: The 14-3-3 family of conserved regulatory proteins comprises the isoforms beta (), gamma (), zeta (), sigma (), tau (), and delta (), which are overexpressed and associated with a high risk of metastasis and poor survival in hepatocellular carcinoma (HCC). In the present study, we investigated whether serum 14-3-3 isoforms are related to HCC progression and patient survival.
METHODS
: Serum samples from 63 HCC patients who underwent surgical reSection 104 HCC patients who received non-surgical anti-HCC treatments, 50 patients with liver cirrhosis alone, 45 patients with chronic hepatitis alone, and 50 healthy subjects were collected between January 2006 and December 2010. Serum levels of 14-3-3 (, , , , and ) isoforms were measured by ELISA. The correlation between 14-3-3 ( and ) isoforms and clinicopathological factors was examined by logistic regression analysis. The feasibility of serum 14-3-3 for discriminating HCC patients was assessed by ROC curve analysis. Patient survival analyses were performed by Kaplan-Meier analyses and Cox regression models.
RESULTS:
Serum levels of 14-3-3 ( and ) were significantly higher in HCC patients than in those with liver cirrhosis, chronic hepatitis, and healthy subjects ( 0.05). There was no difference in the serum levels of 14-3-3 , , and between HCC and the other groups ( 0.05). High levels of serum 14-3-3 were associated with vascular invasion ( 0.016), TNM stage ( 0.012), BCLC stage ( 0.01), and early recurrence ( 0.013). Patients with high levels of serum 14-3-3 had a poor prognosis. There was no significant association between 14-3-3 levels and clinicopathological parameters. A significant independent association between serum 14-3-3 and HCC was observed by univariate and multivariate analysis ( 0.05). Serum 14-3-3 could effectively discriminate HCC patients at a cut-off point of 18.7 ng/mL, with 91.4% sensitivity and 75.3% specificity.
CONCLUSIONS
: Serum 14-3-3 is a potential biomarker for the diagnosis of early-stage HCC, and high levels of serum 14-3-3 were associated with metastasis and poor prognosis in HCC.
Hepatocellular carcinoma (HCC) is the fifth most common cancer and the second leading cause of cancer-related death worldwide. Although the prognosis of patients with HCC is generally poor, the 5-year survival rate is 70% in patients diagnosed at an early stage [1]. However, the early diagnosis of HCC is complicated by the coexistence of inflammation and cirrhosis. Therefore, the identification of novel biomarkers for the early diagnosis of HCC is important.
The diagnosis of HCC without pathologic confirmation can be achieved by assessing the levels of serum alpha-fetoprotein (AFP) in combination with imaging techniques, including ultrasonography, magnetic resonance imaging, and computerized tomography [2, 3]. However, improvements in early diagnosis are needed because only 44% of the patients are diagnosed at a localized disease stage, and only 30% of patients with HCC are candidates for potentially curative treatments at the time of diagnosis [4]. A marker for early diagnosis would meet the following requirements: first, it should have high accuracy, which would increase the probability of making a diagnosis before the cancer has spread and thus increase the cure rate; second, specimen collection for marker detection should be an easy and non-invasive procedure; and third, the cost-effectiveness should be considered [5]. The current gold standard and most commonly used biomarkers for patients at risk for HCC are AFP and ultrasound every 6–12 months; however, this is far from perfect. Serum AFP levels 400 ng/mL are considered diagnostic; however, such high values are observed only in a small percentage of patients with HCC. Therefore, the discovery of an effective and reliable tool for the early diagnosis of HCC is important to increase the number of patients who are eligible for curative treatment and to improve the prognosis of patients with HCC.
