
Abstract
Pulmonary granular cells tumors (CGT) are rare tumors, that derive from Schwann cells. In the tracheobronchial and pulmonary tree, they remain a diagnostic challenge. There are no well-established criteria to differentiate between benign, atypical, and malignant GCT. Moreover, its real frequency in the respiratory tract is still unknown. Here, we represent 2 cases of bronchial and lung GCTs. We aim to highlight the frequency of all clinicopathological characteristics of this rare tumor in the tracheobronchial and pulmonary tree location based on our cases and the available literature in a large systematic review.
Introduction
A granular cell tumor (GCT) is a rare mesenchymal tumor that derives from Schwann cells. It was described for the first time by Abrikossoff and it was called granular cell myoblastoma. 1 It occurs almost at any location in the body. They are most frequently found in the tongue, thoracic region, and upper extremities. 2 They occur rarely in the tracheobronchial and pulmonary tree, where they constitute a diagnostic challenge.3,4,5 There are no well-established criteria to differentiate between benign, atypical, and malignant GCT, as the gray zone, where lesions present the potential for metastasis or local aggressiveness, still needs to be well investigated and better characterized. We aim, through our 2 cases and based on our review of the literature, to highlight the frequency of GCTs of the lung and tracheobronchial tree and to investigate their clinicopathological characteristics in this rare localization, to better diagnose these lesions.
Case 1
A 47-year-old man attended the hospital with a 3-month history of chest pain and shortness of breath. He was a smoker and had no personal or family history of malignancy.
Physical examination demonstrated no abnormalities
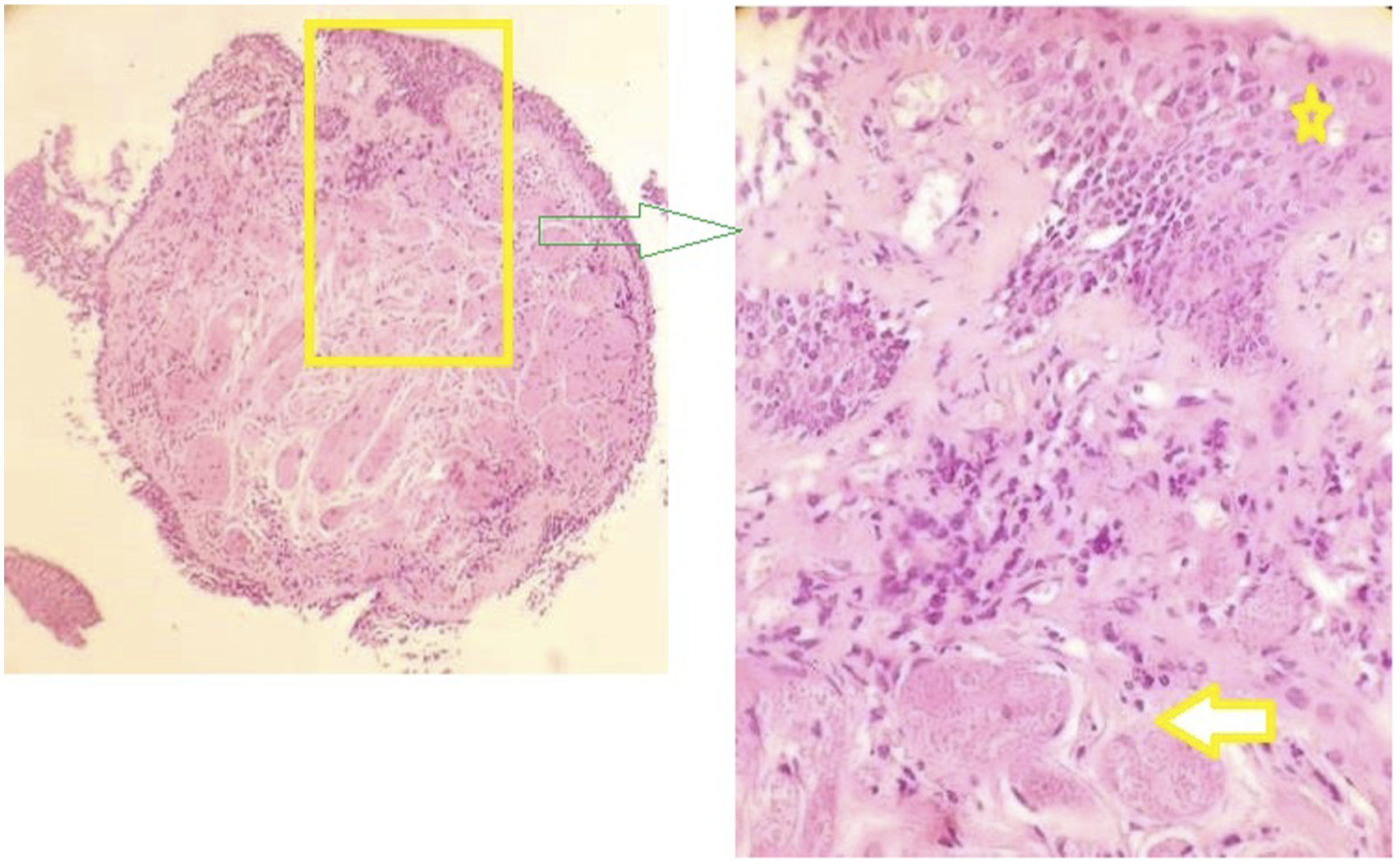
