
Abstract
Granular cell tumors (GCT) are rare mesenchymal tumors belonging to Schwann cell lineage constituting 0.5% of all soft tissue neoplasms. They occur in skin, subcutaneous tissues, mucosal surfaces including within the deeper organs. They are considered unusual and unique neoplasm due to their distinctive pathologic diagnosis. Such a rare case has been discussed here due to unusual age at presentation and in its location.
* GCT is a primarily a pathologic diagnosis without any distinctive clinical or imaging features. * Granular cell tumors (GCT) are rare mesenchymal tumors of Schwannonian differentiation constituting 0.5% of soft neoplasms. * Commonly seen as an uninflamed asymptomatic nodular mass measuring about two to three cms in diameter with a pink or yellowish surface coloration
* Clinically it can be misdiagnosed as dermal appendageal tumor or soft tissue tumor. * Though literature is abundant with GCT in adults along with its occurrence in multiple sites in children, but however its location in the upper back in a female child has been rarely reported so far. This pathological lesion defies the popular myth that, small, asymptomatic nodular lesions should be left untouched.What is known
What is unknown
Introduction
Previously GCT (granular cell tumor), were thought to be of muscular origin, but now, however, they are considered to be originating from Schwann cells or neural origin due to their positivity for S-100 protein. GCT are completely different from granular cell changes happening in many neoplastic and non-neoplastic diseases. GCT are usually small, solitary nodular lesions, occurring at any age group, mostly seen in subcutaneous tissues. However, 5%–10% occur in multiple locations and malignancy is reported in 1%–2%. Commonly seen as an asymptomatic nodular mass measuring about two to three cms in diameter with a pink or yellowish surface coloration.1–3
Case Report
Nine-year-old female child was brought to us with history of asymptomatic swelling noticed on the right scapular region since 1 year, while giving bath by mother. It was of peanut size initially, gradually increased to present size of 2 cm × 1 cm (Figure 1(a)–1(c)). On examination there was an asymptomatic non tender nodular swelling noticed on right scapular region in the subcutaneous plane, freely mobile with normal skin over it. Sonography revealed it to be epidermoid cyst and surgical was planned. Under general anesthesia, yellowish colored, non-encapsulated nodular swelling in the subcutaneous plane just above muscles and its fascia. Swelling was excised in toto (Figure 1(a)–(d)) and histopathology revealed to be, non-encapsulated neoplasm , composed of uniform cells in groups having abundant granular eosinophilic cytoplasm and hyper chromatic nuclei without any kind of atypia, mitosis, necrosis or malignant changes (Figure 1(d)–(f)). Child is on follow up without any symptoms or recurrence. (a)-and (b) -Intra operative appearance of granular cell tumor in the subcutaneous tissue upper back. (c)-Excised yellowish colored GCT. (d)-post operative appearance. (e)-Histopathological image-Hematoxycillin and Eosin stain (H and E)- 100X-well circumscribed non encapsulated neoplasm composed of uniform cells arranged in groups. (f)- H AND E−400X cells with abundant granular eosinophilic cytoplasm and hyperchromatic nuclei.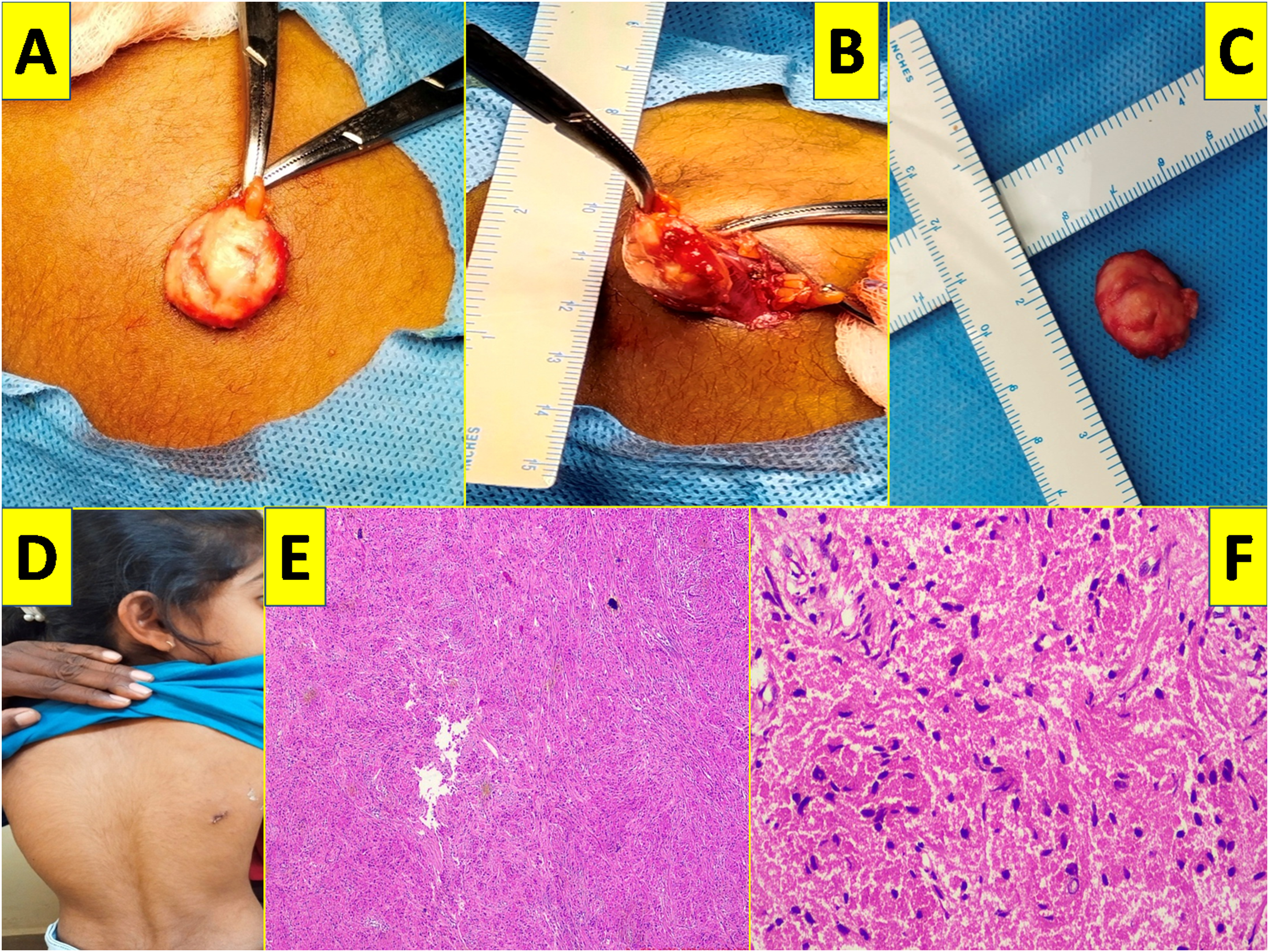
Discussion
Initially described by Abrikossoff in 1926 as ‘granular cell myoblastomas’. However, recently they are labeled as Granular cell tumors (GCT), due to their schwannian cell or neural origin. Clinically they are diagnosed as dermal appendageal tumor or soft tissue tumors. Definite diagnosis can only be made by excision and histopathological examination, confirmed by immunohistochemistry (IHC).1–3
