Equilibrium tested by test. Genotypic data was compared between case and controls using 2 3 and 2 2 contingency table calculator available online at (http://faculty.vassar.edu/lowry/VassarStats.html). In the case of statistical significance, further genotypic analysis to calculate the OR and CI were undertaken using dominant and recessive models of comparison. Statistical analysis was carried out using the statistical package for the social science, version 22 (SPSS-22, IBM, Chicago, USA). 0.05 was considered as statistically significant.
Results
General baseline characters
Baseline profiles of selected subjects are shown in Table 2. Tobacco consumption was found to be predominant risk factor for PCa than both BPH group (PCa versus S-BPH: OR: 3.68; 95% CI: 1.7–7.7; : 0.001 and PCa versus A-BPH: OR: 16.9; 95% CI: 7.59–37.62; : 0.001). The proportion of occupational exposure of pesticide was significantly higher in the group with PCa (PCa: 80.4% versus S-BPH: 56.1% and PCa: 80.4% versus A-BPH: 45.7%; All 0.05). Stratified analysis showed that high level of serum PSA was strongly associated with PCa risk (all 0.001). Some PCa Patients recorded normal or low PSA level; this may be due to the orchiectomy or radical prostatectomy that they underwent. We enrolled healthy age matched A-BPH subjects and PSA testing was voluntary. Therefore statistical comparison of PSA between PCa and A-BPH group was restricted.
Quantification of pesticide by gas chromatography
Compared to BPH controls, PCa had high levels of pesticides (Fig. 1 and Table 3). For example, pesticides namely malathion, chlorpyrifos, -HCH, pp-DDE and fenvalerate were 2 to 4 fold higher in PCa than BPH groups (all 0.05). However, level of -HCH and malathion pesticides were correlated with high Gleason scores ( 0.05) which are an indicator of tumor aggressiveness (Table 4).
Oxidative stress and their scavenging system
Mean level of ROS (n mole of MDA/ml) was 3.91 1.03 and 3.7 0.82 in S-BPH and A-BPH whereas, in PCa group it was almost two fold higher (6.04 1.2). Further, SOD, CAT and GSH level decreased by 2 to 2.9 fold in PCa group than both BPH (all : 0.01) (Fig. 2). Among PCa group, rise in ROS and reduction in antioxidant level were associated with increasing Gleason score (all : 0.001) (Fig. 3). The association between ROS and antioxidants with serum PSA was found to be null (data not shown).
Frequencies of rs4646903T C and rs1048943A G gene polymorphism among prostate cancer (PCa) and control
All subjects
2 3 contingency
TT
TC
CC
OR (95% CI), value
PCa (, %)
27 (26.5%)
56 (54.9%)
19 (18.6%)
0.023
S-BPH (, %)
47 (43.9%)
48 (44.8%)
12 (11.2%)
Allele frequency PCa
110 (53.9%)
94 (46.1%)
Allele frequency S-BPH
142 (66.3%)
72 (33.6%)
Dom TT vs TCCC
PCa
27 (26.5%)
75 (73.5%)
Reference
S-BPH
47 (43.9%)
60 (56.0%)
2.17 (1.21–3.89) 0.008
Rec TTTC vs CC
PCa
83 (81.37%)
19 (18.63%)
Reference
S-BPH
95 (88.78%)
12 (11.22%)
1.81 (0.83–3.95) 0.131
AA
AG
GG
PCa (, %)
35 (34.3%)
53 (51.9%)
14 (13.7%)
0.05
S-BPH (, %)
54 (50.4%)
44 (41.1%)
9 (8.41%)
Allele frequency PCa
123 (60.3%)
81 (39.7%)
Allele frequency S-BPH
152 (71%)
62 (28.9%)
Dom AA vs AGGG