Chest radiograph demonstrated a right hilar opacification which was thought to be malignant (Figure 1). Direct bronchoscopy revealed an obstruction of the bronchi of the third segment of the right upper lobe by a submucosal tumor mass (Figure 2). A transbronchial biopsy was performed. Microscopic examination showed a submucosal mesenchymal proliferation which was composed of large polygonal cells with eosinophilic granular cytoplasm, nuclei with prominent nucleoli, and absence of mitotic figures. Clusters of cells were separated by delicate fibrovascular stroma (Figure 3). No necrosis, pleomorphism, large nucleoli, spindling, or high N/C ratio was seen. Trapped submucous glands were also present. Immunohistochemistry revealed PS100-positive tumor cells (Figure 4). Chest radiograph: a right hilar opacification. A submucosal tumor mass protruding into the luminal airway. Endobronchial biopsy of granular cell tumor (case 1): A bronchial wall covered with metaplastic, reactive squamous epithelium (yellow star), lying above tumor tissue (arrow) composed of oval to round cells with abundant granular, eosinophilic cytoplasm, with small nuclei (H&E). Immunohistochemistry (case 1): tumor cells were strongly positive for S-100.


The patient had Magnetic resonance imaging, which showed secondary bilateral paravertebral lesions concordant with GCT metastases. After a multidisciplinary consultation and discussion with the patient, it has been decided not to perform surgical resection on these metastases as they are not amenable to surgical removal. Palliative radiotherapy has been proposed as an option if the patient develops symptomatic manifestations.
Case 2
A 45-year-old man suffered from a chronic cough for several months. He had a history of smoking. Physical examination was normal.
The chest radiograph demonstrated a nodular lesion in the upper lobar segment. Bronchoscopy showed an obstructive endobronchial lesion. Biopsies were taken.
Histologically, tumor tissue was built from clusters of round to oval and some polygonal cells with eosinophilic, finely granular cytoplasm and small nuclei, with occasional nucleoli.
