This study aimed to explore the correlation of CD45 expression with clinicopathological features and treatment outcomes in elderly acute myeloid leukemia (AML) patients.
METHODS:
One hundred and twenty one elderly patients with de novo AML were consecutively recruited in this prospective cohort study, bone marrow samples from all patients were collected and CD45 expression were measured with flow cytometry. Complete remission (CR), event-free survival (EFS) and overall survival (OS) were evaluated. The median follow-up duration was 15.0 (range 2.0–36.0) months.
RESULTS:
CD45 high expression (CD45) was associated with higher risk stratification in elderly AML patients ( 0.021). The percentage of CD45 cases in CR patients was 16.4%, which was lower compared to non-CR patients (35.2%, 0.017), while no difference in percentage of CD45 cases was found between allogeneic hematopoietic stem cell transplantation (allo-HSCT) patients and non-allo-HSCT patients (16.7% vs. 25.7%, 0.492). As to survival profiles, median EFS in CD45 patients was 6.0 (95% CI: 2.9–9.1) months, which was shorter than that in CD45 low expression (CD45) patients (10.0 (95% CI: 7.2–12.8) months) ( 0.002), and OS in CD45 patients was 16.0 (95% CI: 13.4–18.6) months, which was worse compared to CD45 patients (22.0 (95% CI: 17.0–27.0) months) ( 0.010). In subgroup analysis, no difference of EFS and OS was found between CD45 patients and CD45 patients in favorable, intermediate or adverse risk subgroups.
CONCLUSIONS:
CD45 correlates with adverse risk stratification, decreased treatment response and unfavorable survival profiles in elderly AML patients.
Acute myeloid leukemia (AML), originating from the proliferative, clonal, abnormally differentiated or occasionally poorly differentiated cells penetrating into the bone marrow, blood and other tissues, is the most common type of leukemia in adult, which is characterized by fatal infection, bleeding or organ infiltration and so on [1, 2]. There are approximately 11,900 adults diagnosed as AML every year in United States, among which more than two-thirds of these cases are over sixty years old [3, 4]. Although many advances have been obtained in treatment for AML patients benefiting from the individual or high-dose chemotherapy and allogeneic hematopoietic stem cell transplantation (allo-HSCT), the prognosis of elderly AML patients still remains poor with just 6% two-year survival due to increased comorbidities, severe physiological impairments or decreased tolerance to chemotherapies [3, 5]. Hence, the exploration of novel and convincing biomarkers in elderly AML patients is imperative to improve prognosis.
Increasing evidences have revealed that understanding of prognostic markers for AML would promote prevention of aggressive disease or treatment outcomes at early-stage disease [6, 7]. Cluster of differentiation 45 (CD45), also known as leukocyte common antigen, is one of the most abundant cell surface glycoproteins with molecular weight of 180 220 kDa [8]. Recent decades, CD45 has been reported to play an important role in disease progression of AML [9, 10]. However, little is known about the correlation of CD45 with clinical features and its effect on treatment outcomes in elderly AML patients. Thus, we conducted this prospective cohort study to explore the correlation of CD45 expression with clinicopathological features as well as prognosis in elderly AML patients.
Methods
Patients
One hundred and twenty one elderly patients with de novo AML who were treated at Department of Hematology, The Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology between Aug 2014 and Jul 2017 were consecutively recruited in this prospective cohort study. The inclusion criteria were as follows: (1) Newly diagnosed as AML according to World Health Organization (WHO) Classification of Tumors of Hematopoietic and Lymphoid Tissues (2008) and confirmed by morphology, immunology, cytogenetics and molecular biology (MICM) examination; (2) Age 60 years; (3) Able to be followed up regularly. Patients were excluded if they: (1) were diagnosed as acute promyelocytic leukemia; (2) complicated with other hematological diseases such as hemophilia, myelofibrosis, autoimmune hemolytic anemia and so on; (3) previously received radiotherapy, chemotherapy or allogeneic stem cell transplantation for other diseases; (4) had a history of serious infection, autoimmune disease or other malignant tumors.
Ethics
All participants provided written informed consents. The study protocol was approved by the Ethics Committee of The Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology and performed in accordance with the Declaration of Helsinki.
Data collection
Baseline characteristics of all patients were collected after enrollment including age, gender, French-American-British (FAB) classification (according to FAB classification system), Cytogenetics (according to An International System for Human Cytogenetic Nomenclature (ISCN 2009)), internal tandem duplications in the FMS-like tyrosine kinase 3 (FLT3-ITD) mutational status, isolated biallelic CCAAT/enhancerbinding protein (CEBPA) mutational status, nucleophosmin (NPM1) and risk stratification. The risk status based on validated cytogenetics and molecular abnormalities were classified as: favorable risk, intermediate risk and adverse risk according to National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology of AML (Version 2.2013). Moreover, white blood cell (WBC) counts were recorded in detail as well.
Sample collection and flow cytometric measurement
Bone marrow (BM) samples were collected from all patients prior to the initiation of treatment and BM mononuclear cells were isolated by Ficoll-Hypaque density gradient centrifugation within 24 hours. Then samples were washed and stained with fluorochrome-conjugated antigen-specific monoclonal antibodies. After washing procedure, samples were resuspended in PBS. Afterwards, CD45 antigen expressions were measured with flow cytometry (Becton Dickinson, San Jose, California, USA) and analyzed by CellQuest (Becton Dickinson, San Jose, CA, USA) software, which were performed according to the European Group for the Immunological Characterization of Leukemias (EGIL), and CD45 antigen expressions were quantified in terms of percentage of positive cells as compared to negative controls with isotype- and fluorochrome-matched antibodies. In order to control for technical variation, the CD45 expression values were normalized by using of residual normal lymphocytes in the same samples as internal standards, resulting that the expression values were described as relative ratios of CD45 expressions in leukemic versus normal cells in percentages. Moreover, elderly AML patients were classified as patients with CD45 high expression (CD45) ( 30) and patients with CD45 low expression (CD45) ( 91) according to the 75 percentile of CD45 expression as the methods reported previously [11].