PCa
35 (34.31%)
67 (65.69%)
Reference
S-BPH
54 (50.47%)
53 (49.53%)
1.95 (1.12–3.4) 0.025
Rec AAAG vs GG
PCa
88 (86.27%)
14 (13.73%)
Reference
S-BPH
98 (91.58%)
9 (8.42%)
1.73 (0.71–4.2) 0.271
TT
TC
CC
OR (95% CI), value
PCa (, %)
27 (26.5%)
56 (54.9%)
19 (18.6%)
0.06
A-BPH (, %)
30 (42.8%)
32 (45.7%)
8 (11.4%)
Allele frequency PCa
110 (53.9%)
94 (46.1%)
Allele frequency A-BPH
82 (63.1%)
48 (36.9%)
Dom TT vs TCCC
PCa
27 (26.5%)
75 (73.5%)
Reference
A-BPH
30 (42.86%)
40 (57.14%)
2.08 (1.1–3.97) 0.024
Rec TTTC vs CC
PCa
83 (83.17%)
19 (18.63%)
Reference
A-BPH
62 (88.57%)
8 (11.43%)
1.77 (0.73–4.32) 0.201
AA
AG
GG
PCa (, %)
35 (34.3%)
53 (51.9%)
14 (13.7%)
0.062
A-BPH (, %)
36 (51.4%)
29 (41.4%)
5 (7.1%)
Allele frequency PCa
123 (60.3%)
81 (39.7%)
Allele frequency A-BPH
101 (72.1%)
39 (27.9%)
Dom AA vs AGGG
PCa
35 (34.32%)
67 (65.68%)
Reference
A-BPH
36 (51.42%)
34 (48.58%)
2.03 (1.08–3.77) 0.02
Rec AAAG vs GG
PCa
88 (86.27%)
14 (13.73%)
Reference
A-BPH
65 (92.85%)
5 (7.15%)
2.07 (0.71–6.03) 0.176
OR: Odds ratio; CI: 95% confidence interval; Dom: Dominant; Rec: Recessive; S-BPH: Symptomatic BPH; A-BPH: Asymptomatic BPH. 2 3 and 2 2 chi squire was used; : Asterisk indicates 0.05.
Statistical comparison of the rs4646903T C and rs1048943A G gene with potential risk factors among prostate cancer (PCa) and Symptomatic BPH (S-BPH)
rs4646903T C
TT
TC
CC
OR (95% CI), value
Smoker
Dom TT vs TCCC
PCa
26
(28.57%)
65
(71.43%)
1
S-BPH
33
(44.59%)
41
(55.41%)
2.01 (1.05–3.84) 0.033
Rec TTTC vs CC
PCa
74
(81.31%)
17
(18.69%)
1
S-BPH
67
(90.54%)
7
(9.46%)
2.19 (0.85–5.63) 0.094
Non smoker
Dom TT vs TCCC
PCa
4
(28.57%)
10
(71.43%)
1
S-BPH
14
(42.42%)
19
(57.58%)
1.84 (0.48–7.11) 0.371
Rec TTTC vs CC
PCa
9
(81.82%)
2
(18.18%)
S-BPH
34
(87.18%)
5
(12.82%)
Not applicable
Occupational exposure
Dom TT vs TCCC
PCa
14
(17.07%)
68
(82.93%)
1
S-BPH
22
(36.66%)
38
(63.33%)
2.8 (1.29–6.12) 0.008
Rec TTTC vs CC
PCa
69
(84.14%)
13
(15.85%)
1
S-BPH
51
(85%)
9
(15%)
1.06 (0.42–2.68) 0.88
Non exposure
Dom TT vs TCCC
PCa
13
(65%)
7
(35%)
1
S-BPH
24
(52.17%)
22
(47.83%)
0.58 (0.19–1.74) 0.33
Rec TTTC vs CC
PCa
13
(68.42%)
6
(31.57%)
1
S-BPH
38
(82.60%)
8
(17.40%)
2.55 (0.77–4.44) 0.199
rs1048943A G
AA
AG
GG
OR (95% CI), value
Smoker
Dom AA vs AGGG
PCa
31
(34.06%)
60
(65.94%)
1
S-BPH
39
(52.7%)
35
(47.3%)
2.15 (1.15–4.04) 0.016
Rec AAAG vs GG
PCa
80
(87.91%)
11
(12.08%)
1
S-BPH
67
(90.54%)
7
(9.46%)
1.32 (0.48–3.58) 0.59
Non smoker
Dom AA vs AGGG
PCa
3
(30%)
7
(70%)
Not applicable
S-BPH
15
(45.45%)
18
(54.46)
Rec AAAG vs GG
PCa
7
(70%)
3
(30%)
Not applicable
S-BPH
31
(93.93%)
2
(6.07%)
Occupational exposure
Dom AA vs AGGG
PCa
27
(32.92%)
55
(67.08%)
1
S-BPH
32
(53.33%)
28
(46.67%)
2.32 (1.17–4.61) 0.014
Rec AAAG vs GG
PCa
72
(87.8%)
10
(12.19%)
1
S-BPH
55
(91.66%)
5
(8.33%)
1.52 (0.49–4.72) 0.458
Non exposure
Dom AA vs AGGG
PCa
8
(40%)
12
(60%)
1
S-BPH
21
(45.65%)
25
(54.35%)
1.26 (0.43–3.66) 0.67
Rec AAAG vs GG
PCa
16
(80%)
4
(20%)
Not applicable
S-BPH
42
(91.30%)
4
(8.7%)
OR: Odds ratio; CI: 95% Confidence interval; Dom: Dominant; Rec: Recessive; 2 2 chi squire was used for significance calculation; : Asterisk indicates 0.05.
