In order to improve the understanding of granular cell tumor and avoid missing the best time of treatment, we report three patients with rare granular cell tumors admitted to our hospital in the past 10 years.
METHODS:
The characteristics, methods of treatment, postoperative pathological results and follow-up results of three cases of granular cell tumor were analyzed; and literatures related to granular cell tumors were reviewed.
RESULTS:
All patients underwent surgical treatment, and the excised lesions were sent to the laboratory for testing. Postoperative pathological results were as follows: granular cell tumor of the vulva, granular cell tumor within the sheath of the rectus muscle, and granular cell tumor in the left cubit nerve. All three cases were benign, and no recurrence was found during follow-ups after the operation.
CONCLUSION:
Granular cell tumors are rare tumors derived from the nerve sheath, are mostly benign tumors, and the incidence of malignancy is 2%. The gold standard for diagnosis of granular cell tumor is histopathology. Granular cell tumor is not sensitive to radiotherapy and chemotherapy, and needs to be surgically removed. Since this disease may have no solid lesions and tumor cells can infiltrate local tissues, based on the full excision of the lesion, the extent of resection may be extended to areas without infiltration. This disease has a possibility of recurrence, and patients need to be followed-up.
Granular cell tumor (GCT) is a rare benign soft tissue tumor, which can occur in any part of the body, and was described by Abrikossoff in 1926. It is also known as granular cell myoblastoma [1]. This disease is divided into three types, according to pathological morphology and clinical biological behavior: GCT, malignant granular cell tumor (MGCT), and atypical granular cell tumor (AGCT) [2]. The majority