
Abstract
OBJECTIVE:
The tripartite motif-containing protein (TRIM) family is involved in important biological processes such as the cell cycle, cell apoptosis, and innate immunity of virus. This study aimed to investigate TRIM66 expression and its predictive role in non-small cell lung cancer (NSCLC) patients.
METHODS:
We detected the expression levels of TRIM66 protein and TRIM66 mRNA in NSCLC tissues, and evaluated the prognostic role of TRIM66 in NSCLC.
RESULTS:
TRIMM66 was highly expressed in NSCLC tissues compared with normal paracancerous tissues (
CONCLUSION:
TRIM66 can be serve as an important molecular marker for predicting the prognosis in NSCLC patients.
Introduction
Lung cancer is associated with highest morbidity and mortality among all cancers, with approximately 1.2 million annual deaths worldwide [1]. Non-small cell lung cancer (NSCLC) accounts for over 80% of the total lung cancer cases. Most NSCLC patients are diagnosed at an advanced stage, and the postoperative 5-year survival rate for early NSCLC patients is low [2]. Therefore, investigating the pathogenesis of NSCLC and identifying new therapeutic targets for NSCLC are current research focuses.
The tripartite motif-containing protein (TRIM) family is involved in important biological processes such as the cell cycle, cell apoptosis, and innate immunity of virus [3, 4, 5]. In addition, TRIM is associated with the genesis and development of diseases, including tumorigenesis. TRIM family proteins can affect the sensitivity of tumor cells to chemotherapeutics [6]. TRIM protein 66 (TRIM66) is a member of the TRIM family [7], which is not only a participant in regulating protein expression but also in the malignant behavior of tumor cells. To our knowledge, TRIM66 is abnormally expressed in multiple malignant tumor tissues. However, studies on the correlation between TRIM66 expression and NSCLC are lacking. In this study, we determined the expression of TRIM66 in NSCLC tissues to preliminarily probe its association with the genesis, development, and malignancy grade of NSCLC.
Materials and methods
Patients
NSCLC and para-carcinoma tissue specimens were obtained from 130 patients (75 male and 55 female) who had undergone surgical resection in The First Hospital of Lanzhou University from May 2008 to August 2012 and with pathologic diagnosis of NSCLC. Complete clinical information was available for all patients; the average age of patients was 54.2
Immunohistochemistry
The streptavidin-peroxidase (SP) method was adop-ted for immunohistochemical analysis. Paraffin specimens were cut into slices (4
Single-blind review of sections was adopted in which the pathologists did not know of the corresponding clinical data. The Allred score was used by pathologist during evaluation of immunohistochemical staining [9]. Staining intensity was classified as follows: 0 point, no staining; 1 point, faint yellow staining; 2 points, claybank staining; and 3 points, brown staining. The proportion of nuclear positive cells was classified as 0–100%. In this study, the product of nuclear staining intensity and proportion of nuclear positive cells greater than 0 was considered as indicative of positive TRIM66 expression; otherwise, it was TRIM66 negative. Thus, TRIM66 staining intensities of 0 or 1 point and 2 or 3 points were deemed low and high expression, respectively. Immunohistochemical staining were evaluated with a double-headed microscope (Olympus, Tokyo, Japan).