Genotyping and their relation with prostate cancer
Genotypic frequencies in both control groups were in Hardy-Weinberg equilibrium (S-BPH: 0.96 and A-BPH: 0.903). For rs4646903T C, the homozygous genotype (TT) was found to be high among controls (S-BPH: 43.9 and A-BPH: 42.8%). However, heterozygous genotype (TC) was significant more prevalent among PCa (54.9%) than controls (S-BPH: 44.8% and A-BPH: 45.7%) (Table 5). The frequency of minor allele CC was slightly higher in PCa patients (46.1%) than BPH group (S-BPH: 33.6%, A-BPH: 36.9%). Further, dominant model, reveals that risk was almost 2 fold high in PCa (PCa versus S-BPH: OR 2.17; CI: 1.6–3.8; 0.008 and PCa versus A-BPH: OR 2.08; CI: 1.1–3.97; 0.024).
In rs1048943A G, homozygous genotype (AA) was found to be more prevalent among controls (S-BPH: 50.4% and A-BPH: 51.4%) than PCa (34.3%). The frequency of wild-type allele was higher in group with both BPH controls, whereas minor allele genotype was higher in PCa patients. Dominant model indicated that PCa was associated with risk genotype (AGGG) of rs1048943A G (PCa versus S-BPH: OR 1.95; CI: 1.1–3.4 and PCa versus A-BPH: OR 2.03; CI: 1.8–3.77, all 0.05). We also analyzed genotypic data of symptomatic and asymptomatic BPH subject (Supplementary Table 7). Binary logistic analysis reveals that, symptomatic and asymptomatic BPH group was same at genetic level. Therefore, this combination of PCa and asymptomatic BPH was excluded from further genotypic analysis. Only one type of control is enough for comparing the genetic data with PCa group.
Association of CYP1A1 genotype with baseline risk variable
For estimation of possible correlation between selected two single nucleotide gene polymorphism with PCa risk, stratified analysis based on two major clinical risk factors including smoker, non-smoker and pesticide exposure and non exposure were performed. Dominant model showed that the combined risk genotype (TCCC and AGGG) of CYP1A1 gene had a significant association to those cancer patients who were smoker and exposed to pesticides (Table 6).
Discussion
The impact of environmental exposure on different cancer has been studied in various ethnic groups [17, 18]. In this study, occupationally exposed men had 3 to 4 fold higher risk of PCa. Another notable difference was found in tobacco consumption in the form of smoking. Tobacco consumption in any form affects plasma steroid hormone level and leads to higher testosterone concentration. Nicotine causes lead to dihydro-testosterone accumulation in prostate [19]. An elevation in prostate androgens, particularly the more potent dihydro-testosterone may be lead to an elevated risk of PCa as well as Symptomatic BPH [20].