of GCTs occurs in the skin, submucosal and subcutaneous tissues of the head and neck, especially in the tongue and mouth [3, 4]; and approximately 10% occurs in the vulva. GCT most often occurs in women and black people. It can occur at all ages, and the peak of incidence appears at the age of 50 years old [5]. The vast majority of GCTs are benign, usually manifest as small, slow-growing, single and painless subcutaneous nodules; and the incidence of malignancy is 2% [6, 7, 8, 9]. The gold standard for the diagnosis of GCT is histopathology. In order to improve the understanding of GCT and avoid missing the best time for treatment, we report three patients with GCT, who were admitted in our hospital for the past 10 years. Among these patients, one patient had GCT at the vulva, one patient had GCT within the sheath of the rectus muscle, and one patient had GCT in the left cubit nerve. Literature was reviewed and cases are reported as follows.
Clinical data
Case 1
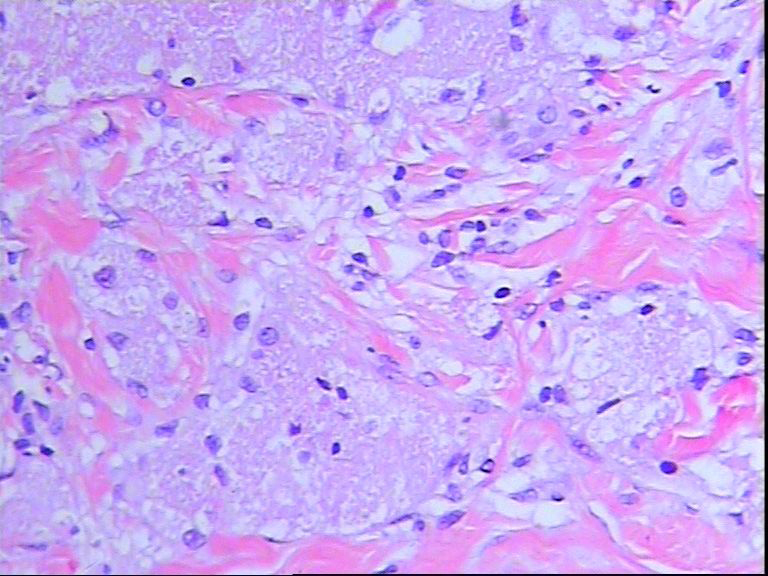
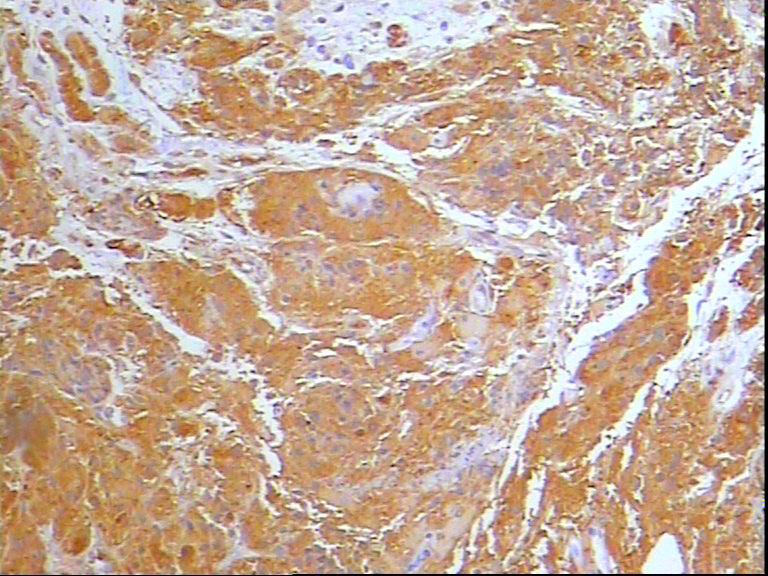
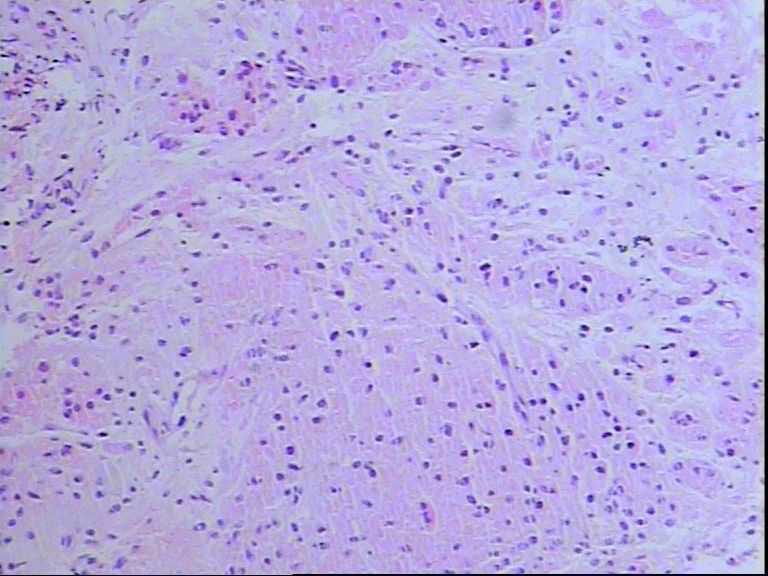
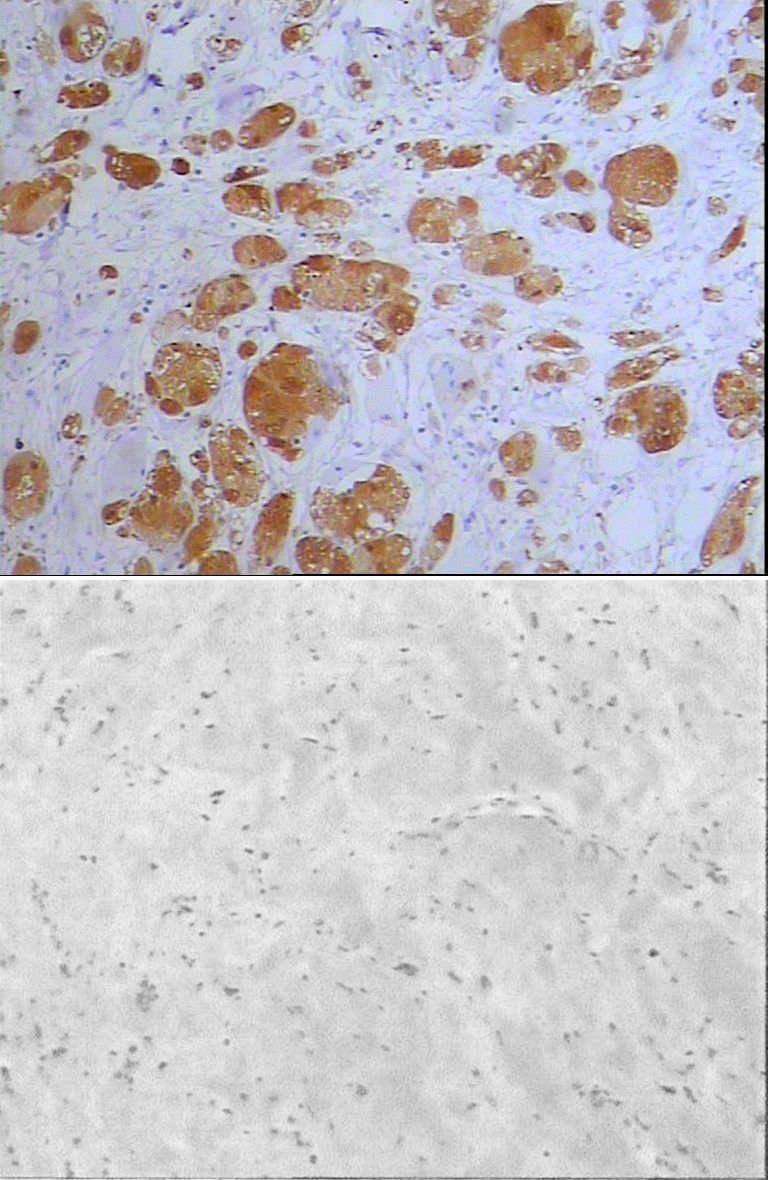
This patient was a 73-year old woman who presented with mass at the right side of the vulva for a year. The size of the mass was similar to a soybean, without tenderness and itching. Hence, the patients did not receive any treatment. In the last one year, the vulva mass gradually grew to the size of an apricot. Since the onset of the disease, patient had an acceptable mental status, normal diet and sleep, and had no loss of weight. Physical examination results: body temperature, 36C; pulse, 88 times/min, respiration, 18 times/min; blood pressure, 157/87 mmHg. General state was good, mental status was lucid, and languish expression was clear. The heart and lung revealed no abnormal murmur. The abdomen was soft, and