
Abstract
Background and Aim:
Pulmonary large cell neuroendocrine carcinoma (LCNEC) is a rare neoplasm, and its clinical features and management are still limited. We evaluated the clinicopathological factors, including CDX2 immunohistochemical expression, to predict survival in patients with LCNEC.
Patients and Methods:
In all, 50 patients with LCNEC who underwent surgery at 4 institutes between 2001 and 2017 were included. Clinicopathological characteristics were evaluated for prognostic factors and statistically analyzed by Kaplan-Meier curve with a log-rank test or Cox regression models. We used immunohistochemical (IHC) analysis to determine the expressions of CDX2 and compared them with clinicopathological factors and survival.
Results:
Sixteen of the 50 cases (32%) were CDX2 positive. No correlation was found between the CDX2 expression by IHC and clinicopathological factors. Multivariate analysis identified adjuvant chemotherapy (hazard ratio [HR] =2.86, 95% confidence interval [CI] = 1.04-8.16, P = .04) and vascular invasion (HR = 4.35, 95% CI = 1.21-15.63, P = .03) as being associated with a significantly worse rate of recurrence-free survival.
Conclusion:
CDX2 was expressed in 1/3 of LCNEC but not associated with prognostic factor. Adjuvant chemotherapy and vascular invasion were associated with a negative prognostic factor of LCNEC.
Introduction
According to the World Health Organization (WHO), Cancer Fact Sheet published in 2019, about 2.09 million patients died of lung cancers in 2018, and it is the major cause of malignancy-related deaths worldwide. 1 Almost one-fifth of all lung cancers are presented as neuroendocrine tumors (NET), including typical carcinoid (TC) and atypical carcinoid (AC), as well as high-grade large cell neuroendocrine carcinoma (LCNEC) and small-cell lung cancer (SCLC). LCNEC and SCLC are hybrid tumors that are similar to each other.2,3
In 1991, LCNEC was first discovered in the lung, and it is present in approximately 1% to 3% of all lung cancer patients.3-5 Although almost 30 years have passed since LCNEC was first discovered, due to its infrequency and biology, treatment of LCNEC remains inconclusive.3,6-16 In addition, LCNEC is reported to have a poorer prognosis than non-neuroendocrine lung cancers and AC, and in some studies, it is comparable to SCLC.5,17 On the other hand, as the accuracy of diagnosis and screening system has improved, the rate of being diagnosed with LCNEC has increased.2,5
Recently, Caudal Type Homeobox 2 (CDX2) is a reported prognostic factor of colorectal cancer. 18 CDX2 is a homeobox gene known as a transcription factor with a crucial role for intestinal development and mainly express in midgut-related organ: colon, duodenum, and small intestine. Generally, CDX2 is not expressed in the lungs. Consequently, CDX2 has been useful to establish the gastrointestinal origin of metastatic adenocarcinomas and carcinoids, and can be especially useful in distinguishing metastatic colorectal adenocarcinoma from tumors of unknown origin. 19 However, it is reported that few of LCNEC expressed CDX2.20-23
In this study, we evaluated the outcomes of patients undergoing lung resection for LCNEC in order to identify the prognostic factors, including CDX2 expression.
Patients and Methods
Patients and samples
We investigated clinicopathological characteristics of 50 patients with Stage I to III LCNEC, which had been surgically resected during January 2004 and February 2017. Diagnosis of the LCNEC was according to the WHO Lung Tumors Classification Criteria: 24 (1) neuroendocrine morphology;:organoid necrotizing, palisading, trabeculae, or rosettes; (2) mitoses > 10 per 10 high power fields; (3) necrotic appearance; and (4) immunohistochemical expression of at least one neuroendocrine marker other than NSE (CD56, Chromogranin-A or Synaptophysin, etc.) in tumor cells. Paraffin blocks were retrieved from four institutions: The Department of General Thoracic, Breast and Pediatric Surgery, Fukuoka University School of Medicine and Hospital (Fukuoka, Japan); National Hospital Organization Fukuoka Higashi Medical Center (Koga, Japan); National Hospital Organization Omuta Medical Center (Omuta, Japan); and Imakiire Hospital (Kagoshima, Japan). Fukuoka University institutional ethical committee approved the retrospective study (2017M088) and waived the need for patient consent. We inspected each patient’s medical database for clinical information, including outcome information and follow-up status. Clinicopathological features were retrospectively analyzed, including sex, age, smoking history, size of the tumor, anatomical tumor location, lymph node metastasis, pleural invasion, lymphatic invasion, vascular invasion, adjuvant chemotherapy, and surgical approach. The pathological stage was determined according to the tumor/node/metastasis (TNM) classification vol. 8 of malignant tumors. 25 In all 50 cases, medical records and laboratory records confirmed that the origin of the tumor was the lung.
