
Abstract
BACKGROUND:
High-mobility group A2 (HMGA2) has been investigated to be associated with tumorigenesis; however, the expression pattern and clinical significance of HMGA2 in non-small cell lung cancer (NSCLC) remains poorly understood. The purpose of this study is to examine the expression of HMGA2 and to analyze its relationships with respect to clinico-pathological features and patient survival in NSCLC.
METHODS:
The expression level of HMGA2 was examined by Western blot and immunohistochemistry in NSCLC cells and tissues. The relationship between HMGA2 expression and survival of NSCLC patients was calculated by a Kaplan-Meier method and the evaluation of risk factor was determined by the multiple regression analysis.
RESULTS:
NSCLC tissues exhibited a higher expression level of HMGA2 compared to normal tissues (
CONCLUSIONS:
HMGA2 was highly expressed in NSCLC tissues and cells and its overexpression was correlated with low-grade differentiation, lymph node metastasis, advanced clinical stage and poor survival time of NSCLC, which suggested that it could serve as a potential molecular marker and prognostic index for NSCLC.
Introduction
The incidence of lung cancer has significantly increased over the last century in China, largely due to environmental pollution and unhealthy lifestyles. Now lung cancer is the leading cause of cancer-related death in this country, with 733,000 expected deaths in China in 2015 and accounts for 28% of all cancer-related deaths among cancer patients in China [1]. Especially, morbidity and mortality of non-small-cell lung cancer (NSCLC) are relatively high, with a 5-year survival rate of less than 20%, which is often due to lung cancer first presenting at late stages and a lack of curative therapeutic options at these later stages. Over the past decade, the discovery of driver mutations has changed the landscape for the treatment of NSCLC [2]. In addition, the findings of abnormal molecule, gene mutation, and genetic phenotype have been suggested to improve the diagnostic accuracy of lung cancer at the early stage, such markers often guide patient treatment options and confer valuable prognostic information [3].
Recently, emerging studies reported that high- mobility group A2 (HMGA2) was correlated with many human malignancies and participated in different cellular activities, including cell cycle regulation, differentiation senescence [4]. The HMGA2 is coded by a gene on chromosome 12q14-15, which is characterized by its ability to bind to nucleotide sites rich in adenine and thymine [5]. Previous study show that HMGA2, the non-histone chromatin binding protein, plays important roles in the repair and protection of genomic DNA in embryonic stem cells and cancer cells [6]. Although over-expression of HMGA2 has been found in many kinds of malignant tumors, including colon, breast, pancreatic, and esophageal cancer; and the research results suggested that the up-regulation of HMGA2 is involved in the malignant phenotype of these cancers, which leads to poor prognosis for these patients with malignant tumors [3, 4]. The data on the natural expression status of the HMGA2 and its relationship with clinicopathological parameters of NSCLC patients remains insufficient. This study was to investigate the significance of HMGA2 expression in NSCLC and its clinical significance for NSCLC diagnosis and prognosis.
Material and methods
Cell lines of NSCLC
Human NSCLC lines NCI-A549 and NCI-H520 were obtained from the Cell Biology Department of Medical School, Xuzhou Medical University, China. Sixteen HBE cell line was purchased from the Tumor Institution, Academy of Chinese Medical Sciences, Beijing, China. The cell lines were treated strictly complying with a process previously described [7], the cells were cultured in RPMI 1640 medium with 10% FBS, 100 units/ml penicillin and 100
Patients selection
From January 2009 to December 2012, we collected a total 80 surgical tissue specimens from NSCLC patients who accepted surgical resection at the Lianyungang First People’s Hospital, Lianyungang, China. The diagnosis of lung cancer was confirmed by pathologists under the optical microscope, the type of pathology of some patients were determined with immunohistochemical pathology. These patients were not treated with chemotherapy or radiotherapy before surgery. Among these patients received surgery, 77 cases were patients with stage II–III, and only 3 patients belonged to stage IV. Forty adjacent normal lung tissues from NSCLC patients were selected as normal control. After removing the tumor mass via surgery, we carefully separated the cancer-adjacent normal tissues from the cancer tissues. The distance between the edge of cancer-adjacent normal tissues and tumor tissues was greater than 3 cm to avoid contamination of cancer cells. The individuals included in this project were classified according to different clinical features (Table 1). All patients were included in the follow-up program for collecting the data of survival. Definition of survival time: from the date of taking tissues samples (the time of surgery) to the date of patients’ death (or the last date lost to follow-up). In our study, the median follow-up was 36.7 months. This project was approved by the Institutional Review Board (Lianyungang First People’s Hospital, Lianyungang, China), and written informed consent was obtained from all subjects.