Treatment and follow up
After diagnoses established, patients received induction chemotherapy regimens (DCAG, IA, DA or MA) according to disease conditions and risk stratifications, which were given as follows: (1) DCAG: Decitabine 15 mg/m/d (days 1–5), Ara-C 10 mg/m/d (days 3–9), aclacinomycin 8 mg/m/d (days 3–6), G-CSF 300 g/d from day 1; (2) IA, Idarubicin 8–12 mg/m/d (days 1–3), Ara-C 100 mg/m/d (days 1–7); (3) DA, Daunorubicin 40 60 mg/m/d (days 1–3), Ara-C 100 mg/m/d (days 1–7); (4) MA: Mitoxantrone 6 8 mg/m/d (days 1–3), Ara-C 100 mg/m/d (days 1–7). During 21–28 days after the accomplishment of induction chemotherapy, BM aspirate/biopsy and blood test were performed to monitor blasts percentage of residual cellularity. For patients achieved complete remission (CR), consolidation therapies were given, and if patients were deemed as strong candidates for hematopoietic stem cell transplantation (HSCT) and had available donors, HSCTs were used. As for patients with the reduction of BM blasts less than 60%, they were treated as induction failures and other regimens and/or best supportive cares were given, while for patients who did not achieve CR but with the reduction of BM blasts more than 60%, original regimens were repeated. In addition, patients with hypoplasia were suggested to await recovery if their residual BM blasts were less than 10%, and the patients with hypoplasia and residual BM blasts more than 10% were treated as induction failures and other regimens and/or best supportive cares were given as well. Furthermore, all patients were followed up regularly. The median follow-up duration was 15.0 months (range 2.0–36.0 months), and the last follow-up date was July 30 2017.
Definitions
According to the recommendations of European Leukemia Net (ELN) guidelines [12], CR, event-free survival (EFS) and overall survival (OS) were defined as follows: (1) CR: BM blasts 5%; absence of blasts with Auer rods; absence of extramedullary disease; absolute neutrophil count 1.0 10/L (1000/L); platelet count 100 10/L (100000/L); independence of red cell transfusions. (2) EFS: measured from the date of entry into the study to the date of recurrence, progression or death from any cause. (3) OS: measured from the date of entry into the study to the date of death from any cause.
Statistics
Statistical analysis was performed using SPSS 22.0 software (IBM, USA) and Graphs were drawn by Graphpad Prism 6.01 software (GraphPad Software Inc, USA). Data was mainly presented as mean value standard deviation, median value (1/4–3/4 quartiles) or count (percentage). Comparison was determined by Chi-square test, Kruskal-Wallis rank sum test. Kaplan-Meier (K-M) curves were applied to display EFS and OS. Log rank test was used to compare EFS and OS between/among different groups. In addition, univariate and multivariate Cox’s proportional hazards regression were used to analyze factors affecting EFS and OS. value 0.05 was considered significant.
Baseline characteristics of elderly AML patients
Elderly AML patients
( 121)
Age (years)
66.8 4.1
Gender (male/female)
67/54
FAB classification (n/%)
M1
8 (6.6)
M2
44 (36.4)
M4
24 (19.8)
M5
35 (28.9)
M6
10 (8.3)
Cytogenetics (n/%)
t(9;11)
1 (0.8)
5 or 5q-
2 (1.7)
t(9;22)
2 (1.7)
7 or 7q-
4 (3.3)
8
4 (3.3)
inv(16) or t(16;16)
5 (4.1)
t(8;21)
7 (5.8)
11q23
8 (6.6)
CK
14 (11.6)
Others (not included in favorable
14 (11.6)
or adverse risk)
NK
60 (49.6)
Monosomal karyotype (n/%)
12 (9.9)
FLT3-ITD mutation (n/%)
35 (28.9)
Isolated biallelic CEBPA mutation (n/%)
17 (14.0)
NPM1 (n/%)
46 (38.0)
Risk stratification (n/%)
Favorable risk
25 (20.7)
Intermediate risk
38 (31.4)
Adverse risk
58 (47.9)
WBC ( 10 cell/L)
16.220 (8.504–32.656)
Data were presented as mean value standard deviation, median value (1/4–3/4 quartiles) or count (percentage). AML, acute myeloid leukemia; FAB classification, French-American-British classification system; CK, complex karyotype; NK, normal karyotype; FLT3-ITD, internal tandem duplications in the FMS-like tyrosine kinase 3; CEBPA, CCAAT/enhancerbinding protein ; NPM1, nucleophosmin; WBC, white blood cell.
Results
Baseline characteristics
One hundred and twenty one elderly AML patients with mean age of 66.8 4.1 years were enrolled, and there were 67 males and 54 females (Table 1). According to FAB classification, the numbers of patients with M1, M2, M4, M5 and M6 were 8 (6.6%), 44 (36.4%), 24 (19.8%), 35 (28.9%) and 10 (8.3%) respectively. In addition, 12 (9.9%), 35 (28.9%), 17 (14.0%) and 46 (38.0%) patients were with monosomal karyotype, FLT3-ITD mutation, isolated biallelic CEBPA mutation and NPM1 respectively. As to risk stratification, there were 25 (20.7%), 38 (31.4%) and 58 (47.9%) patients categorized as favorable risk, intermediate risk and adverse risk. Median value of WBC in all patients was 16.220 (8.504–32.656) 10 cell/L. Other detailed baseline characteristics were shown in Table 1.