Chemical pesticides disrupt normal endocrine function and are related to various hormone mediated malignancies [3]. Since, PCa is hormone-dependent malignancy; this study is focused on relationship between different type of pesticides and PCa. We selected 10 pesticides on the basis of persistent nature and consumption rate in northern part of India [21]. Despite low concentration, majority of pesticide were detected in blood of PCa patients along with both BPH group. We found high median level of five and seven pesticides in PCa group than S-BPH and A-BPH group, respectively. Pesticides like Fenvalerate and DDT have anti-androgenic or estrogenic potential. On other hand, HCH pesticide and its isomer have both estrogenic and anti-estrogenic potential [21]. These pesticides are known to have carcinogenic potential even at very low concentration [22]. Stratified analysis of PCa group based on Gleason score was found that -HCH and Malathion pesticides were associated with high risk of PCa (all 0.05). This result was consistent with Kumar et al. [7] who previously reported that, there was an association between pesticide level and Prostate cancer in Indian population. However, it has been reported that serum concentration of HCH and dieldrin were significantly associated with prostate cancer risk in the United States population [18]. Moreover, Xu et al. [23] found a group of pesticides like methyl bromide showed prostate specific biological effects. This study provides evidence of relationship between PCa and ambient pesticide exposures.
Several mechanisms of carcinogenesis have been suggested and proposed, the most important appears to be oxidative stress. A significant higher level of ROS was found in PCa group than BPH. SOD, CAT and GSH are considered primary antioxidants involved in direct scavenging of ROS. In our study, SOD, CAT and GSH levels were found to be significantly low in PCa group [24]. Stratified analysis of PCa group based on Gleason score revealed that, Gleason score positively correlated with ROS and negatively correlated with antioxidants. Several independent studies suggest that the reduction of antioxidant activity increases the toxic effect of ROS and may lead to severe cellular and molecular damage [25]. SOD catalyzes the dismutation of superoxide into HO and O, while CAT and GSH remove HO. Decrease in antioxidant activity can lead to excessive accumulation of ROS resulting in initiation and propagation of cellular damage which induces tumor aggressiveness [24].
In genetic studies, the average effect of single locus can be estimated by an additive model. In presence of dominance, the additive model is expected to be more accurate. Broadly additive model are divided into two types dominant and recessive model. In dominant model, comparison groups are wild-type homozygous genotype verses allele positivity (combination of hetero and minor allele) whereas in recessive model, comparison groups are minor allele verses the rest (combination of wild-type and heterozygous genotype). Published data on rs4646903T C and rs1048943A G genes polymorphism in PCa lack consensus. Only one study from Indians have analyzed rs4646903T C and rs1048943A G locus in Prostate cancer [7]. Based on dominant model we observed that the rs4646903T C and rs1048943A G substitution significantly increase the risk of PCa in northern Indian patients. The PCa group exhibits a far high frequency of substitution than BPH. Mittal et al. [26] who previously reported that if genotype containing at least one copy of mutated allele (TC, CC or AG, GG) then the risk was two fold high in PCa. Moreover, Ding et al. [27] suggested that individual carrying combined risk genotype of CYP1A1 (TCCC or AGGG) was more susceptible to PCa. However, these findings were contradicted by a Meta analysis which showed that instead of heterozygous or mutant genotype, homozygous wild-type genotype of CYP1A1 was associated with increased PCa risk [28]. Another case control study along with a Meta analysis showed that there was no correlation between CYP1A1 gene and PCa [29, 30]. The difference of this result might be due to different genetic makeup amongst different ethnicity.
Regarding link between CYP1A1 genotype and demographic risk factors in men, the most compelling data comes from the agriculture sector [17, 31, 32]. Several other factors like pesticide exposure, smoking and diet, may influence the risk of different type of cancer [6]. In present study, smoking and occupational exposure were considering as main baseline risk factors therefore these two variables were subjected into genetic analysis. We observed that smoking and occupational exposure had two and three times higher risk for PCa. In corroboration with above findings, studies conducted in India and other countries also revealed that baseline risk variables like smoking and occupational exposure may contribute to the genetic etiology of different type of cancer including PCa [6, 32].
There are few limitations to our study. First, this is a single centric study and sample size is not enough to explain statistical power for stratified analysis. India is being a multi-ethnic country (like Dravidians, Indo-Europian and Tibeto-Burman) and genetic polymorphism being subject to ethnic variation. The gene pool is still conserve because of caste system, hence results of this study, should be validated by further investigations looking into the ethnic variation involved in these polymorphism from other part of India.
In conclusion, our study suggested that use of pesticide has affected human health via oxidative pathway. Further, rs4646903T C and rs1048943A G polymorphism are associated with increased risk of PCa and the risk was also influence by smoking and pesticide exposure. Further, studies are needed to validate our results in multi-centric study with large population.