Clinico-pathological features of lung cancer patients (N
80)
Clinico-pathological features of lung cancer patients (N
Severe,
To produce the tissue microarray, pathologists from Shaanxi Chaoying Biotechnology Company (Li Jun and Wang Mei) selected morphologically representative cancer areas. The TMA was constructed strictly complying with a process previously described with an instrument from Beecher Instruments, Manual Tissue Arrayer, USA. Briefly, they removed a tissue core from the donor block with an inner diameter of approximately 2.0 mm and the each core sample from lung cancer tissue was placed into a recipient block according to a strict order. The array block constructed was sectioned and leveled on the microscope slide and then baked in an oven and finally tested with routine H&E staining and immunohistochemistry (IHC).
Immunohistochemistry (IHC)
The expression status of HMGA2 in NSCLC tissues was tested by IHC method (Kit of Ultra-sensitive S-P, produced by Zhongshan Jinqiao, Beijing, China), which was strictly performed according to a previous method that was described in published article [3]. The best dilution of anti-human HMGA2 antibody is 1:50 (Shanghai Changdao biological technology company). The positive staining slice of colon cancer served as a positive control; PBS took place of the first antibody as the negative control. The immunostaining of HMGA2 was assessed according to a previous method described [3]. Ten high-magnification fields of each tissue section were randomly selected (
Western blot
Western blot was employed to disclose the expression status of HMGA2 in NSCLC cells according to a standard method reported in a previous study [7]. The harvested NSCLC cells were washed once with PBS, lysed with 2