Correlations of CD45 with clinicopathological features in elderly AML patients
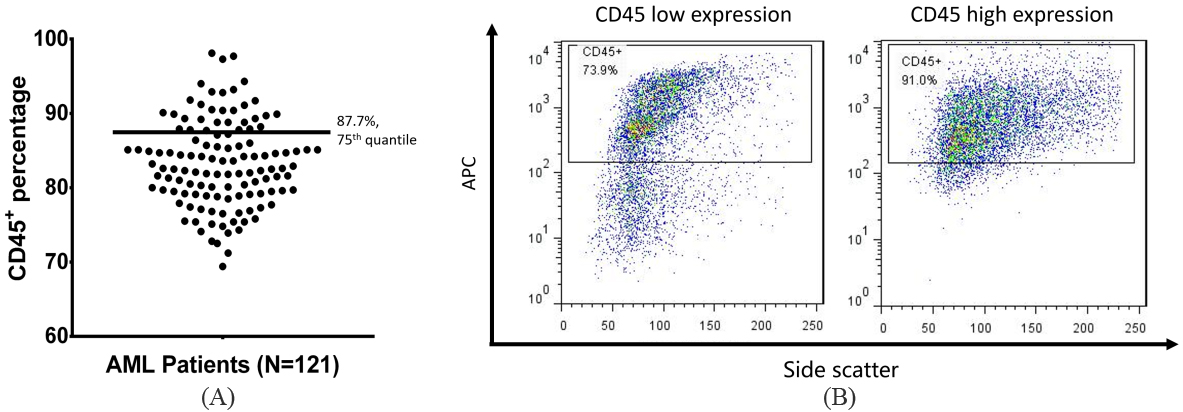
The median percentage of CD45 positive cells was 82.6% (range: 69.4%–98.1%, 25–75: 79.2%–87.7%) (Supplementary Fig. 1A and B), and patients were classified into CD45 group and CD45 group with cut-off value at 75 percentile of CD45 expression in total patients. As shown in Table 2, CD45 was associated with higher risk stratification ( 0.021), while no difference in other clinicopathological features including age ( 0.557), gender ( 0.796), FAB classification ( 0.620) and WBC ( 0.192) was found between CD45 patients and CD45 patients.
Correlation of CD45 with clinicopathological features of elderly AML patients
Items
No. of
CD45
CD45
value
patients
( 30)
( 91)
Age (n/%)
66 years
67
18 (26.9)
49 (73.1)
0.557
66 years
54
12 (22.2)
42 (77.8)
Gender (n/%)
0.796
Male
67
16 (23.9)
51 (76.1)
Female
54
14 (25.9)
40 (74.1)
FAB classification (n/%)
0.620
M1
8
2 (25.0)
6 (75.0)
M2
44
13 (29.5)
31 (70.5)
M4
24
3 (12.5)
21 (87.5)
M5
35
9 (25.7)
26 (74.3)
M6
10
3 (30.0)
7 (70.0)
Risk stratification (n/%)
0.021
Favorable risk
25
2 (8.0)
23 (92.0)
Intermediate risk
38
9 (23.7)
29 (76.3)
Adverse risk
58
19 (32.8)
39 (67.2)
WBC (n/%)
0.192
10 ( 10 cell/L)
81
23 (28.4)
58 (71.6)
10 ( 10 cell/L)
40
7 (17.5)
33 (82.5)
Data were presented as count (percentage). Comparison was determined by Chi-square test or Kruskal-Wallis rank sum test. 0.05 was considered significant. As a cut-off to distinguish the CD45 from CD45, the 75 percentile was used. AML, acute myeloid leukemia; FAB classification, French-American-British classification systems; WBC, white blood cell.
Correlation of CD45 with treatment response and allo-HSCT realization
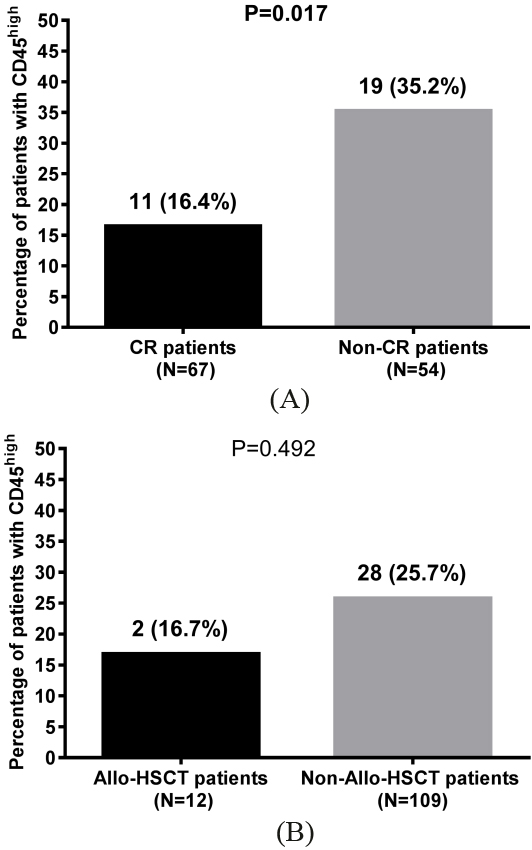
As displayed in Fig. 1A, 67 elderly AML patients achieved CR and 54 patients failed to achieve CR. Percentage of CD45 cases was 16.4% ( 11) in CR patients, which was decreased than that in non-CR patients (35.2% ( 19)) ( 0.017). Furthermore, there were 12 patients received allo-HSCT while 109 patients did not (Fig. 1B). No difference in percentage of CD45 patients was found between allo-HSCT group (16.7% ( 2)) and non-allo-HSCT group (25.7% ( 28)) ( 0.492). As to the information of allo-HSCT, 3 cases received fludarabine/ busulfan, 3 cases received fludarabine/busulfan/total-body irradiation, 2 cases received fludarabine/busulfan/ antihuman T-lymphocyte immunoglobulin, 2 cases received cladribine/busulfan and 2 cases received cladribine/busulfan/total-body irradiation as conditioning regimens. Average age of donors were 36.5 9.7 years with 8 males and 4 females, and 3 patients underwent HLA-matched allo-HSCT while the remaining 9 patients underwent HLA-mismatched allo-HSCT.