For the patients who received adjuvant chemotherapies, the selection of their regimen was also determined at the discretion of the attending physician. We categorized the adjuvant chemotherapy regimen into the non-small cell lung cancer (NSCLC) regimen group and the small cell lung cancer (SCLC) regimen group.
We collected all available paraffin blocks of these patients, and hematoxylin-eosin (H&E) slides were retrieved. All the H&E slides were examined, and the original diagnoses were confirmed.
Immunohistochemical analysis
CDX2 was detected in paraffin sections of LCNEC tissue. Four-micrometer sections were prepared for tissue slides. Antigen retrieval was performed at 95°C for 10 minutes in a microwave with Target Retrieval Solution (pH 9.0) S2367 (DAKO, Glostrup, Denmark) after deparaffinization. Followed by a cooling down period at room temperature for 20 minutes, then treatment with 3% hydrogen peroxide for 15 minutes at room temperature. After the treatment with TBST buffer S3006 (DAKO), Protein Block, Serum Free Solution X0909 (DAKO) was used to block non-specific binding incubate for 10 minutes at room temperature. Staining with anti-human CDX2 clone DAK-CDX2 M3636 (DAKO) with diluents using Antibody Diluent S2022 (DAKO), 1:100, was performed overnight at 4°C. After the treatment with TBST buffer S3006 (DAKO), Histofine Simple Stain MAX-PO (Nichirei, Tokyo, Japan) for CDX2 was applied and incubated for 30 minutes at room temperature. The substrate used DAB, and nuclear staining used hematoxylin. Negative controls used Negative Control Mouse IgG1 X0931 (DAKO) instead of the primary antibody. Immunohistochemical (IHC) staining was evaluated as previously described. 26
All slides were interpreted by two independent observers in a blinded fashion. For evaluation reliability, two independent assessors estimated the staining positivity of two serial sections.
Statistical analysis
All statistical analyses were performed using JMP 13.0 (SAS Institute Inc., Cary, NC, USA). The different variables of the tumors and normal tissues were analyzed with chi-square or Fisher’s exact tests. Recurrence-free survival (RFS) was determined from the date of operation to the first time of the first recurrence or metastasis. Overall survival (OS) was determined from the date of operation until death or the last follow-up visit. RFS and OS were analyzed using the Kaplan-Meier method and evaluated by the log-rank test. Significant differences were accepted at P < .05.
Results
A total of 50 cases of LCNEC were used in this study. The clinicopathological features of the patients are summarized in Table 1. The cohorts comprised 42 males (84%) and 8 females (16%), with a mean age of 69.5 years (range: 54-82 years). The median follow-up period was 50.0 months (range: 6-201 months). Within the follow-up period, 23 patients (46%) had a recurrence of LCNEC, and 23 patients (46%) died.
Patient characteristics (n = 50).

Abbreviation: TNM, tumor/node/metastasis.
The pathological stage distribution, according to the 8th edition of TNM were as follows. Stage IA1 in 6 patients (12%), IA2 in 9 (18%), IA3 in 6 (12%), IB in 7 (14%), IIA in 3 (6%), IIB in 12 (24%), IIIA in 3 (6%) and IIIB in 4 (8%).
Perioperative adjuvant chemotherapy was to 19 patients (38%). In detail, 8 (42%) of 19 patients received NSCLC regimens, 11 (58%) of 19 patients received SCLC regimens (Table 2).
Patient characteristics of adjuvant chemotherapy administrated group.

Abbreviations: AMR, Amrubicin; CBDCA, Carboplatin; CDDP, Cisplatin; CPT11, Irinotecan; GEM, Gemcitabine; NSCLC, non-small cell lung cancer; PTX, Paclitaxel; SCLC, small cell lung cancer; VP16, Etoposide.
CDX2 expression
The expression pattern of CDX2 is shown in Figure 1. CDX2-positive cases showed strong granular staining in nuclei of LCNEC from the resected specimens, although normal pulmonary cells did not show any positive staining of CDX2. In all, 16 out of 50 patients, 32% were CDX2-positive. As shown in Table 3, younger age and large tumor size were significantly related with CDX2 expression but not with other clinicopathological factors.