Statistical analysis
The SPSS 19.0 software package was used to perform the statistical analysis (SPSS Institute, version 19.0, Chicago, USA). The expression difference of HMGA2 and its relationships with clinico-pathological features of NSCLC was analyzed using the
Protein expression of HMGA2 in NSCLC tissues. (A) Low expression of HMGA2 in adjacent normal lung tissues (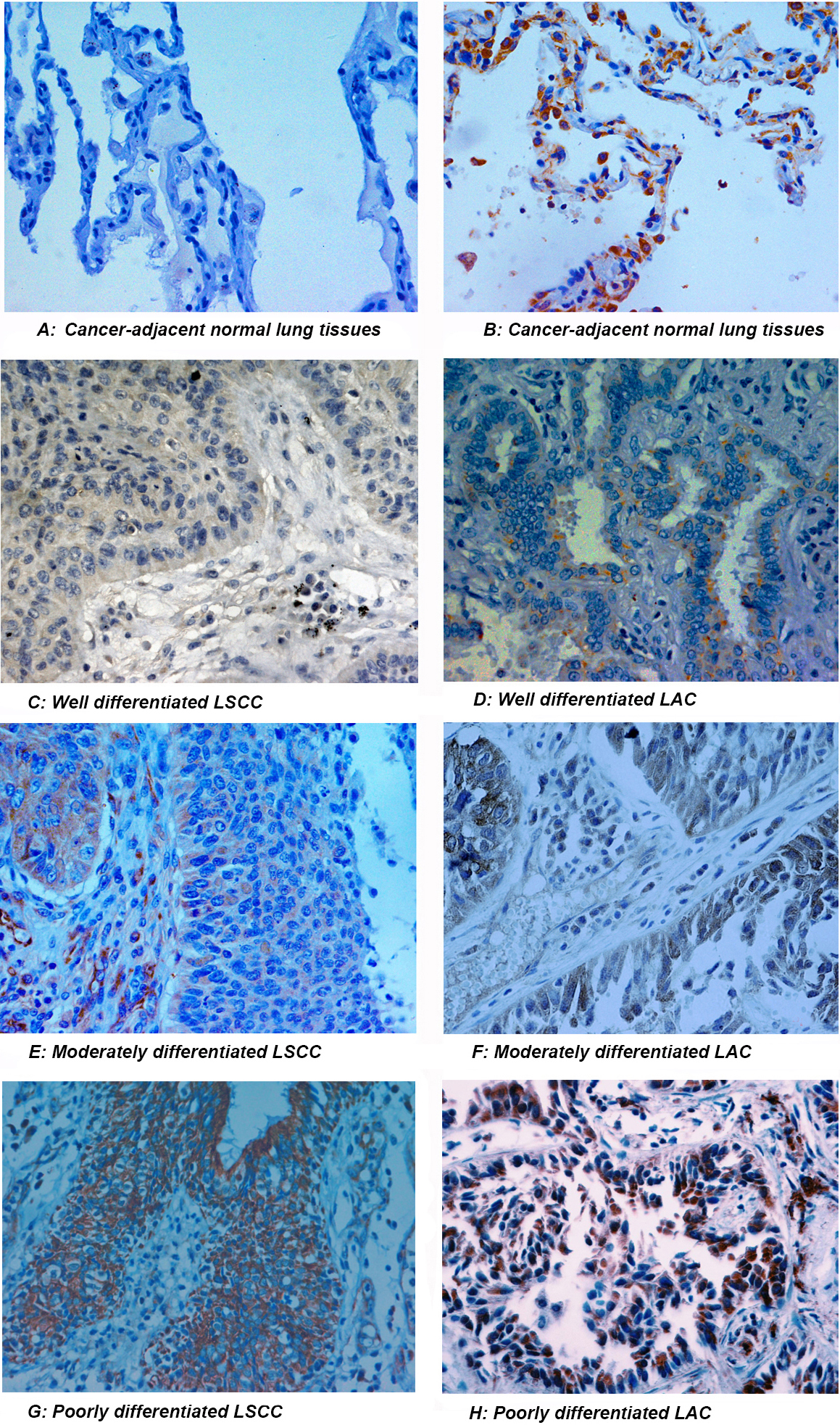
Correlation between clinico-pathological features and the expression of HMGA2 in NSCLC
Correlation of expression of HMGA2 with clinicopathologic factors of NSCLC patients and its expression in different cell lines. (A) Increased HMGA2 in lung cancer tissues compared with the normal tissues (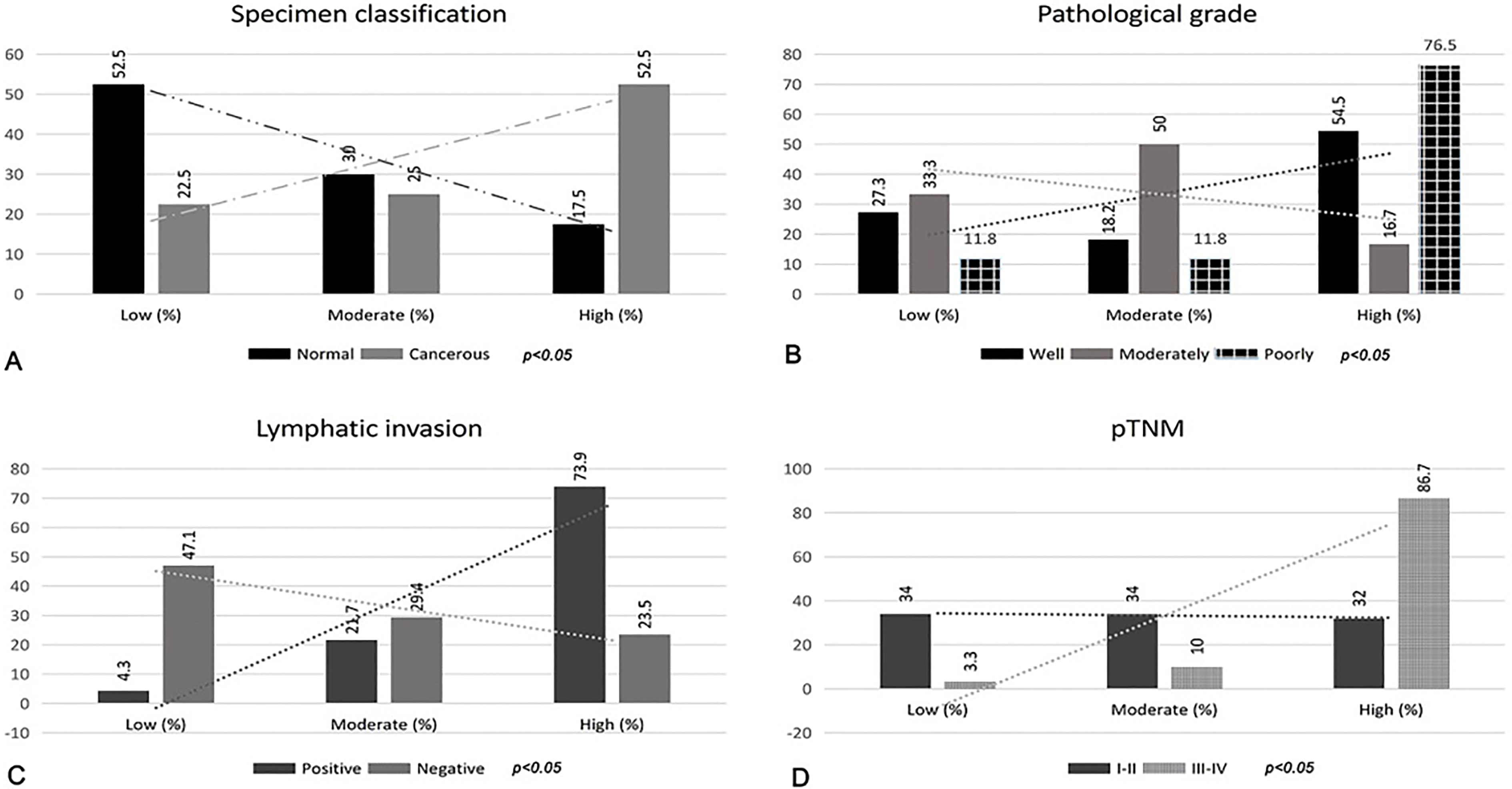
Cox proportional hazards regression model analysis of overall survival
LAC, lung adenocarcinoma; LSCC, lung squamous cell carcinoma; Smoking, pack years of smoking. OR, odds ratio; CI, confidence interval.
Expression of HMGA2 in different cell lines and the relationship between its expression and prognosis of patients with NSCLC. (A and B) Western blot analysis showed that the expression of HMGA2 was higher in A549 and H520 cells than in 16HBE cells (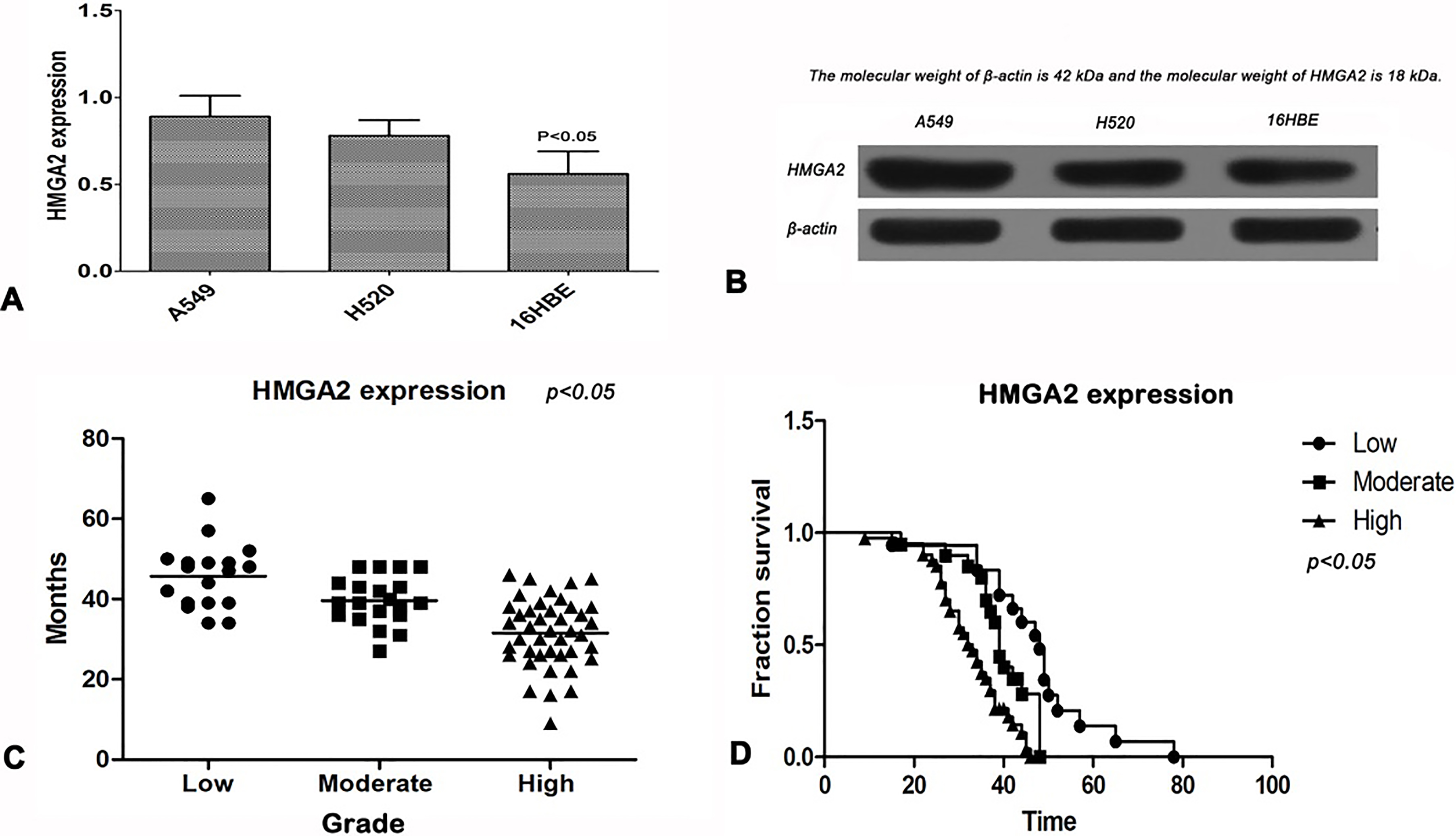
Comparison of HMGA2 expression in NSCLC tissues and cancer-adjacent normal tissues
HMGA2 protein was expressed in the cytoplasm of NSCLC cells, partially expressed in the nucleus, showing brown and yellow particles with different thickness (Fig. 1A–H). Simultaneously, a small amount of HMGA2 protein was also found in normal lung tissues, located in the cytoplasm and nuclei of cells. The statistical analysis showed that the high expression rate of HMGA2 in NSCLC tissues (42/80, 52.5%) was significantly higher than that in normal lung tissues (7/40, 17.5%), the difference was statistically significant (