Comparison of CD45 percentage between CR and non-CR patients, allo-HSCT and non-allo-HSCT patients. Percentage of CD45 patients in CR group was decreased than that in non-CR group (A). Furthermore, no difference of percentage of CD45 patients was found between allo-HSCT group and non-allo-HSCT group (B). Chi-square test was applied to compare difference of CD45 patients percentage between different groups. CR, complete remission; allo-HSCT, allogeneic hematopoietic stem cell transplantation. 0.05 was considered significant.
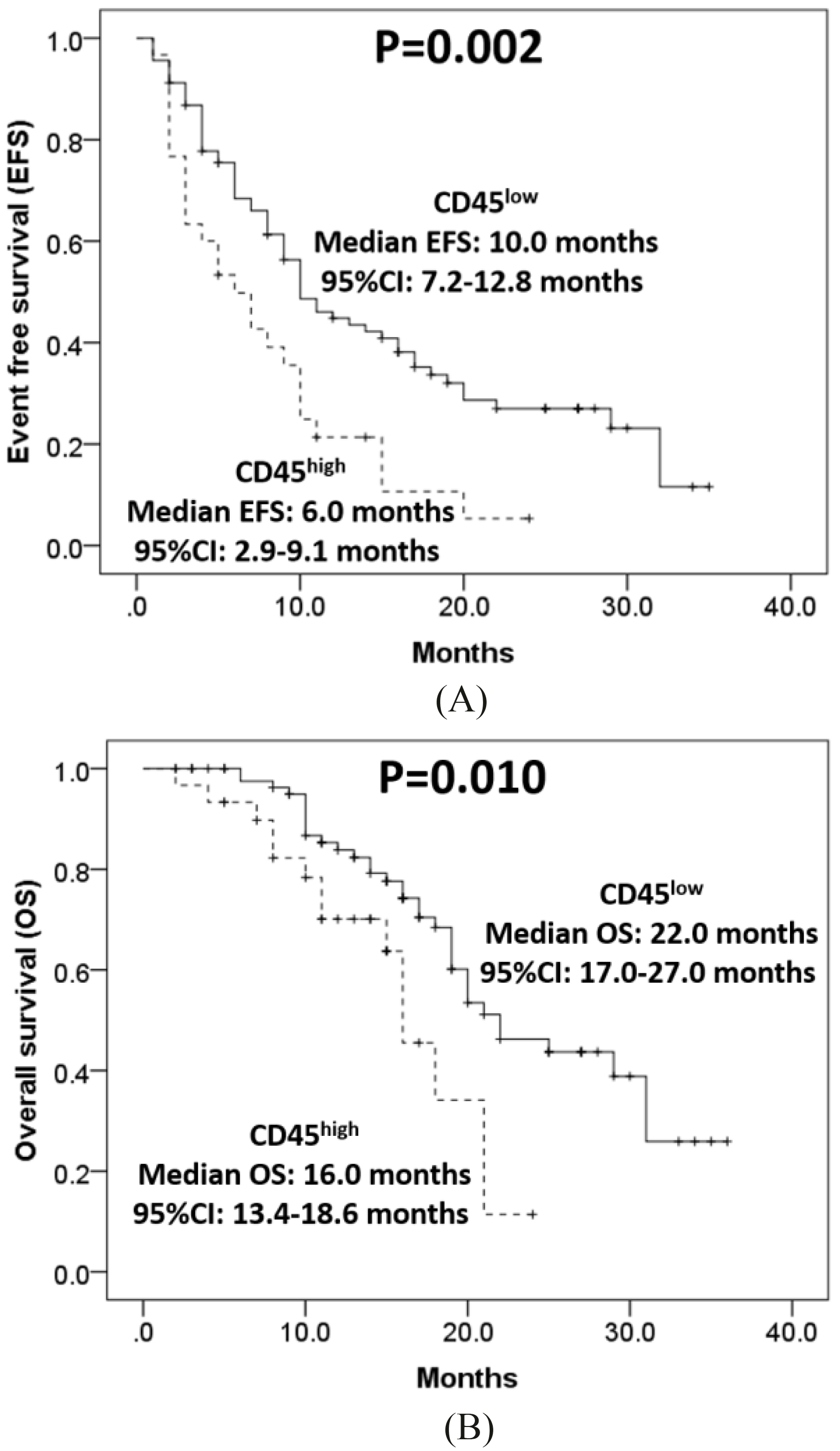
Comparison of EFS and OS between CD45 and CD45 patients. Mean EFS of CD45 patients was shorter than that in CD45 patients (A). Besides, mean OS in CD45 patients was decreased than that in CD45 patients (B). K-M curve was used to exhibit EFS and OS. Log-rank test was conducted to compare difference of EFS and OS between different groups. EFS, event-free survival; OS, overall survival. 0.05 was considered significant.