Representative CDX2 expression in pulmonary large cell neuroendocrine carcinoma (LCNEC) by immunohistochemistry (IHC). Nuclei of cancer cells were stained strongly in 3 + cases (50x, A, 200x, B) and 1 + (200x, C). Negative staining of LCNEC (200x, D).
Clinicopathological characteristics.

Abbreviations: CDX2, Caudal Type Homeobox 2; TNM, tumor/node/metastasis.
The 5-year RFS was 52.6% (62.2% for Stage I, 44.0% for Stage II, 0.0% for Stage III), whereas 5-year OS rate among the 50 patients was 55.1% (67.1% for Stage I, 43.3% for Stage II, 0.0% for Stage III) retrospectively.
Prognostic factors
In univariate analysis, no difference in the survival period was found in the CDX2-positive and CDX2-negative group (Table 4). We found that vascular invasion and lymphatic invasion showed prognostic significance by univariate analysis in OS (P = .01, hazard ratio [HR] = 3.87; 95% confidence interval [CI] = 1.42, 10.28/P = .02, HR = 3.65; 95% CI = 1.26, 10.19; Table 4). Adjuvant chemotherapy was associated with a deterioration in RFS compared to no adjuvant chemotherapy group (HR = 2.70; 95% CI = 1.18, 6.50; Table 4). In addition, there was no significant difference in RFS between both the NSCLC and SCLC regimen groups (P = .80, HR = 0.86; 95% CI = 0.25, 2.94; Table 4).
Univariate analysis of prognostic factors and survival; Cox proportional hazards model.