Correlation of HMGA2 expression with clinico-pathologic factors of NSCLC patients
As shown in Fig. 2A–D, the expression of HMGA2 was correlated with some clinical parameters of NSCLC. Compared with moderately differentiated (4/24, 16.7%) and well-differentiated (12/22, 54.5%) NSCLC, poorly differentiated NSCLC showed a high expression of HMGA2 (26/34, 76.5%). In addition, the expression of HMGA2 in NSCLC tissues with lymph node metastasis (34/46, 73.9%) was significantly higher than that in NSCLC without lymph node metastasis (8/34, 23.5%). Furthermore, over-expression of HMGA2 was observed in NSCLC tissues in stage III–IV (26/30, 86.7%) compared to I–II NSCLC tissues (16/50, 32%). However, the expression of HMGA2 was not associated with gender, age, degree of smoking and histological type in patients with NSCLC (
Expression pattern of HMGA2 in A549 and H520 cells
We performed western blot analysis to determine the expression pattern of HMGA2 in A549, H520 cells and 16HBE cells, and found that the expression of HMGA2 was higher in A549 and H520 cells than in 16HBE cells (Fig. 3A and B). Quantitative analysis showed that the level of HMGA2 expression in the A549 (0.92
Correlation between HMGA2 expression and prognosis in patients with NSCLC
From the follow-up database, we obtained the survival data of NSCLC patients. Of the 80 patients, 71 had complete follow-up records. We sorted out the data and conducted a survival analysis. We drew Kaplan-Meier curves to disclose the correlation between HMGA2 expression and prognosis in patients with NSCLC. As shown in Fig. 3C and D, the results demonstrated that patients with high expression of HMGA2 had shorter survival time than those with moderate and low expression (