Survival profiles between CD45 and CD45 elderly AML patients
Comparison of EFS and OS between CD45 patients and CD45 patients were performed in Fig. 2. The median EFS was 6.0 (95% CI: 2.9–9.1) months in CD45 AML patients, which was worse than that in CD45 AML patients (10.0 (95% CI: 7.2–12.8) months) ( 0.002) (Fig. 2A). Besides, median OS in CD45 patients was 16.0 (95% CI: 13.4–18.6) months, which was also shorter compared with CD45 patients (22.0 (95% CI: 17.0–27.0) months) ( 0.010) (Fig. 2B).
Cox’s proportional hazards regression model analysis of factors affecting EFS
Parameters
Univariate Cox’s regression
Multivariate Cox’s regression
value
HR
95% CI
value
HR
95% CI
Lower
Higher
Lower
Higher
CD45
0.004
1.984
1.243
3.167
0.478
1.190
0.736
1.927
Age ( 66 years)
0.204
1.319
0.861
2.023
0.388
1.211
0.784
1.869
Gender (male)
0.473
1.169
0.763
1.790
0.783
1.064
0.684
1.657
Adverse risk stratification
0.001
3.030
2.153
4.266
0.001
3.792
2.606
5.519
WBC 10 ( 10 cell/L)
0.001
2.235
1.393
3.584
0.001
3.680
2.219
6.101
Data were presented as value, HR (hazards ratio) and 95% CI (confidence interval). 0.05 was considered significant (in bold). Risk stratification was scored as 0-favorable risk, 1-intermediate risk, 2-adverse risk. EFS, event free survival; WBC, white blood cell.
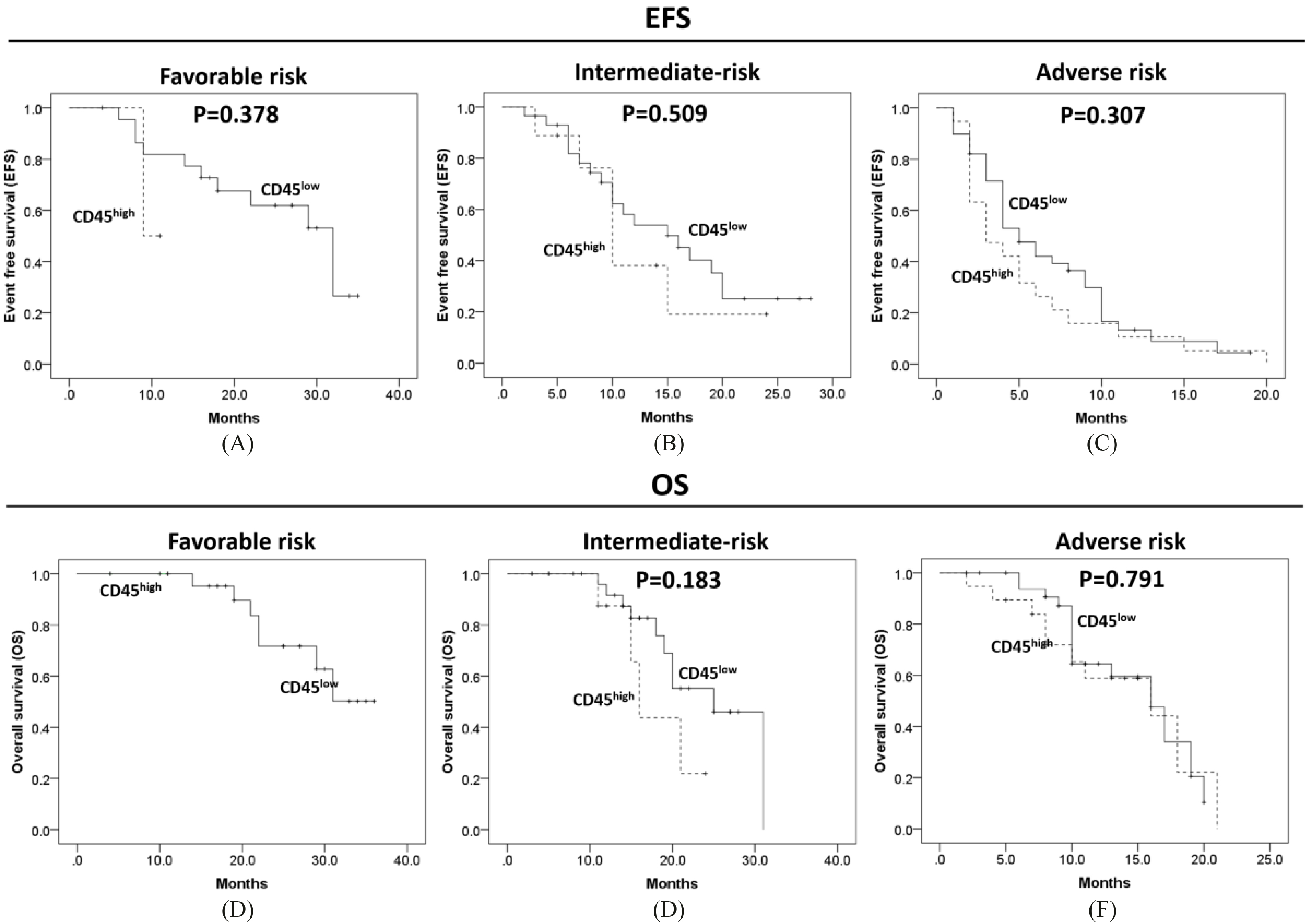
Subgroup analysis of EFS and OS in CD45 and CD45 AML patients. No difference of EFS was observed between CD45 elderly AML patients and CD45 elderly AML patients in subgroup of favorable risk (A), intermediate risk (B) and adverse risk (C). In addition, no difference of OS was found between patients with CD45 and patients with CD45 in intermediate risk group (E) as well as adverse risk group (F). Furthermore, statistics could not be performed in favorable risk subgroup due to lack of CD45 patients ( 2) (D). K-M curve was used to exhibit EFS and OS. Log-rank test was conducted to compare difference of EFS and OS between different groups. EFS, event-free survival; OS, overall survival. 0.05 was considered significant.