Between the clusters of tumor cells, fibrous tissue was focally present. These tumor cells were infiltrative between bronchial glands (Figure 5). Immunohistochemically, all tumor cells were S-100 (Figure 6) and vimentin-positive. Human Melanoma Black-45 (HMB-45) and Cytokeratin were negative. The patient was treated by endoscopic resection. The follow-up didn’t notice any recurrence or metastasis. Endobronchial biopsy of granular cell tumor (case 2): polygonal tumor cells were infiltrative between bronchial glands (H&E). Immunohistochemistry (case 2): S-100 positive.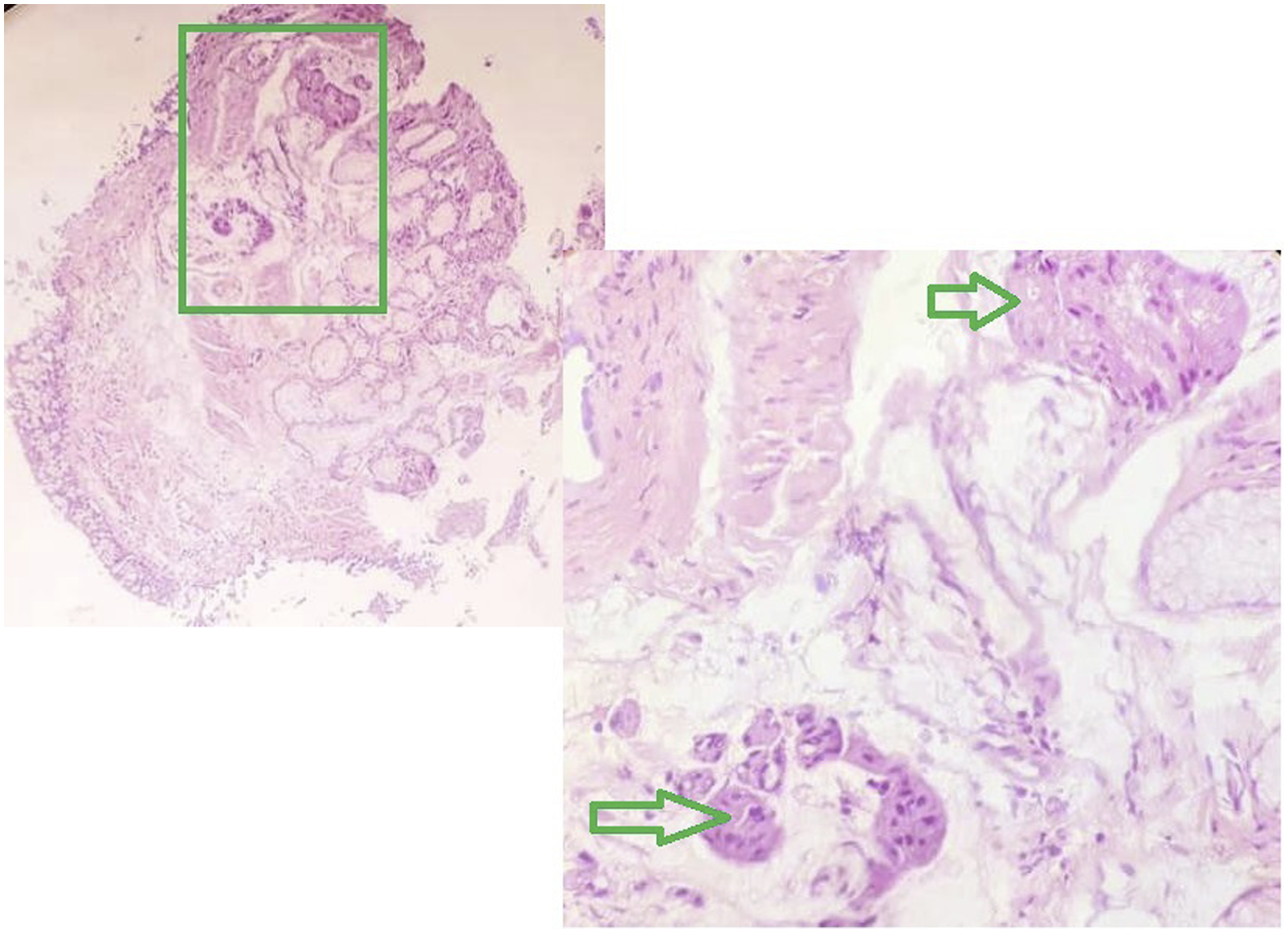

Review of the literature
All potentially eligible articles were screened, at the title, abstract and full-text stages. The review was conducted based on the Preferred Reporting Items for Review and Meta-Analysis Protocols (PRISMA) statement. 6 The terms « granular cell tumor » and “granular cell myoblastoma » were searched in the PubMed database and 5181 titles appeared. We retained only studies reporting GCT of the respiratory tract, i.e., lung, trachea, and bronchi GCT. In this review, we included case reports and case series whatever the number of cases, in English and French literature reporting GCTs of the respiratory tract which detailed clinical and/or pathological characteristics. No case was excluded. The frequency of these findings was only calculated based on studies reporting them. Reports not searching for these findings were marked as non-available (NA).
Finally, 55 studies fulfilling these criteria were analyzed for clinicopathologic findings of GCT.2,7–61 These studies are distributed as follows:
A total of
The data collected were recorded on the exploitation sheet and were subject to computer entry and statistical analysis using the ‘Excel’ software.