Multivariate statistical analysis of clinical parameters
When the survival time was defined as a dependent variable and a variety of clinical parameters were served as independent variables, we performed a Cox-regression analysis. The statistical results showed that the high expression of HMGA2 seemed to be an independent risk factor for the survival of patients with NSCLC (
Discussion
The high mobility group A2 (HMGA2) is a member of the high mobility group AT-hook (HMGA) family. HMGA2 plays a critical role in several cellular biological processes, including cell transformation, growth, differentiation, senescence and cycle control [9]. The HMGA2 protein is an architectural transcription factor that has recently been implicated in the development and progression of malignant tumors [4]. HMGA2 over-expression has been detected in several human malignancies, in particular pancreatic [8], gastrointestinal tract [4], and ovarian cancer [9] representing a very useful biomarker of malignancy [10]. Furthermore, highly expression of HMGA2 has been correlated with cancer proliferation, increased metastasis and poor prognosis in multiple types of cancer [5, 8, 9, 10]. In the world, lung cancer continues to be one of the top five causes of cancer-related mortality, with NSCLC being the most common subtype [11]. A few of studies display that HMGA2 is correlated with lung cancer and down-regulation of HMGA2 seems to reduce the proliferation and mobility of lung cancer [10, 12]. However, the data on the natural expression status of the HMGA2 and its relationships with clinicopathological parameters and survival of lung cancer patients remain insufficient.