Subgroup analysis of survival profiles between CD45 and CD45 elderly AML patients
All patients were divided into different subgroups according to risk stratification (Fig. 3). No difference of EFS was found between CD45 elderly AML patients and CD45 elderly AML patients in favorable risk subgroup (Fig. 3A, 0.378), intermediate risk subgroup (Fig. 3B, 0.509) and adverse risk subgroup (Fig. 3C, 0.307). In addition, no difference of OS was observed between CD45 patients and CD45 patients in intermediate risk subgroup (Fig. 3E, 0.183) and adverse risk subgroup (Fig. 3F, 0.719) as well, while statistics could not be performed in favorable risk subgroup due to lack of CD45 patients ( 2).
Cox’s proportional hazards regression model analysis of factors affecting OS
Parameters
Univariate Cox’s regression
Multivariate Cox’s regression
value
HR
95% CI
value
HR
95% CI
Lower
Higher
Lower
Higher
CD45
0.014
2.262
1.184
4.322
0.654
1.167
0.595
2.286
Age ( 66 years)
0.249
1.399
0.790
2.477
0.559
1.189
0.665
2.128
Gender (male)
0.816
1.069
0.608
1.880
0.928
1.027
0.575
1.835
Adverse risk stratification
0.001
3.461
2.154
5.561
0.001
3.458
2.120
5.641
WBC 10 ( 10 cell/L)
0.095
1.683
0.913
3.103
0.040
1.944
1.029
3.670
Data were presented as value, HR (hazards ratio) and 95% CI (confidence interval). 0.05 was considered significant (in bold). Risk stratification was scored as 0-favorable risk, 1-intermediate risk, 2-adverse risk. OS, overall survival; WBC, white blood cell.
Analysis of factors affecting EFS and OS by Cox’s model
Univariate Cox’s proportional hazards regression revealed that CD45 correlated with worse EFS (Table 3, 0.004) and OS (Table 4, 0.014), while further multivariate Cox’s proportional hazards regression disclosed that CD45 was not independent predictive factor for shorter EFS ( 0.478) or OS ( 0.654), while adverse risk as well as WBC were independently correlated with worse EFS and OS. Combining the fact that CD45 correlated with adverse risk stratification, we speculated that CD45 might affect the survival profiles through its association with adverse risk.
Discussion
In this study, we found that: (1) CD45 high expression was correlated with adverse risk stratification in elderly AML patients; (2) CD45 high expression was associated with decreased CR achievement, shorter EFS as well as OS in elderly AML patients.
CD45, a tyrosine phosphatase, is a cell surface antigen being expressed on nucleated hematopoietic cells that plays a central role in regulating cellular signal transductions in hematopoietic processes [13, 14]. A larger number of studies have been conducted to explore the role of CD45 in AML [8, 15, 16, 17]. For example, an interesting study indicates that CD45, severing as a hematopoietic JAK phosphatase, negatively regulates certain cytokine receptor activation that is involved in the differentiation, proliferation and antiviral immunity of hematopoietic cells [15]. In addition, CD45 binds with Lyn (Src family) on its tyrosine inhibitory site (Y507) and further activates granulocyte/macrophage colony-stimulating factor (GM-CSF) related anti-apoptotic signal pathways in AML [15, 18, 19, 20]. Furthermore, several studies reveal that elevated CD45 expression is associated with interleukin (IL)-6-induced proliferation of myeloma cells through activation of signal transducer such as activator of transcription 3 (STAT 3) and mitogen-activated protein kinase (MAPK) [8, 21]. Therefore, these previous studies suggest that CD45 plays a crucial role in AML development and progression.
In the meanwhile, some clinical studies investigating the correlation of CD45 expression with clinicopathological features in several types of leukemia have been disclosed as well [22, 23, 24]. For instance, CD45 expression has been reported to be associated with continuous progression in chronic lymphocytic leukemia (CLL) patients [22]. Another study reveals that CD45 expression is correlated with the presence of trisomy 12 in CLL patients [23]. In addition, CD45 expression is also observed to be correlated with trisomy 8 presence in Philadelphia-positive B-cell precursor acute lymphoblastic leukemia (BCP-ALL) patients [24]. Although the correlation between CD45 expression and clinicopathological features in several types of leukemia have been explored, little is known about the role of CD45 in elderly AML patients. In the present study, we found that CD45 expression was correlated with adverse risk stratification in elderly AML patients. The possible reason was that CD45 high expression might increase the acquisition of some cytogenetic mutations such as FLT3-ITD mutation and chromosomal translocation (6;9) (p23; q34), thereby contributed to adverse risk stratification in elderly AML [25, 26].