The pathogenesis of the GCT still remains unknown. However, histochemical and ultra structural studies propose the origin of these lesions from Schwann cells, striated muscle, mesenchymal cells, histiocytes or epithelial cells. Histologically GCT are characterized by non-encapsulated tumors lined by irregular sheets of large, round or polygonal cells with indistinct cell border, containing abundantly eosinophilic, granular, pale staining cytoplasm having small, round or oval nuclei. Granularity of the cytoplasm may be due to massive accumulation of lysosomes.1,3,6
Fanburg-smith et al, classified GCTs into benign, atypical and malignant categories based on six histologic criteria (necrosis, spindling, vesicular nuclei with large nucleoli, increased mitotic activity, high nuclear to cytoplasmic ratio and pleomorphism).1–3
Benign GCTs have a focal pleomorphism alone or none of the above-mentioned criteria; however, atypical GCTs have 1 to 2 criteria, whereas, malignant GCT have 3to 6 criteria.1–3
A higher Ki-67 proliferation index (>10%) and overexpression of p53 are also seen in atypical and malignant GCTs.1,3,6
Malignant GCT are aggressive, require wide resection, have poor response to chemotherapy and radiotherapy, hence likely to recur.1,3,6
Whereas benign GCT are small, have good response to excision and carry good prognosis.1,3,6
Vascular lesions, lipoma, benign mesenchymal neoplasm, neurofibroma, traumatic fibroma, squamous cell carcinoma, dermatofibroma. Keratoacanthoma, leiomyoma and keloid are among the differential diagnosis for this lesion.4–6
GCTs are usually asymptomatic, slow growing smooth surfaced or hyperkeratotic solitary nodules and are non-encapsulated. They are commonly seen in intradermal, subcutaneous, or in submucosal lesions.4–6
Pathologically GCTs have round or polygonal cells arranged in cords or nests; with small eccentrically place nuclei and abundant eosinophilic granular cytoplasm. Cells have indistinct borders like syncytial appearance.1–6
Since a majority of the GCTs, follow a benign clinical course, therefore requiring conservative surgical excision with a low rate of recurrence. When GCT metastasis to regional nodes or organs is considered in malignant.5,6
A malignant GCT is aggressive and has poor prognosis, whereas, a benign GCT has excellent outcome after surgical excision.5,6
Author had a nine-year-old female child with an asymptomatic nodular swelling in the back since 1 year. A solitary well defined non encapsulated yellowish colored swelling in the subcutaneous tissue not adherent to surrounding tissues was excised and its histopathology revealed it to be granular cell tumor (Figure 1(e) and (f)). Child is doing well on 3 years follow up without recurrence. Child, still needs to be evaluated at periodic intervals to rule out malignant transformation and late recurrences.
One case of malignant GCT over the back in an adult has been reported in literature; however here, author reports a benign GCT over the upper back in a child and its management. 7
Though literature is abundant with GCTs in adults along with its occurrence in multiple sites in children, but however its location in the upper back in a female child is the first ever case to be reported so far.
Conclusion
Clinically appearing benign asymptomatic small nodular swelling or soft tissue tumor, should be excised to reveal its true pathological nature which can affect the further management of the patient
However, follow up at regular and periodic intervals should be emphasized to rule out malignancy or metastasis.
This pathological lesion defies the popular myth that, small, asymptomatic nodular lesions should be left untouched.
Footnotes
Acknowledgements
The author would like to thank all her pediatric surgical colleagues and other staffs of IGICH, Bengaluru, Karnataka, India.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.