Abbreviations: CDX2, Caudal Type Homeobox 2; CI, confidence interval; HR, hazard ratio; NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer.
Multivariate analysis of survival was performed using 6 clinical prognostic factors, including age, sex, nodal metastasis, lymphatic invasion, vascular invasion, and adjuvant chemotherapy (Table 5). Patients who underwent adjuvant chemotherapy had a significantly lower prognosis than those without chemotherapy (P = .04, HR = 2.86; 95% CI = 1.04, 8.16). Furthermore, patients who had vascular invasions also had a significantly lower prognosis than those that did not have vascular invasion (P = .03, HR = 4.35; 95%CI = 1.21, 15.63).
Multivariate analysis of prognostic factors and survival; Cox proportional hazards model.
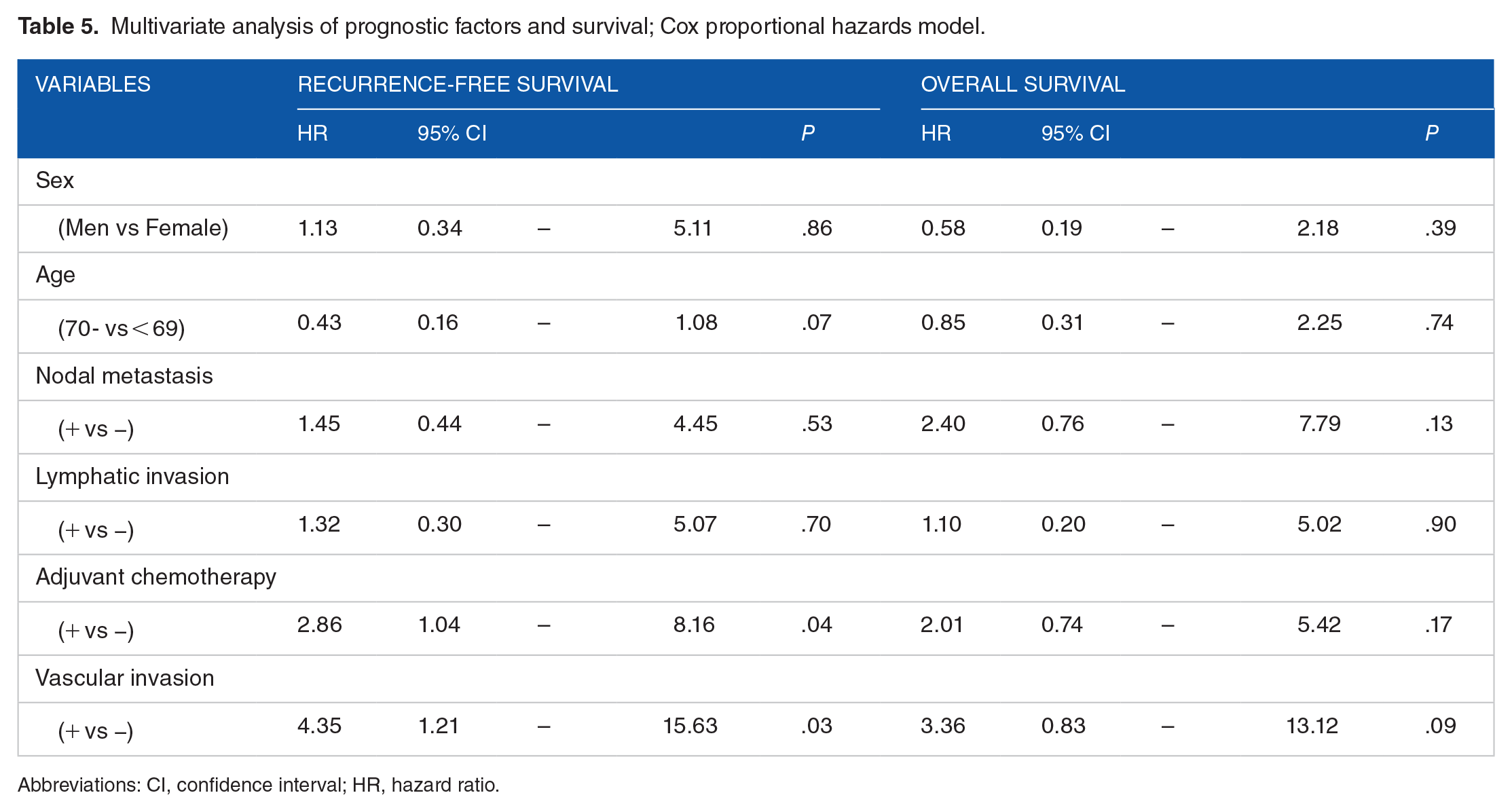
Abbreviations: CI, confidence interval; HR, hazard ratio.
Figure 2 shows RFS and OS according to the vascular invasion. Five-year RFS showed a lower survival in the vascular invasion positive group (positive 25.0%, negative 62.3%, P = .01; Figure 2A). Also, 5-year OS showed lower survival between the two groups (positive 16.2%, negative 63.4%, P = .01; Figure 2B).
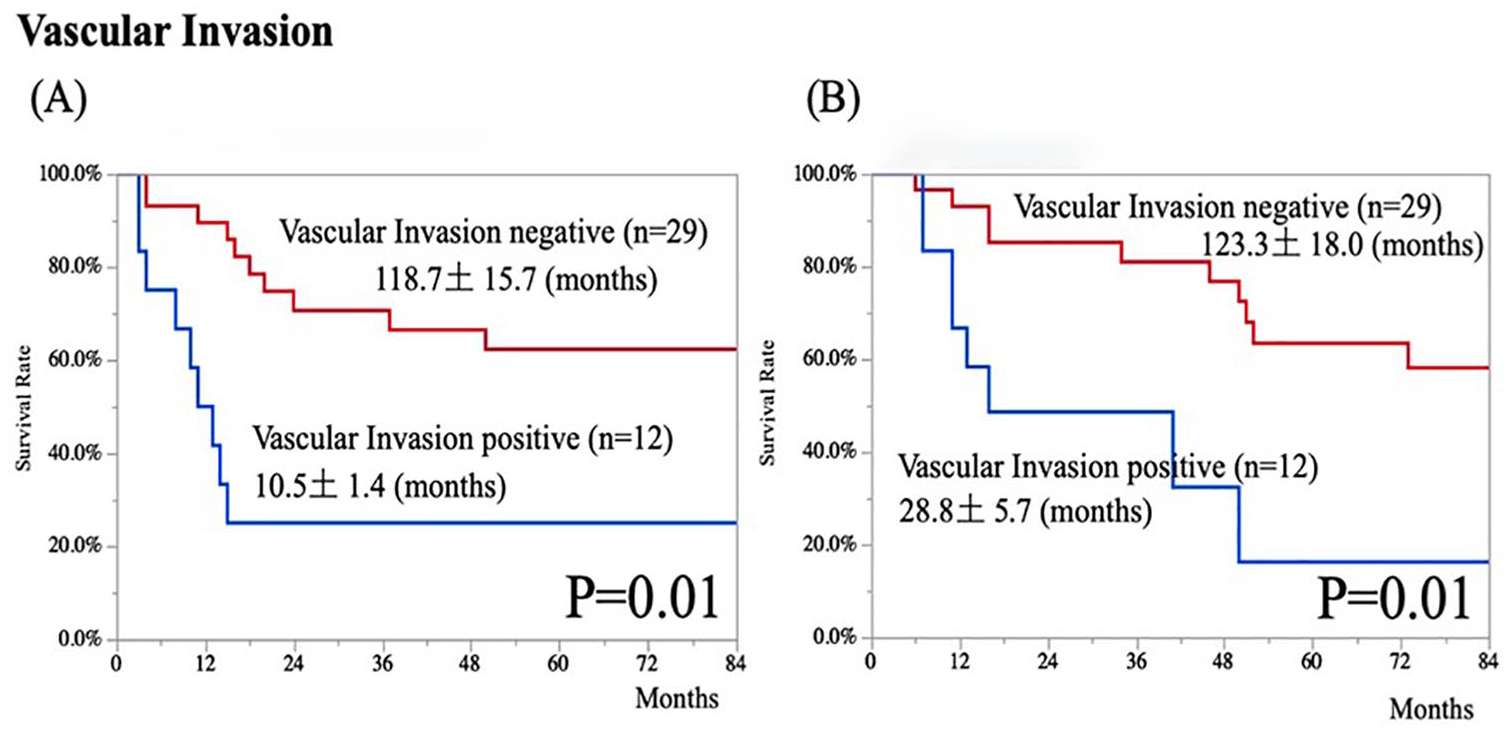
Recurrence-free survival (A) and overall survival (B) according to vascular invasion.