there was no tenderness in the lower abdomen. Furthermore, the patient did not complain of muscle tension and rebound pain, and the liver and spleen could not be felt under the ribs. Neurological examination revealed a normal result. The limbs could freely move. Both lower limbs had no edema. Gynecological examination results: vulva development was normal, being the married parous type. A mass with a size of 1.5 2.5 cm could be touched on the right side of the greater lip of pudendum. The mass was oval and hard, had good activity, and was without tenderness. The vagina was normal, presenting with a moderate amount of white secretion. The cervix was hypertrophic, with medium texture and columnar shape. The cervical surface presented with erosion, the uterine body shrunk, and other abnormalities could not be felt. Preliminary clinical diagnosis: vulval mass, hypertension and chronic cervicitis. Routine laboratory examination revealed no abnormality. The mass on the right side of the vulva was resected under local anesthesia. A 2-cm incision was made on the skin above the vulva mass. During the operation, it was found that the boundary between the mass and surrounding tissues was unclear. The mass was hard, without an obvious capsule. The mass was separated and completely resected. The mass was cut off, found to be a yellow white solid mass with a tough texture. No bleeding was found. Then, the skin was sutured. Pathology of the mass: large and polygonal cells were observed under a microscope. The nuclei were small and deeply stained, and was located at the center of the cells. The cytoplasm of cells was rich in eosinophilic granules. Immunohistochemical markers were S-100 () and CD68 (). The above features are consistent with GCT. The pathological diagnosis was vulval GCT. No recurrence was found during the follow-ups after the operation.