Review of the litterature: Clinical characteristics.

R: right lung; L: left lung; NA: not available.
Clinical findings
GCTs affect women (63, 52.5%) more frequently than men (47, 39.1%). Information was unavailable in 12 cases (10%).27,28,29,30,32,35,36,45 The age ranged from 6 to 66 years. Smoke history was reported in 40 cases (33.33%), was absent in 14 cases (11.6%), and was not practiced in 66 cases (55%). The lesion was commonly described in the bronchus (94, 78.3%), and tracheal GCTs represented the second most localization (15, 12.5%). 11 GCTs were described in the lung (11, 9.1%). The right lung was more affected than the left one (51 vs 38, 42.5% vs 31.6%). Five cases were reported in the trachea.14,22,47,57,58
Most patients in this review presented with an asymptomatic nodule or mass discovered incidentally (32, 26.7%).8,9,45,57,58,59 Pulmonary multiple GCT was documented in nine lesions (7.5%).14,20,26,45,56,58 The coexistence with bronchopulmonary carcinoma was noticed in 14 cases (11.6%).25,48,56,58 Two patients had presented metastases at the moment of the diagnosis.56,58
The first case of metastatic GCT was a case of a 38-year-old nonsmoker man diagnosed with a malignant and obstructed GCT of the trachea with no further available information on this case. 56
The second case of metastatic GCT was a case of a 51-year-old nonsmoker woman diagnosed with a malignant GCT. She presented with a 6.4 × 6.1 × 4.4 cm infra hilar left lower lobe mass with extrinsic compression and obstruction of the left mainstem on enhanced computed tomography. Pathology of the resection specimen confirmed a GCT composed of sheets of tumor cells with pleural, pericardial, and diaphragmatic metastases. Molecular analysis by next-generation sequencing failed to yield any driver mutations common to primary lung adenocarcinomas. 58
Pulmonary metastases from malignant oesophageal GCT had been reported. 18 The follow-up was available for 18 cases (15%), ranging from 1 month 52 to 28 years. 56 Two tumors showed recurrence: one with large tracheal infiltration and positive surgical margin, 1 year later, 14 and the second 3 weeks later. 35 However, the most common patients were disease free Treatment was based on surgical resection, endoscopic resection, electrocautery, and laser.
Histopathological findings

Perineural invasion was noted in three neoplasms (2.5%).18,45,57 Vascular invasion was not reported in the published cases. Inflammatory cells were present intratumorally, peritumorally, or both in 11 cases (9.1%). Necrosis was reported in 3 cases (2.5%).18,19,58
The Fanburg-Smith and the Nasser histological criteria were collected for all studies when available. 61 According to the Fanburg-Smith criteria, the most common pulmonary GCTs were benign (117, 97.5%). Only three primary malignant GCT in the lung and the tracheobronchial tree had been described (3, 2.5%),19,56,58 with two tumors with distant metastases.56,58 Only 2 cases of the recurrent disease had been reported.14,35
Discussion
Through these two reported cases and from all previous reports we analyzed and tried to extract the exact frequency of GCTs and their clinicopathological characteristics. GCT remains an interesting tumor occurring widely, with most cases following a benign course. Malignant behavior is described on rare occasions. Our study supports these findings with no metastatic case found in our two patients and rare metastatic cases reported in the literature. Our two reports patients were men aged 45 and 47 years old, diagnosed with benign GCT located in the bronchi, revealed by dyspnea, shortness of breath, and chronic cough. They were managed by surgical resection, with negative margins without any progression at follow-up.
Histologically, Tumors were characterized by an infiltrative growth pattern in our 2 cases. Few studies found perineural and vascular invasion in GCT, considering these features as benign findings that have no adverse outcome. In our 2 cases, no perineural invasion or vascular invasion was found. These findings are similar to the literature.