As shown in Figure 3, we evaluated RFS and OS according to the lymphatic invasion. Five-year RFS showed a lower survival in the lymphatic invasion positive group (positive 18.2%, negative 62.8%, P = .01; Figure 3A). Also, 5-year OS showed a lower survival between the two groups (positive 17.7%, negative 63.6%, P = .01; Figure 3B).

Recurrence-free survival (A) and overall survival (B) according to lymphatic invasion.
Figure 4 revealed RFS and OS according to the administration of adjuvant chemotherapy. Five-year RFS in the adjuvant chemotherapy-negative group was higher survival than in the positive group (69.6% and 26.7%, P = .02; Figure 4A). Although, 5-year OS showed no significant difference in OS, respectively (63.5% and 38.3%, P = .07; Figure 4B).

Recurrence-free survival (A) and overall survival (B) according to adjuvant chemotherapy.
Figure 5 shows RFS and OS according to the stratification of CDX2 expression. Five-year RFS in the CDX2-positive group and CDX2-negative group showed no significant difference (52.4% and 52.4%, respectively, P = .944; Figure 5A). Also, 5-year OS in the CDX2-positive group and CDX2-negative group showed no significant difference (51.8% and 56.4%, respectively, P = .81; Figure 5B).

Recurrence-free survival (A) and overall survival (B) according to CDX2 expression.
Discussion
LCNEC is a rare lung carcinoma.3-5 Due to its rarity, LCNEC’s understanding is largely based on a small number of retrospective studies or national database study.3,6-16 In these past studies, LCNEC has been reported to be a poor prognosis, as worse as SCLC. Even in the early stage I LCNEC, their 5-year OS reported in previous studies was 27% to 67%. 10 In our study, even in the operable patients, the 5-year RFS was 52.6%, whereas 5-year OS was 55.1% retrospectively. In the past, only a few had been discussed about the prognostic factors of LCNEC.17,27-30 As a prognostic factor, Asamura et al 17 reported completeness of resection, symptoms, nodal involvement, and age. On the other hand, Fournel et al 28 and Yeh et al 29 reported there was no significant factor related to the survival. As univariate analysis shows that, lymphatic invasion, vascular invasion, and adjuvant chemotherapy were worse prognostic factors related to RFS. Furthermore, lymphatic invasion and vascular invasion were worse prognostic factors of OS. In multivariate analysis, vascular invasion and adjuvant chemotherapy were negative prognostic factors. Studies discussing prognostic factors in large cell neuroendocrine carcinoma of lung are rare due to the rarity of this neoplasm. Therefore, our results provide new insights.
CDX2 is known as a transcription factor which has been playing a role in the development of small and large intestine in mammals and in differentiation of epithelial cells. 19 CDX2 is a factor normally associated with the development of midgut and hindgut. Generally, CDX2 is considered not expressed in the lungs, as it is an organ derived from the foregut. By utilizing the staining properties of CDX2, which has been used in clinical practice for at least over 20 years to distinguish primary lung cancer from metastatic lung cancer.19,22,26,30 In 2016, Dalerba et al 18 reported CDX2 as a prognostic factor for colorectal cancer. CDX2 which, when expressed in colorectal cancer, suppresses cancer growth. This mechanism has not yet been elucidated, and various studies are ongoing. In fact, only a few papers have reported on the expression of CDX2 in LCNEC.20-23 Bari et al 20 examined staining for CDX2 in LCNEC and reported that 56% of the lung were positive for CDX2. There are countless similar reports, with 30%–56% reporting CDX2 positivity.20-23 Our results follow the results of previous studies. Although we evaluated the correlation between CDX2 expression and clinicopathological factors, only age and tumor size were significant. These results may suggest that CDX2 was related to tumor growth.