As to the effect of CD45 on prognosis in AML patients, several studies have been carried out [26, 27, 28]. An interesting study explores predictive value of several pre-therapeutic parameters in AML patients, which discloses that elevated CD45 expression is associated with lower percentage of 5-year survival [27]. Another study investigates immunophenotypic aberrations in NPM mutation AML patients with age up to 70 years, which discloses that upregulation of CD45 is associated with shorter OS [26]. A case report also reveals that a 62-year old AML patient with positive CD45 expression fails to remission after chemotherapy and develops myeloid sarcoma, which is an extramedullary malignancy usually occurring in AML patients [28]. These previous studies suggest that CD45 acts as an unfavorable role in the prognosis of AML patients, however, detailed information about the predictive value of CD45 for treatment response and survival profiles in elderly AML patients is still unclear. In this study, we found that CD45 high expression correlated with lower CR achievement and it was associated with worse EFS and OS in elderly AML patients. The possible reasons were as follows: (1) CD45 regulated several kinases (including Lyn, STAT 3 and MAPK) or interacted with some molecules (including galectin or IL-6) to induce proliferation of leukemia cells, thereby increased recurrence and caused poor prognosis in elderly AML patients [8, 16, 21, 29]. (2) CD45 might correlate with overexpression of several multidrug transporter genes (such as genes for multidrug resistance associated protein 1 (MRP-1) or P-glycoprotein (P-gp)), thereby resulted in severe resistance to treatment and caused worse prognosis in elderly AML patients [26, 30].
There were still some limitations in our study: (1) sample size of 121 was relatively small, thus the statistical efficacy might be poor; (2) this study was a cohort study without any interference, and all patients were from a signal center; (3) follow-up duration of 15.0 months (range 2.0–36.0 months) was relatively short, thus, long-term effect of CD45 on prognosis in elderly AML patients was not investigated. Thus further multi-center study with larger sample size and long-term follow-up duration is needed; (4) minimal residual disease (MRD), as an important prognostic factor, was not included in the analysis in this study due to only less than 40% patients had MRD status data.
In conclusion, CD45 correlates with adverse risk stratification, decreased treatment response and unfavorable survival profiles in elderly AML patients.
Footnotes
Conflict of interest
No potential conflict of interest was reported by the authors.
Supplementary data
Expressions of CD45 in elderly AML patients. (A) presented the plot distribution of CD45 percentage by flow cytometry; (B) showed examples of low expression and high expression results of CD45 by flow cytometry.
References
1.
DohnerH.WeisdorfD.J. and BloomfieldC.D., Acute myeloid leukemia, N Engl J Med373 (2015), 1136–52.
2.
EsteyE. and DohnerH., Acute myeloid leukaemia, Lancet368 (2006), 1894–907.
3.
CraigC.M. and SchillerG.J., Acute myeloid leukemia in the elderly: Conventional and novel treatment approaches, Blood Rev22 (2008), 221–34.
4.
RiesL.G.MelbertD.KrapchoM.StinchcombD.G.HowladerN.HornerM.MariottoA.MillerB.FeuerE.AltekruseS.LewisD.CleggL.EisnerM.ReichmanM. and EdwardsB., SEER Cancer Statistics Review, 1975–2004, National Cancer Institute. Bethesda, MD, USA, http://seer.cancer.gov/csr/1975_2004/, based on November 2006 SEER data submission, posted to the SEER web site, 2007.
5.
MenzinJ.LangK.EarleC.C.KerneyD. and MallickR., The outcomes and costs of acute myeloid leukemia among the elderly, Arch Intern Med162 (2002), 1597–603.
6.
CountouriotisA.MooreT.B. and SakamotoK.M., Cell surface antigen and molecular targeting in the treatment of hematologic malignancies, Stem Cells20 (2002), 215–29.
7.
WeidmannE.HinzT.KleinS.SchuiD.K.HarderS.KrienerS.KabelitzD.HoelzerD. and MitrouP.S., Cytotoxic hepatosplenic gammadelta T-cell lymphoma following acute myeloid leukemia bearing two distinct gamma chains of the T-cell receptor. Biologic and clinical features, Haematologica85 (2000), 1024–31.
8.
HermistonM.L.XuZ. and WeissA., CD45: A critical regulator of signaling thresholds in immune cells, Annu Rev Immunol21 (2003), 107–37.
9.
PagelJ.M.GooleyT.A.RajendranJ.FisherD.R.WilsonW.A.SandmaierB.M.MatthewsD.C.DeegH.J.GopalA.K.MartinP.J.StorbR.F.PressO.W. and AppelbaumF.R., Allogeneic hematopoietic cell transplantation after conditioning with 131I-anti-CD45 antibody plus fludarabine and low-dose total body irradiation for elderly patients with advanced acute myeloid leukemia or high-risk myelodysplastic syndrome, Blood114 (2009), 5444–53.
10.
BuckleyS.A. and WalterR.B., Antigen-specific immunotherapies for acute myeloid leukemia, Hematology Am Soc Hematol Educ Program2015 (2015), 584–95.
11.
RateiR.SchabathR.KarawajewL.ZimmermannM.MorickeA.SchrappeM. and LudwigW.D., Lineage classification of childhood acute lymphoblastic leukemia according to the EGIL recommendations: Results of the ALL-BFM 2000 trial, Klin Padiatr225(Suppl 1) (2013), S34–9.
12.
DohnerH.EsteyE.H.AmadoriS.AppelbaumF.R.BuchnerT.BurnettA.K.DombretH.FenauxP.GrimwadeD.LarsonR.A.Lo-CocoF.NaoeT.NiederwieserD.OssenkoppeleG.J.SanzM.A.SierraJ.TallmanM.S.LowenbergB.BloomfieldC.D. and EuropeanL., Diagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNet, Blood115 (2010), 453–74.
13.
WalterR.B.BoyleK.M.AppelbaumF.R.BernsteinI.D. and PagelJ.M., Simultaneously targeting CD45 significantly increases cytotoxicity of the anti-CD33 immunoconjugate, gemtuzumab ozogamicin, against acute myeloid leukemia (AML) cells and improves survival of mice bearing human AML xenografts, Blood111 (2008), 4813–6.
14.