Footnotes
Acknowledgments
This work was supported by Council of Science and Technology (Letter no. CST/SERPD/D-1391), Uttar Pradesh, India. Authors are also thankful to Director, CSIR-IITR, Lucknow, India for providing the instrumental support.
Conflict of interest
None.
Supplementary data
Comparison of CYP1A1 genotypic data in symptomatic and asymptomatic BPH
Genotype
Symptomatic BPH (, %)
Asymptomatic BPH (, %)
OR (95% CI)
value
rs4646903T C
TT
47 (43.9%)
30 (42.8%)
Reference
TC
48 (44.8%)
32 (45.7%)
0.95 (0.50–1.8)
0.89
CC
12 (11.2%)
8 (11.4%)
0.95 (0.35–2.6)
0.93
TCCC
60 (56%)
40 (57.1%)
0.95 (0.52–1.76)
0.88
rs1048943A G
AA
54 (50.4%)
36 (51.4%)
Reference
AG
44 (41.1%)
29 (41.4%)
1.01 (0.53–1.9)
0.97
GG
9 (8.41%)
5 (7.1%)
1.2 (0.37–3.8)
0.76
AGGG
53 (49.5%)
34 (48.5%)
1.03 (0.56–1.89)
0.88
OR: Odds ratio; CI: 95% confidence interval; 2 2 chi squire was used for significance calculation; : Asterisk indicates 0.05.
References
1.
BaadeP.D.YouldenD.R.CrambS.M.DunnJ. and GardinerR.A., Epidemiology of prostate cancer in the Asia-Pacific region, Prostate Int1(2) (2013), 47–58.
2.
JainS.SaxenaS. and KumarA., Epidemiology of prostate cancer in India, Meta Gene2 (2014), 596–605.
3.
GeorgeJ. and ShuklaY., Pesticides and cancer: Insights into toxicoproteomic-based findings, J Proteomics74 (2011), 2713–2722.
4.
Landau-OssondoM.RabiaN.Jos-PelageJ.MarquetL.M.IsidoreY.Saint-AimeC.MartinM.IrigarayP. and BelpommeD., Why pesticides could be a common cause of prostate and breast cancers in the French Caribbean Island, Martinique. An overview on key mechanisms of pesticide-induced cancer, Biomed Pharmacotherapy63 (2009), 383–395.
5.
HuW.Y.ShiG.B.LamH.M.HuD.P.HoS.M.MaduekeI.C.Kajdacsy-BallaA. and PrinsG.S., Estrogen-initiated transformation of prostate epithelium derived from normal human prostate stem-progenitor cells, Endocrinol152 (2011), 2150–2163.
6.
SharmaR.AhujaM.PandaN.K. and KhullarM., Combined effect of smoking and polymorphisms in tobacco carcinogen-metabolizing enzymes CYP1A1 and GSTM1 on the head and neck cancer risk in North Indians, DNA Cell Biol29 (2010), 441–448.
7.
KumarV.YadavC.S.SinghS.GoelS.AhmedR.S.GuptaS.GroverR.K. and BanerjeeB.D., CYP 1A1 polymorphism and organophosphate pesticides levels in the etiology of prostate cancer, Chemosphere81 (2010), 464–468.
8.
BagA.JyalaN.S. and BagN., Cytochrome P450 1A1 genetic polymorphisms as cancer biomarkers, Indian Journal of Cancer52(4) (2015), 479.
9.
SiddiqueM.K.J.SrivastavaS. and MehrotraP.K., Environmental exposure to lead as a risk for prostate cancer, Biochem. Environ Sci15 (2002), 298–305.
10.
BushB.SnowJ. and KoblintzR., Polychlorobiphenyl (PCB) congeners, p,p’-DE and hexachlorobenzene in maternal and fetal cord blood from mothers in upstate New York, Arch Environ Contam Toxicol13 (1984), 517–527.
11.
OhkawaH.OhishiN. and YagiK., Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction, Anal Biochem95 (1979), 351–358.
12.
KakkarR.ManthaS.V.RadhiJ.PrasadK. and KalraJ., Increased oxidative stress in rat liver and pancreas during progression of streptozotocin-induced diabetes, Clin Sci94 (1998), 623–632.