However, this is the first study focused on a correlation with the prognosis between LCNEC and CDX2 expression. 18 We assumed that CDX2 might be a prognostic factor having the same characteristics of colorectal cancers. In our study, 32% (16/50) of the cases were positive for CDX2. By univariate analysis in our study has not shown any prognostic value of CDX2 staining with LCNEC histology. Whether CDX2 could be a prognostic factor, but it was not.
Lee et al 21 referred that there are borderline high-grade neuroendocrine carcinomas that morphologically fall between LCNEC and SCLC. Growing evidence suggests that LCNEC is a histologically and biologically heterogeneous group of tumors. Motoi 31 examined organ homology and prognostic factors for neuroendocrine tumors/cancer (NET/NEC), which occur in various organs, including LCNEC. In miRNA expression analysis, high-grade and low-grade NEC were separately grouped. Lungs and the gastrointestinal tract tended to have a common histology beyond the developing organ. In other words, this indicates that NETSs could be classified as a common disease unit regardless of the organ. Furthermore, our study and former studies suggest that the expression of CDX2 across organs may be one of the potential proofs of inter-organ homology in NETs.20-23
There has been a history of differentiating between metastatic lung tumors and primary lung cancer based on the presence or absence of CDX2 expression. However, according to this study, CDX-2 expression should not be used as the only criteria to exclude lung cancer origin in order to avoid clinical pitfalls.
It is thoroughly established in many studies that chemotherapy improves prognostic factors.3,6-15 On the other hand, some studies reported that chemotherapy did not affect the prognosis of LCNEC.32-34 Due to the small number of cases and the fact that most studies were retrospective, chemotherapy for LCNEC remains controversial.3,6-15,32-34 Reflecting this fact, adjuvant chemotherapy for LCNEC has not been determined in current guidelines.35,36 National Comprehensive Cancer Network (NCCN) guidelines suggest that LCNEC should be treated by the same regimens with NSCLC. 36 Even if we used both regimens, which have no significant differences, our result showed that adjuvant chemotherapy for LCNEC was a significantly unfavorable prognostic factor related to recurrence. Although our results differed from many previous studies, SEER-based study reported a similar survival curve of LCNEC with adjuvant chemotherapy. 37 Taken together, it may be harmful to apply by adjuvant chemotherapy using NSCLC regimens or both. Evaluation of the effects of chemotherapy on LCNEC requires a large number of patients. Large number of study population in LCNEC with or without adjuvant chemotherapy should be needed.
This study had some limitations. This study included only 50 patients in 4 institutions, and this could influence the results. Since this study is a retrospective and multi-institutional study, it cannot be guaranteed that the conditions are the same. Also, the improvement of surgical and multidisciplinary treatment techniques, the progress of chemotherapy over the target duration, must be considered. In adjuvant chemotherapy, administration of adjuvant chemotherapies, the choice of the regimen was also determined at the discretion of the attending physician. Performance bias and selection bias of patients may influence our results. It is thought that a large-scale study targeting more LCNEC patients is needed in the future.
In conclusion, this study evaluates the prognostic significance of CDX2 on LCNEC along with other known parameters. Similar to other known tumor types, vascular invasion was a significant prognostic factor. There was no prognostic significance of pulmonary LCNEC histology and CDX2 immunostaining. CDX2 is expressed in 32% of LCNEC but may not be a possible prognostic factor. Only vascular invasion was a possible recurrent marker for LCNEC patients. It is thought that a large-scale study targeting more LCNEC patients should be undertaken to clarify this hypothesis.
Footnotes
Acknowledgements
The authors appreciate the technical support of Ms. Yoko Miyanari. Also, Mr. Jacob Healy for his native English proofing support.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
I. Conception and design: SY,
II. Administrative support: KO, KN, SY
III. Provision of patients: KM, SA
IV. Collection and assembly of data: KM, SA, KI
V. Data analysis and interpretation: RM, SY
VI. Manuscript writing: All authors