Primary pulmonary and tracheobronchial tree GCT is known to comprise 6%-10% of all GTCs.8,9 Two large series have studied GCT of the lung in their different clinicopathological aspects.59,60
These tumors are derived from Schwann cells. They present a wide spectrum of clinical, biological, and pathological findings. They develop between the third and fourth decades of life and are more commonly seen in women. GCTs are developed frequently in the bronchus, then the trachea, and finally in the lung. The right lung seemed to be more affected than the left one. In our reported two cases, GCTs were endobronchial. Most patients are asymptomatic, with a polypoid nodule ranging from a few millimeters to 8 cm. 2 The most common symptoms are cough, shortness of breath, chest pain, and recurrent pneumonitis. On endoscopy, the lesion is more polypoid and limited than infiltrative, contrary to the other localization, in which the infiltrative growth pattern is observed in 60% of the cases. 61 Four percent to 10% of pulmonary GCTs are multicentric. 21 Multiple pulmonary GCTs most commonly occur as endobronchial tumor masses.9,15,21,27,46,57,59 It is important to emphasize that multifocality is not a sign of malignancy and to stress that infiltration of surrounding tissue is a common finding in lung benign CGT. Local peri bronchial extension in lung parenchyma may be present in up to 40% 60 but with extremely rare direct lymph node infiltration.2,59
Pulmonary GCT can occur with synchronous GCT in other organs, or alongside other neoplasms2,8
Only 3 cases of malignant GCT in the pulmonary and tracheobronchial trees had been reported in the literature.19,56,58 Malignant GCTs affect more frequently women than men. According to the available information in the literature review, perineural invasion in pulmonary and tracheobronchial GCT is seen in almost 1.6- % of the reported cases. No case of vascular invasion had been reported in this localization. Necrosis and Mitosis are not frequent. They were reported in two malignant GCTs, and one benign GCT.18,19,58 In the third malignant reported GCT, these histologic characteristics were not precise. 56 Despite their high reproducibility, necrosis, and mitosis may indicate an increased risk of malignant evolution, which are not strong correlators with malignancy in GCTs in this studied localization. This finding leads us to wonder if the Fanburg-Smith and the Nasser histological criteria are also applicable in pulmonary and tracheobronchial tree localization. We think that only metastases may classify tumors as malignant. In fact, in our first reported case, no histologic criteria of malignancy were found, however, the patient had developed metastases.
Some authors stipulate that the upregulation of p53 as well as Ki67, a nuclear proliferative marker, are well correlated with an aggressive clinical course and malignant behavior of GCT of soft tissue. In a recent study, p53 immunostains were negative and Ki67 was less than 1% in all benign cases. 62
Differential diagnosis is discussed according to the benign or malignant presentation. For benign GCT, it includes fibroxanthoma and leiomyoma. Malignant GCTs are more difficult to diagnose owing to their unusual presentation. The differential diagnosis includes a large spectrum of diseases such as malignant peripheral sheath tumors, histiocytosis, Rosai-Dorfman disease, PEComa, melanoma, carcinoma, and alveolar soft tissue sarcoma. A large panel of immunohistochemical stains will be needed in some cases. The correlation between morphological analysis and immunohistochemical results is mandatory to make the diagnosis.
The treatment of GCT of the lung is based on tumor size and the extent of infiltration. Small tumors (<1.0 cm) may be treated by bronchoscopic extirpation, laser therapy, or sleeve resection. Larger tumors (>1.0 cm) that usually extend beyond the tracheobronchial cartilage are usually treated by surgical resection. 19
Due to the low number of true malignant cases and series, information about the prognosis is still lacking.
Conclusion
In conclusion, this paper reports two other benign cases of endobronchial GCT, in addition to the largest review of the literature on pulmonary and tracheobronchial GCTs.
GCT remains an interesting tumor in this localization, with most cases following a benign course and a malignant behavior described on rare occasions. They may occur without symptoms. The rare cases that showed metastatic spread did not correlate with the histological features typically associated with aggressive behavior. The most available malignancy criteria in this localization are metastases.
Supplemental Material
Supplemental Material - Granular cell tumor of the lung and tracheobronchial tree: two case-presentation with a review of the literature
Granular cell tumor of the lung and tracheobronchial tree: two case-presentation with a review of the literature by Yoldez Houcine, Mouna Mlika, Chirine Moussa, Houda Rouis, Emna Brahem, Olfa Ismail, Sonia Maȃlej and Faouzi El Mezni in Rare Tumors
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Informed consent for these 2 cases was obtained from patients
Data Availability Statement
The authors declare that any datasets used can be accessed Epidemiology 1-2 Diagnostic challenge of granular celle Tumor in the tracheo-bronchial tree location: 3-6 published cases of granular cell tumor: 7-61
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.