OrozcoJ.J.BäckT.KenoyerA.BalkinE.R.HamlinD.K.WilburD.S.FisherD.R.FrayoS.L.HylaridesM.D.GreenD.J.GopalA.K.PressO.W. and PagelJ.M., Anti-CD45 radioimmunotherapy using (211)At with bone marrow transplantation prolongs survival in a disseminated murine leukemia model, Blood121 (2013), 3759–67.
15.
Irie-SasakiJ.SasakiT.MatsumotoW.OpavskyA.ChengM.WelsteadG.GriffithsE.KrawczykC.RichardsonC.D.AitkenK.IscoveN.KoretzkyG.JohnsonP.LiuP.RothsteinD.M. and PenningerJ.M., CD45 is a JAK phosphatase and negatively regulates cytokine receptor signalling, Nature409 (2001), 349–54.
16.
FaderlS.HarrisD.VanQ.KantarjianH.M.TalpazM. and EstrovZ., Granulocyte-macrophage colony-stimulating factor (GM-CSF) induces antiapoptotic and proapoptotic signals in acute myeloid leukemia, Blood102 (2003), 630–7.
17.
Saint-PaulL.NguyenC.H.BuffiereA.Pais de BarrosJ.P.HammannA.Landras-GuettaC.FilomenkoR.ChretienM.L.JohnsonP.BastieJ.N.DelvaL. and QuereR., CD45 phosphatase is crucial for human and murine acute myeloid leukemia maintenance through its localization in lipid rafts, Oncotarget7 (2016), 64785–64797.
18.
HibbsM.L. and HarderK.W., The duplicitous nature of the Lyn tyrosine kinase in growth factor signaling, Growth Factors24 (2006), 137–49.
19.
ScapiniP.PereiraS.ZhangH. and LowellC.A., Multiple roles of Lyn kinase in myeloid cell signaling and function, Immunol Rev228 (2009), 23–40.
20.
WeiS.LiuJ.H.Epling-BurnetteP.K.GameroA.M.UsseryD.PearsonE.W.ElkabaniM.E.DiazJ.I. and DjeuJ.Y., Critical role of Lyn kinase in inhibition of neutrophil apoptosis by granulocyte-macrophage colony-stimulating factor, J Immunol157 (1996), 5155–62.
21.
BatailleR.RobillardN.Pellat-DeceunynckC. and AmiotM., A cellular model for myeloma cell growth and maturation based on an intraclonal CD45 hierarchy, Immunol Rev194 (2003), 105–11.
22.
HuangP.Y.BestO.G.AlmaziJ.G.BelovL.DavisZ.A.MajidA.DyerM.J.PascoviciD.MulliganS.P. and ChristophersonR.I., Cell surface phenotype profiles distinguish stable and progressive chronic lymphocytic leukemia, Leuk Lymphoma55 (2014), 2085–92.
23.
RizzoD.LotayA.GachardN.MarfakI.FaucherJ.L.TrimoreauF.GuerinE.BordessouleD.JaccardA. and FeuillardJ., Very low levels of surface CD45 reflect CLL cell fragility, are inversely correlated with trisomy 12 and are associated with increased treatment-free survival, Am J Hematol88 (2013), 747–53.
24.
PrimoD.TaberneroM.D.PerezJ.J.RasilloA.SayaguesJ.M.EspinosaA.B.Lopez-BergesM.C.Garcia-SanzR.GutierrezN.C.HernandezJ.M.RomeroM.OsunaC.S.GiraltM.BarbonM.San MiguelJ.F. and OrfaoA., Genetic heterogeneity of BCR/ABL+ adult B-cell precursor acute lymphoblastic leukemia: Impact on the clinical, biological and immunophenotypical disease characteristics, Leukemia19 (2005), 713–20.
25.
ChiY.LindgrenV.QuigleyS. and GaitondeS., Acute myelogenous leukemia with t(6;9)(p23;q34) and marrow basophilia: An overview, Arch Pathol Lab Med132 (2008), 1835–7.
26.
NomdedeuJ.BussagliaE.VillamorN.MartinezC.EsteveJ.TormoM.EstivillC.QueipoM.P.GuardiaR.CarricondoM.HoyosM.LlorenteA.JuncaJ.GallartM.DomingoA.BargayJ.MascaroM.MoraledaJ.M.FlorensaL.RiberaJ.M.GallardoD.BrunetS.AventinA.SierraJ. and SpanishC., Immunophenotype of acute myeloid leukemia with NPM mutations: prognostic impact of the leukemic compartment size, Leuk Res35 (2011), 163–8.
27.
ValetG.ReppR.LinkH.EhningerA.GramatzkiM.M. and GroupS.-A.S., Pretherapeutic identification of high-risk acute myeloid leukemia (AML) patients from immunophenotypic, cytogenetic, and clinical parameters, Cytometry B Clin Cytom53 (2003), 4–10.
28.
ColellaG.TirelliA.CaponeR.RubiniC. and GuastafierroS., Myeloid sarcoma occurring in the maxillary gingiva: A case without leukemic manifestations, Int J Hematol81 (2005), 138–41.
29.
StillmanB.N.HsuD.K.PangM.BrewerC.F.JohnsonP.LiuF.T. and BaumL.G., Galectin-3 and galectin-1 bind distinct cell surface glycoprotein receptors to induce T cell death, J Immunol176 (2006), 778–89.
30.
de Figueiredo-PontesL.L.PintaoM.C.OliveiraL.C.DalmazzoL.F.JacomoR.H.GarciaA.B.FalcaoR.P. and RegoE.M., Determination of P-glycoprotein, MDR-related protein 1, breast cancer resistance protein, and lung-resistance protein expression in leukemic stem cells of acute myeloid leukemia, Cytometry B Clin Cytom74 (2008), 163–8.