Histological picture.
Immunohistochemical picture.
Case 2
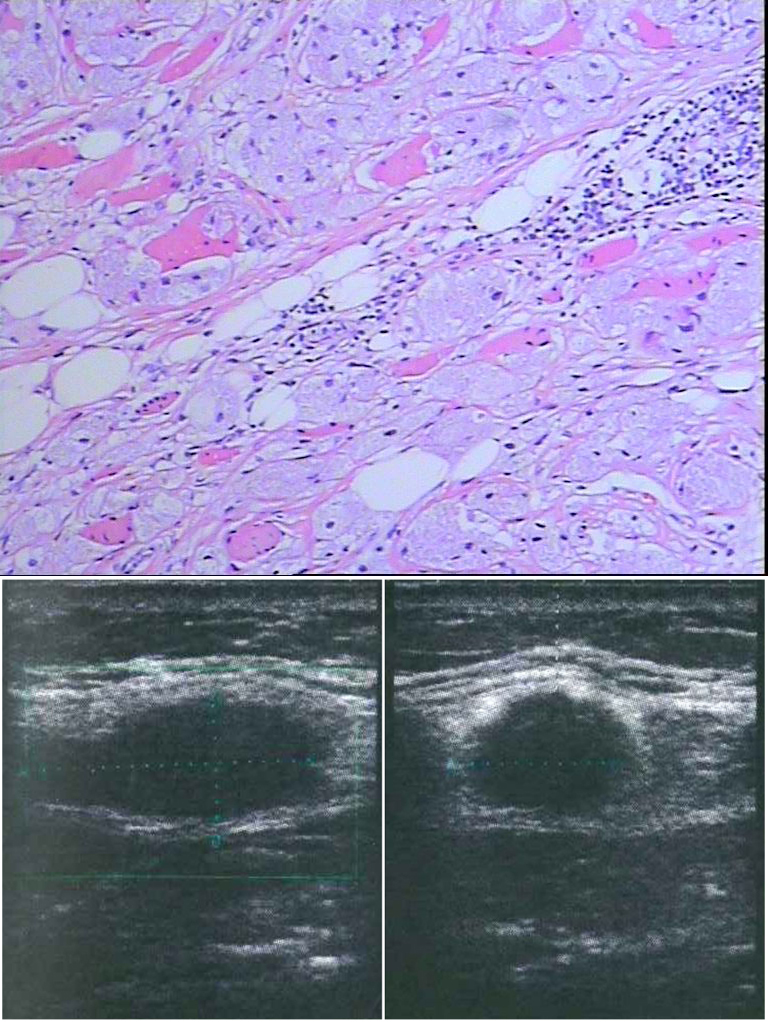
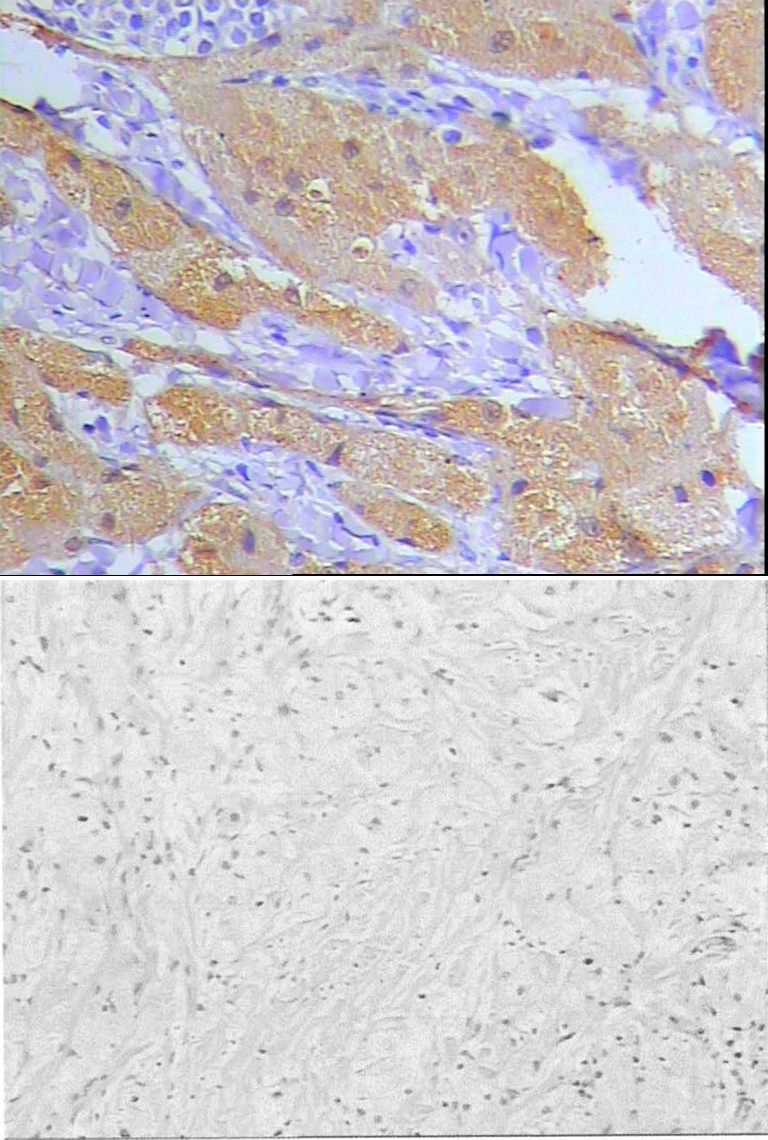
This patient was a 49-year old woman who presented with painless mass in the right abdominal wall for more than 40 days. This patient accidentally discovered a mass on her right abdominal wall more than 40 days ago, which had a pea-like size. No special treatments were given. The patient underwent computed tomography (CT) examination in another hospital and revealed a dense shadow of soft tissues on the right side of the sheath of rectus muscle. Color Doppler ultrasound revealed a solid mass in the abdominal wall, which was suspected as sarcoma. The mass felt hard, had poor activity, and was without tenderness. Furthermore, the patient had no abdominal distention, nausea, vomiting and fever, as well as defecation disorder. No redness was observed on the skin surface. The patient visited the General Surgical Department of our hospital for further diagnosis and treatment. The Outpatient Department admitted this patient based on a reason of “mass on the right abdominal wall”. Since its onset, the diseased patient had an acceptable mental status, a satisfactory diet and sleep, and had no loss of weight. Physical examination results: body temperature, 36.5C; pulse, 80 times/min; respiration, 20 times/min; blood pressure, 120/80 mmHg; no superficial lymph node enlargement was felt. The sounds of double lung breath were normal. Heart rate was 80 beats per minute with regular rhythm. The valve auscultation area presented with no pathological murmur. A mass with a size of 1.0 1.0 cm could be felt in the center of right rectus abdominis, was without tenderness, and had poor activity and hard texture. No redness and protrusions were observed on the skin surface. Surface temperature did not increase. Preliminary clinical diagnosis was a mass on the right abdominal wall. Routine laboratory examination revealed no abnormality. Resection of