Immunohistochemistry staining of TRIMM66 in NSCLC tissues and adjacent normal tissues. (A and B) lung squamous cell carcinoma; (C and D) lung adenocarcinoma; (E and F) normal adjacent lung tissues. (A, C and E) the TRIM66 located in the nuclei of tumor cells; (B, D and F) the TRIM66 located in the cytoplasm of tumor cells. Abbreviations: NSCLC, nonsmall cell lung cancer.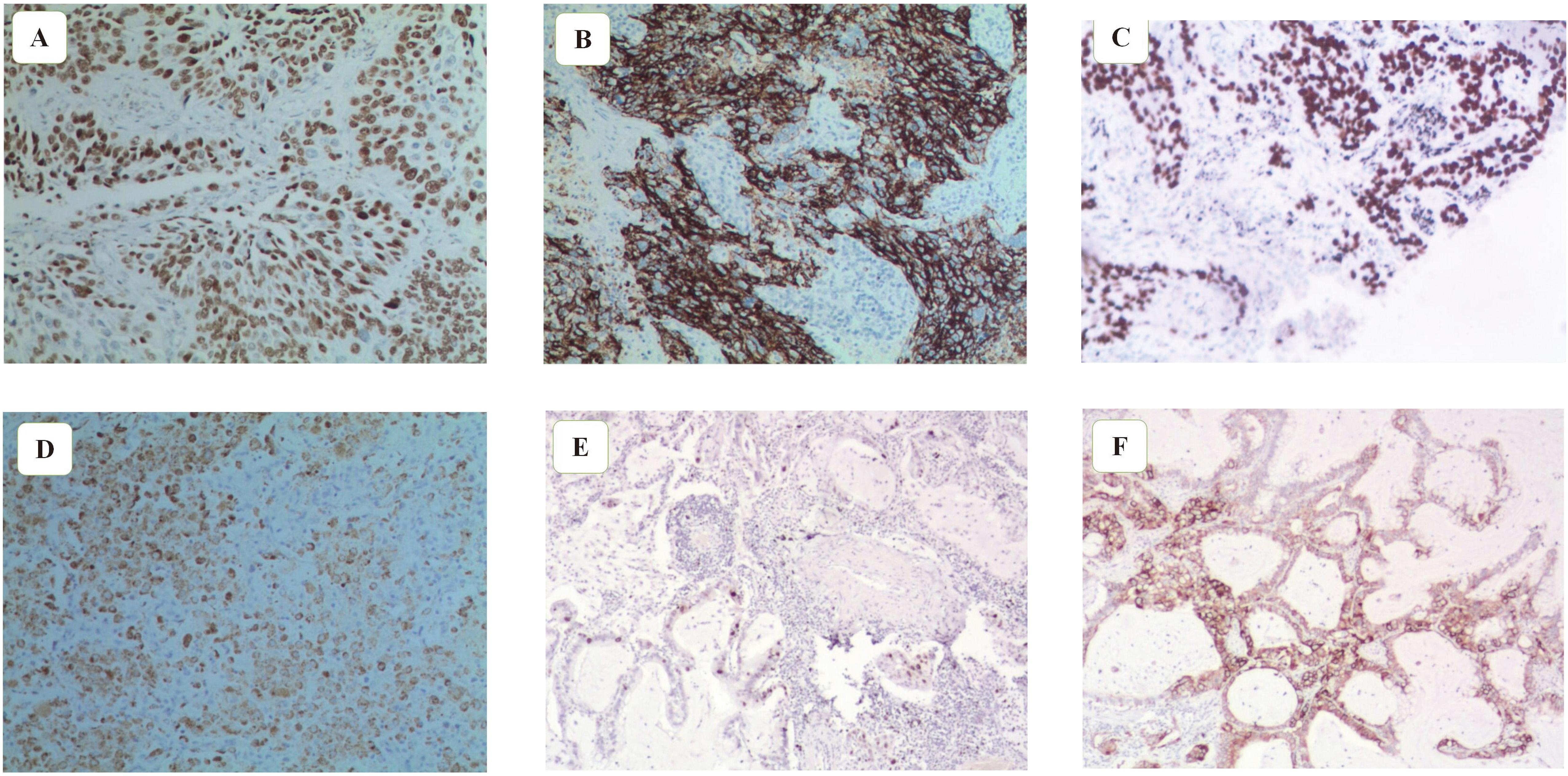
The TRIM66 mRNA was detected by RT-PCR. Abbreviations: T, tumor tissues; N, normal tissues; RT-PCR, Reverse transcription-polymerase chain reaction.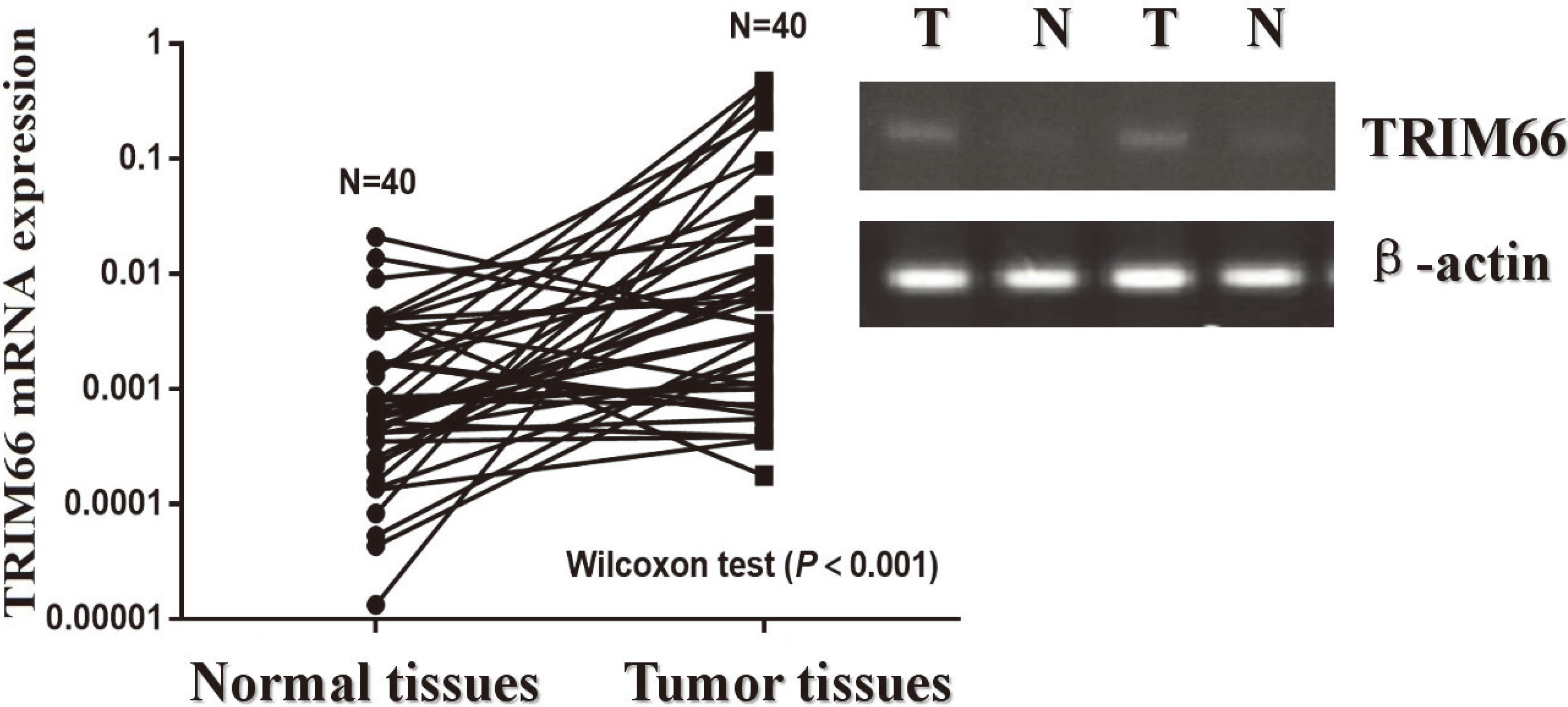
RNA was extracted in strict accordance with TRIzol (Life Technologies Corporation, Carlsbad, CA) instructions. RT of sample mRNA into cDNA was conducted, followed by PCR amplification. The reaction conditions were as follows: pre-degeneration at 94
Statistical methods
By using
Results
TRIMM66 expression in NSCLC tissues
Immunohistochemical results indicated that TRIM66 was mainly located in the nuclei of tumor cells, but TRIM66 staining could also be found in the cytoplasm of a few tumor cells (Fig. 1). Of the 130 NSCLC tissue samples, 75 showed high TRIM66 expression, which was remarkably higher than that found in para-carcinoma tissues (61.2% vs. 33.1%; Pearson
TRIM11 expression and clinicopathological features of NSCLC patients
Based on the immunohistochemical results, 130 cases of NSCLC patients were classified into the low or high TRIM66 expression groups. Simultaneously, the correlation between TRIM66 expression and clinicopathological characteristics of NSCLC patients was analyzed. The high TRIM66 expression closely associated with lymph node metastasis and TNM stage in NSCLC patients (
Correlation of clinicopathologic variables with TRIM66 in NSCLC
Correlation of clinicopathologic variables with TRIM66 in NSCLC
Abbreviations: SCC, squamous cell carcinoma; AD, adenocarcinoma; NSCLC, non-small cell lung cancer; TNM, tumor node metastasis.
Kaplan-Meier survival curves for disease-free survival of NSCLC patients based on TRIM66 expression.
Kaplan-Meier survival curves for overall survival of NSCLC patients based on TRIM66 expression.
Kaplan-Meier survival curves for overall survival of NSCLC patients based on lymph node status.
DFS and OS of NSCLC patients according to TRIM66 expression
DFS and OS of NSCLC patients according to TRIM66 expression
Abbreviations: NSCLC, non-small cell lung cancer; DFS, disease-free survival; OS, overall survival; Cl, confidence interval; SE, standard error.