13.
McCordJ.M. and FridovichI., Superoxide dismutase. An enzymic function for erythrocuprein (hemocuprein), J Biol Chem244 (1969), 6049–6055.
14.
AebiH.CantzM. and SuterH., Cellular distribution of catalase activity in red cells of homozygous and heterozygous cases of acatalasia, Experientia21 (1965), 713–714.
GerstmanB., Basic biostatistics for public health practice, Jones and Bartlett Learning press 2nd edition, Burlington 2014, 77–526.
17.
AlavanjaM.C.SamanicC.DosemeciM. et al., Use of agricultural pesticides and prostate cancer risk in the Agricultural Health Study cohort, Am J Epidemiol157 (2003), 800–814.
18.
CockburnM.MillsP.ZhangX.ZadnickJ.GoldbergD. and RitzB., Prostate cancer and ambient pesticide exposure in agriculturally intensive areas in California, Am J Epidemiol173 (2011), 1280–1288.
19.
FieldA.E.ColditzG.A.WillettW.C. et al., The relation of smoking, age, relative weight, and dietary intake to serum adrenal steroids, sex hormones, and sex hormone-binding globulin in middleaged men, J Clin Endocrinol Metab79 (1994), 1310–1316.
20.
KobrinskyN.L.KlugM.G.HokansonP.J.SjolanderD.E. and BurdL., Impact of smoking on cancer stage at diagnosis, J Clin Oncol21 (2003), 907–913.
21.
MishraK. and SharmaR.C., Assessment of organochlorine pesticides in human milk and risk exposure to infant from north-east India, Sci Total Environ409 (2011), 4939–4949.
22.
MishraK.SharmaR.C. and KumarS., Contamination level and spatial distribution of organochlorine pesticides in soil from India, Ecotoxicol Environ Safety76 (2012), 215–225.
23.
XuX.DaileyA.B.TalbottE.O.IlacquaV.A.KearneyG. and AsalN.R., Associations of serum concentrations of organochlorine pesticides with breast cancer and prostate cancer in US, Adults Environ Health Prospect118 (2010), 60–66.
24.
ThapaD. and GhoshR., Antioxidants for prostate cancer chemoprevention: challenges and opportunities, Biochem Pharmacol83 (2012), 1319–1330.
25.
ReuterS.GuptaS.C.ChaturvediM.M. and AggarwalB.B., Oxidative stress, inflammation, and cancer: How are they linked? Free Radical Biol Medicine49 (2010), 1603–1616.
26.
MittalR.D. and SrivastavaD.L., Cytochrome P4501A1 and microsomal epoxide hydrolase gene polymorphisms: gene-environment interaction and risk of prostate cancer, DNA Cell Biol26 (2007), 791–798.
27.
DingG.XuW.LiuH.ZhangM.HuangQ. and LiaoZ., CYP1A1 MspI polymorphism is associated with prostate cancer susceptibility: evidence from a meta-analysis, Mol Biol Reports40(5) (2013), 3483–3491.
28.
OuC.ZhaoY.LiuJ.H.ZhuB.LiP.Z. and ZhaoH.L., Relationship between aldosterone synthase CYP1A1 mspi gene polymorphism and prostate cancer risk, Technol Cancer Res Treat (2016). doi: 10.1177/1533034615625519.
29.
MandicS.HorvatV.MarcziS.LukicI. and GalicJ., Association study of cytochrome P450 1A12A polymorphism with prostate cancer risk and aggressiveness in Croatians, Coll Antropol38(1) (2014), 141–146.
30.
ZhuW.LiuH.WangX.LuJ.ZhangH.WangS. and YangW., Associations of CYP1 polymorphisms with risk of prostate cancer: an updated meta-analysis, Bioscience Reports39(3) (2019), 29.
31.
BandP.R.AbantoZ.BertJ.LangB.FangR.GallagherR.P. and LeN.D., Prostate cancer risk and exposure to pesticides in British Columbia farmers, Prostate71 (2011), 168–183.
32.
ChristensenC.H.BarryK.H.AndreottiG. et al., Sex steroid hormone single-nucleotide polymorphisms, pesticide use, and the risk of prostate cancer: a nested case-control study within the agricultural health study, Frontiers in Oncology6 (2016), 237.