the right abdominal mass was performed under general anesthesia. A longitudinal incision was made in the center of the right rectus abdominis. The length of the incision was approximately 10 cm. The skin was cut off layer by layer to the surface of the rectus abdominis, and when the aponeurosis was cut off, the rectus abdominis and aponeurosis were separated. The mass was found in the middle segment of the rectus abdominis. The diameter was approximately 1.5 1.5 cm. The texture was hard with poor activity. The posterior rectus sheath was not affected. Muscles were cut off at the sites 2 cm from the upper and lower parts of the mass, and part of the aponeurosis was removed. A piece of gray red tissue was found during the operation. The volume was 7.5 3–4 0.5–1.5 cm, and a hard mass could be felt within it, which had a volume of 3.2 2.3 1.5 cm. Sections were gray yellow or gray white, with a tough texture. The boundaries were unclear. Intraoperative frozen test revealed a diagnosis of GCT. A small amount of muscles around the mass were removed, and a biological patch was implanted in the posterior sheath of anterior muscle, which was sutured and firmly fixed. A drainage tube was placed under the patch, and the anterior sheath was intermittently sutured, layer by layer. The mass was sent for pathological examination. Results under a microscope: tumor cells revealed a nest-like growth and infiltration, and most were large cells or polygonal cells with abundant cytoplasm. Nuclei were small and deeply stained, round or oval, located in the center of cells, and were surrounded by a large number of collagen fiber bundles. Postoperative pathological results were as follows: GCT (within the right rectus abdominis), and part of the tumor was close to a surgical margin. Other surgical margins were all negative. Immunohistochemical markers were S-100 (), CD68 (), NSE (), Vimentin (), CK (), GFAP (), GSMA (), Des (). No recurrence was found in the follow-up after the operation.