Univariate and multivariate analysis for overall survival
Abbreviations: Cl, confidence interval; HR, hazard ratio.
Long-term follow-up was conducted in all NSCLC patients to probe the relation between TRIM66 expression and prognosis for NSCLC patients. The survival curve of the 130 NSCLC patients was drawn at the end of follow-up. Kaplan-Meier survival model indicated that DFS and OS of NSCLC patients in the high TRIM66 expression group were markedly lower than those in the low expression group (
TRIM family proteins possess three domains: RING finger, 1 or 2 B-box, and 1 coiled-coil region. Of them, B-box represents its characteristic domain, while coiled-coil region mainly plays a connective role [10]. Presently, 70 TRIM family members have been successively discovered [10, 11]. Structures of TRIM C-terminal differ from each other, which makes it possible for TRIM to specifically bind to different substrates [10, 12]. TRIM family proteins are further divided into 11 subfamilies, according to different C-terminal domains of TRIM [13, 14]. Most TRIM proteins mainly function as a ubiquitin E3 ligase, while a few TRIM proteins can serve as SUMO E3 ligase or other ubiquitin-like E3 ligases [15, 16]. Some TRIM proteins do not depend on their RING finger domains while functioning [17]. TRIM proteins are related to multiple human diseases, such as developmental disorders, neurodegenerative diseases, viral infections, and cancer [4, 15, 18, 19, 20, 21, 22, 23]. An increasing number of studies have found that TRIM family proteins are related to the genesis, development, and prognosis of tumors.
Abnormal TRIM expression is closely related to the genesis and development of NSCLC. For instance, expression of TRIM29 is upregulated in NSCLC tissues, and high TRIM29 expression indicates poorer prognosis in NSCLC patients [24]. In human lung squamous carcinoma NCI-H520 cells, silencing TRIM29 expression through siRNA contributes to inhibiting the proliferation and invasion of tumor cells [25]. Zhan et al. discovered that TRIM59 could be highly expressed in multiple lung cancer cell lines, and the knockout of TRIM59 gene affected the expression of cyclin (including CDC25C and CDK1), thus promoting the proliferation and migration of lung cancer cells [26]. Expression of TRIM44 was upregulated in lung cancer A549 and H441 cells, which could remarkably enhance the migration and invasion abilities of tumor cells, as was suggested in a series of experiments carried out by Luo et al. [27]. In addition, they also found that TRIM44 could upregulate the expression of CXCL16 and MMP9 through activating the NF-
It was also discovered that, compared with normal human bronchial epithelial cells, expression of TRIM66 is upregulated in all NSCLC cell lines [26]. However, this finding was based on an in vitro study, and the expression of TRIM66 in vivo remains unknown. Taking the previously stated reasons into consideration, expression of TRIM66 in NSCLC tissue is detected by an immunohistochemical method. We observed that TRIM66 expression was mainly limited to the nucleus of NSCLC tumor cells. Moreover, the results of statistical analysis reconfirmed the high expression of TRIM66 in NSCLC tumor cells. Secondly, RT-PCR results also indicated that TRIM66 mRNA content in NSCLC tissue was notably higher than in para-carcinoma tissue. Further, we also found that TRIM66 expression level was closely associated with clinicopathological characteristics such as lymph node metastasis and TNM stage, suggesting that TRIM66 may promote the growth, proliferation, and invasion of NSCLC tumor cells. A long-term follow-up of 130 NSCLC patients was carried out; the results of which demonstrated that NSCLC patients with high TRIM66 expression have shorter survival time than those with low TRIM66 expression. The multivariate analysis showed that high TRIM66 expression is one of the important indicators for independently predicting a poorer prognosis in NSCLC patients. We can speculate, based on these results, that TRIM66 expression is closely associated with the genesis and development of NSCLC and the malignancy grade of NSCLC may be positively correlated with TRIM66 expression.
Taken together, our findings suggest that high TRIM66 expression indicates poorer prognosis in NSCLC patients, and thus, TRIM66 can be serve as an important molecular marker for predicting the prognosis in NSCLC patients. However, this study is limited by its design as a clinical observational study, and the precise mechanism concerning TRIM66 remains unclear, which will require further investigation in future studies. A foundation for the further investigation of the molecular mechanism of TRIM has been established in this study. We believe that blocking TRIM-related signal transduction pathway contributes to achieving the goals of delaying tumor growth, proliferation, invasion, and metastasis.
Conflict of interest
The authors report no conflicts of interest in this work.
Funding statement
This study was funded by grants from Section Development Fund.