In this study, we found that HMGA2 protein was highly expressed in the cytoplasm of NSCLC cells, which implied that HMGA2 was likely to be implicated in the occurrence and development of NSCLC. Previous study indicates that HMGA2 is an oncogene important in the pathogenesis of human lung cancer and that targeting HMGA2 can be therapeutically beneficial in lung cancer and other cancers characterized by increased HMGA2 expression [13]. Comparing matching tumor and non-tumorous samples from the same NSCLC patient, HMGA2 is revealed a highly significant overexpression in lung cancer cases, and thus suggests that HMGA2 overexpression is a common event in NSCLC and could serve as molecular marker for lung cancer [12]. We also found that a small amount of HMGA2 protein was also expressed in normal lung tissue, and located in the cytoplasm, suggesting that the function of normal cells was also depended on the function of HMGA2 signal. In our study, the high expression rate of HMGA2 in NSCLC tissues was significantly higher than that in normal lung tissues, and in particular in poorly differentiated lung cancer. Thus, we can infer that higher HMGA2 expression is potentially correlated with the malignant biological behavior of NSCLC. Our results are consistent with numerous prior studies that HMGA2 is up-regulated both in cancer cells and tissues compared with the normal cells and tissues [4, 5, 6]. In addition, we noticed that the expression of HMGA2 was correlated with lymph node metastasis (
In our study, Western blot was employed to further disclose the expression status of HMGA2 in different NSCLC cells. We found that the level of HMGA2 expression in the NSCLC cells was higher than that in normal bronchial epithelial cells. One newly study shows that HMGA2 is upregulated in lung adenocarcinoma (LAC) and associates with reduced overall survival in patients with LAC. HMGA2 knockdown suppresses the proliferation and motility of H1299 cells, while HMGA2 ectopic expression in A549 cells increases cell proliferation and migration [15]. As NSCLC is a highly malignant tumor, a clear understanding on the mechanism and action of HMGA2 in NSCLC cells will facilitate to disclose the biological mechanisms of NSCLC and help to improve the design of preventive treatment [16, 17]. Long-term follow-up analysis in our study indicated that high expression of HMGA2 showed a significant association with post-surgical survival time, suggesting that patients with high expression of HMGA2 had shorter survival than those with moderate and low expression of HMGA2. Subsequent Cox regression analysis further confirmed that high expression of HMGA2 might be an important risk factor (OR
Actually, there are several limitations in this study. First, it was carried out in single institute in east China, which may not represent the feature of the wider population. Second, the size of this study was relatively small and did not sufficiently assess difference of NSCLC level between lung cancers at early stages (I–II stage). Therefore, further investigations designing larger samples of patients with lung cancer are still required to get more solid and reliable conclusion.
Conclusion
In summary, our study demonstrated that HMGA2 was upregulated and positively associated with the poorly differentiated NSCLC, lymph node metastasis, advanced clinical stage and shorter survival time. The results suggested that the detection of HMGA2 may be served as a useful tumor marker for NSCLC diagnosis and could contribute to prognosis prediction of NSCLC.
Footnotes
Acknowledgments
This work was supported by Lianyungang City Science and Technology Bureau Funded Projects (No. SH1401). We wish to thank Dr. Gao WL and Rong BX for their helpful discussions and statistical assistance provided during the preparation of this manuscript and also wish to thank Dr. Li J and Wang M for technical assistance.
Conflict of interest
The authors have no financial conflicts of interest to declare.