Histological picture.
Immunohistochemical picture.
Histological picture.
Immunohistochemical picture.
Case 3
The patient was a 38-year old woman who had a contusion on the left hand 10 years ago, and found atrophy of the left thenar muscle a month ago. Ten years ago, the patient encountered a contusion on the left hand, which induced pain on the left hand; and she did not receive systematic treatment. In the last month, the ulnaris of the left hand felt numbness and pain, and the left thenar muscles developed atrophy. In addition, a mass with a size of a broad bean was found in the left cubit nerve. Physical examination results: body temperature, 36.8C; pulse, 68 times/min; respiration, 18 times/min; blood pressure, 130/90 mmHg. Vital signs of the patient were stable, and heart, lung and abdomen examinations revealed no abnormality. The left thumb, indicator and middle fingers felt dull. The left thenar muscles developed atrophy. The opposition movement of the thumb was weak. The Tines sign of the median nerve at wrist was positive. Wrist flexion test (Phaien sign): flexing of the elbow, lifting the forearm, and simultaneously flexing double wrists by 90 degrees. One minute later, the left side presents with stimulation symptom of the median nerve. A mass was felt in the left cubit nerve, with a size of approximately 1.5 2.0 cm. The texture was hard, with poor activity. No redness was observed on the skin surface. The skin temperature did not increase. The carpal tunnel presented no inflammation or tumor, and was locally uplifted. The left hand palm had tenderness when touched. Other physical examinations revealed no abnormalities. Electrophysiological results: motor nerve conduction velocity of the median nerve and left ulnar nerve was normal, while sensory conduction velocity was reduced. Clinical diagnosis was a mass in the left cubit nerve. Patient underwent exploratory operation of the left carpal canal under brachial plexus block anesthesia: a Z-shaped incision was made on the left wrist, skin and subcutaneous tissues were cut off layer by layer, the ulnar tunnel was opened, and it was found that the deep branch of the ulnar nerve degenerated and swelled. No normal nerve tissue was found when the extima was incised. The mass had a gray color, hard texture and unclear boundaries. The resected tissues were subject to pathology, the extima of nerve was sutured, and the incision was washed and sutured layer by layer. Postoperative pathological results were as follows: the left cubit nerve met the criteria of GCT. Immunohistochemical markers were S-100 (), CD68 (), NSE (), Vimentin (), CK(), GFAP(), GSMA (), Des (). No recurrence was found in the follow-up after the operation.
Discussion
GCT is a rare soft tissue tumor. In 1926, Abrikossoff described it as a granular cell myoblastoma. GCT was considered to be derived from the lemmocytes in the neurilemma. Immunohistochemistry and electron microscopy have confirmed that GCT cells are derived from Schwann cells [10]. The author has read a large number of domestic and foreign literatures and found that the peak age of GCT ranged between 17–59 years, the median age was 36.5 years, and the average age was 30–50 years. GCT frequently occurs in the tongue, skin, subcutaneous tissues, breast and bladder; and rarely occurs in the female reproductive system. GCT patients with tumors in the vulva account for 7% of all GCT patients. GCT in the vulva can occur at any age and usually manifests as a single tumor, which more commonly presents in the female labia, and occasionally occurs in the clitoris [11]. In the present study, two types of GCT (GCT in the sheath of the right rectus muscle and GCT in the right wrist ulnar nerve) were reported; which have not been reported in previous literature. GCT is usually benign, and the incidence of malignancy is 2%. Bellezza et al. [12] reported the first case of MGCT. Fanburg-Smith et al. [6] reviewed 73 cases of GCT, and proposed that the diagnostic criteria of MGCT are that the tumor is characterized by rapid growth, the diameter is 5 cm, and the patients present with early recurrence or metastasis in local areas. Histological manifestations include necrosis, spindle cells, vesicular nuclei (large nucleoli), mitotic figures 2/10 HP, high nucleocytoplasmic ratio and pleomorphism. A tumor in accordance with 3 of these manifestations is considered to be histologically malignant; while those tumors, in accordance with manifestations 1–2, are considered to be AGCT. However, MGCT at the vulva is extremely rare, its treatment is not available, and follow-up is difficult. At present, only four cases of MGCT and three cases of AGCT at the vulva have been reported [13, 14, 15, 16, 17, 18]. The gold standard for the diagnosis of benign GCT are as follows: histopathology: under a light microscope, The tumor boundary can be clear or local infiltration, diameter 3 cm, up to 6 individual cm; plane heterogeneity, hard texture, gray, grayish yellow or yellowish brown. Microscopically, the tumor cells are lined with nests, bands, or cords, separated by thin fibrous tissue, and occasionally neoplastic cells are arranged in sheets. The tumor cells are round, oval or polygonal, and the cytoplasm is rich. Eosinophilic coarse granules or eosinophilic globules [19] can be seen. The tumor cells were well differentiated, there are a few mild to moderate atypia, mitotic figure, immunohistochemistry, tumor cell S-100 (), NSE (), vimentin (), and CD68 (), GFAP (), chromogranin (), synaptophysin (), NF (), EMA (), CK (), desmin () and HMB45 () [19, 20]. At present, the treatment of GCT is mainly surgical treatment. For MGCT, patients undergoing radiotherapy and chemotherapy are few. Studies have revealed that GCT is not sensitive to radiotherapy and chemotherapy [21, 22, 23, 24, 25]. Benign GCT at the vulva has not a capsule. Hence, tumor cells can infiltrate into local tissues. In the operation, in addition to complete resection of the tumor, the resection range can be extended to areas without invasion, in order to prevent recurrence.
References
1.
AbrikossoffA., Uber myome, ausgehend von der quergestreiften wilkuerlichen muskulatur, Virchows Arch Pathol Anat260 (1926), 215–233.
2.
FletcherC.D.M.BridgeJ.A.HogendoornP.C.W. et al., WHO Classification of Tumours of Soft Tissue and Bone, 4th Edition, Lyon, IARC, 2013, pp. 178–179.
3.
WeissS.W. and GoldblumJ.R., Enzinger and Weiss’s Soft Tissue Tumor, fifth Edition, St Louis, Mosby, 2008, pp. 878–887.
4.
LackE.E.WorshamG.F.CallihanM.D.CrawfordB.E.KlappenbachS.RowdenG. and ChunB., Granular cell tumor: A clinicopathologic study of 110 patients, J Surg Oncol13 (1980), 301–316.
5.
CheewakriangkraiC.SharmaS.DeebG. and LeleS., A rare female genital tract tumor: Benign granular cell tumor of vulvar: case report and review of the literature, Gynecol Oncol97 (2005), 656–658. PMID: 15863174, DOI: 10.1016/j.ygyno.2004.12.058.
6.
Fanburg-SmithJ.C.Meis-KindblomJ.M.FanteR. et al., Malignant granular cell tumoy of soft tissue: Diagnostic criteria and clinicopathologic correlation, Am J Surg Pathol22(7) (1998), 779–779.
7.
KhansurT.BalducciL. and TavassoliM., Granular cell tumor. Clinical spectrum of the benign and malignant entity, Cancer60 (1987), 220–222.
8.
SonobeH.IwataJ.FurihataM.MorikoT. and OhtsukiY., Malignant granular cell tumor: Report of a case and review and the literaure, Pathol Res Pract194 (1998), 507–513.
9.
KataokaA.KoikeM.KuranukiK.WakayamaK.YamadaS.AkasakaY., A case of malignant granular cell tumor arisen in the chest wall (in Japanses with English abstract), J Jpn Surg Assoc66 (2005), 2403–2406.
10.
PergelA.YucelA.F.KaracaA.S.AydinI.SahinD.A. and DemirbagN., A therapeutic and diagnostic dilemma: granular cell tumor of the breast, Case Rep Med2011 (2011), 972168.
11.
BecelliR.PeruginiM.GaspariniG.CassoniA. and FabianiF., Abrikossoff’s tumor, J Craniofac Surg12(1) (2001), 78–78.
12.
BellezzaG.ColellaR.SidoniA. et al., Immunohistochemical expression of Galectin-3 and HBME-1 in granular cell tumors: A new finding, Histopathol23(9) (2008), 1127–1127.
13.
LaxmishaC. and ThappaD.M., Granular cell tumor of the clitoris, J Eur Acad Dermatol Venereol21 (2007), 392–393.
14.
BehzatogluK. and BahadlrB., Malignant granular cell tumor with unusal histological features, Pathol Int57(2) (2007), 115–115.
15.
HorowitzI.R.CopasP. and MajmudarB., Granular cell tumors of the vulva, Am J Obstet Gynecol173(6) (1995), 1710–1710.
16.
SchmidtO.FleckensteinG.H.GunawanB.Recurrenceet al. and rapid metastasis formation of a granular cell tumor of the vulva, Eur J Obstet Gynecol Reprod Biol106(2) (2003), 219–219.
17.
JardinesL.CheungL.LiVolsiV. et al., Malignant granular cell tumors: Report of a case and review of the literature, Surgery116(1) (1994), 49–49.
18.
RamosP.C.KappD.S.LongacreT. et al., Malignant granular cell tumor of the vulva in a 17-year-old: Case report and literature review, Int J Gynecol Cancer10(5) (2000), 429–429.
19.
LeB.H.BoyerP.J.LewisJ.E. and KapadiaS.B., Granular cell tumor: Immunohistochemical assessment of inhibin-alpha, protein gene product 9.5, S100 protein, CD68, and Ki-67 proliferative index with clinical correlation, Arch Pathol Lab Med128(7) (2004), 771–771.
20.
RobertsonA.J.McIntoshW.LamontP. et al., Malignant granular cell tumor (myoblastoma) of the vulva, Report of a case and review of the literature, Histopathology5(1) (1981), 69–69.
21.
MagoriV.A.SzegvariM., Rezidivierender und metastasierender Abrikossoff-Tumor der Vulva, Zentralblatt Fur Pathologie und Pathologische Anatomie117(3) (1973), 265–265.
22.
RosenthalS.A.LivolsiV.A. and TurrisiA.T., Adjuvant radiotherapy for recurrent granular cell tumor, Cancer65(4) (1990), 897–897.
23.
RamosP.C.KappD.S.LongacreT.A. and TengN.N.H., Malignant granular cell tumor of the vulva in a 17-year-old: Case report and literature review, Int J Gynecol Cancer10(5) (2000), 429–429.
24.
Castillo LaraM.Martínez HerreraA.Torrejón CardosoR. and Lubián LópezD.M., Granular cell tumor in breast: A case report, Breast Cancer9 (2017), 245–248.
25.
Jiménez-HerreroE.Hervás-MarínD. and Vera-SempereF.J., Expresión de calretinina en el tumor de células granulares: Análisis del gradiente de intensidad en la inmunotinción con correlación clínico-patológica, Rev Esp Patol47(3) (2014), 149–155.