The 14-3-3 family of conserved regulatory proteins consists of seven isoforms: , , , , , , and . Studies indicate that the 14-3-3 , 14-3-3 , 14-3-3 , 14-3-3 , and 14-3-3 isoforms are overexpressed in HCC [1, 6]. Increased 14-3-3 expression is associated with poor overall and progression-free survival in HCC, and 14-3-3 overexpression significantly correlates with extrahepatic metastasis [8]. Increased 14-3-3 stimulates cell proliferation and tumor formation [11], whereas knockdown of 14-3-3 reduces rat hepatoma cell proliferation and tumor growth [12]. The 14-3-3 and 14-3-3 isoforms are abundantly expressed and significantly associated with poor survival rates and a high risk of HCC metastasis [7, 8]. 14-3-3 is overexpressed in hepatoma cell lines and in tumors from HCC patients, whereas silencing of 14-3-3 by RNA interference suppresses tumor cell proliferation [13]. 14-3-3 plays a “bipolar” role in HCC. It has been reported that expression of 14-3-3 is correlated with histological grade and micro-vascular thrombi of HCC [14]. These results suggest that 14-3-3 contributes to facilitating HCC cancer cell migration and invasion.
Elevated serum 14-3-3 levels have been observed in many diseases, including inflammatory polyarthritis [15], eosinophilic meningitis [16], gastric cancer [17], vulvar squamous cell carcinoma [18], and breast cancer [19]. Increased serum levels of 14-3-3 may be associated with aggressive tumor growth and poor survival [17, 19]. The aims of the present study were to determine serum 14-3-3 levels and to assess the association between serum 14-3-3 levels and clinical significance.
Serum 14-3-3 levels assay
Groups
Serum 14-3-3 levels (ng/mL)
14-3-3
14-3-3
14-3-3
14-3-3
14-3-3
HCC (surgical)
63
96.4 13.5
5.9 1.4
58.5 8.7
6.9 1.7
24.9 5.4
HCC (non-surgical)
104
109.8 20.3
6.3 1.6
65.3 9.4
7.8 2.1
28.3 8.2
Liver cirrhosis
50
20.4 3.6
4.1 0.9
10.3 1.5
4.24 1.6
21.0 4.8
Chronic hepatitis
45
30.7 6.6
5.8 1.2
19.6 4.7
3.16 0.7
26.4 5.3
Healthy controls
50
18.2 4.4
3.6 0.8
9.4 1.2
2.78 0.9
17.4 7.3
Vs healthy controls, 0.05, 0.05 (Student’s test).
Patients and methods
Patients and specimens
All serum samples were collected from the central hospital of Linyi. This study was approved by the independent Institutional Review Board (IRB) of the central hospital of Linyi and conformed to the 1975 Helsinki declaration ethical guidelines. Our exclusion criteria were as follows: 1) previous history of anti-HCC treatment, 2) pathological or radiological evidence of mixed HCC-cholangiocellular carcinoma, 3) insufficient clinical data, and 4) insufficient serum samples. Serum samples from 63 patients with HCC who underwent surgical resection, 104 patients who received non-surgical anti-HCC treatments (chemotherapy, radiotherapy, ablation, and conservative care), 50 patients with liver cirrhosis alone, 45 patients with chronic hepatitis alone, and 50 healthy subjects with no evidence of viral hepatitis [HBV surface antigen (HBsAg) and HCV antibody negative and normal liver biochemistry] were collected between January 2006 and December 2010.
Diagnosis and grading of HCC and liver cirrhosis
HCC diagnosis was made based on the following criteria: 1) pathological HCC diagnosis for patients who underwent surgical resection or percutaneous biopsy or 2) clinical and radiological HCC diagnosis for patients without available HCC tissue specimens, based on the guidelines of the American Association for the Study of Liver Diseases [20]. In the surgical resection cases, Tumor-Node-Metastasis (TNM) staging based on the American Joint Commission on Cancer (7 edition) was assessed postoperatively [21]. Otherwise, HCC stage was clinically defined according to the Barcelona Clinic Liver Cancer (BCLC) staging system [22]. For this study, early-stage HCC was defined as HCCs with TNM I–II and BCLC A–B. Liver cirrhosis was histologically or clinically diagnosed as follows: 1) platelet count 100000/L and ultrasonographic findings suggestive of cirrhosis, including a blunted, nodular liver edge accompanied by splenomegaly ( 12 cm), esophageal or gastric varices, or overt liver cirrhosis complications, including ascites, variceal bleeding, and hepatic encephalopathy [23].
Correlation of serum 14-3-3 with clinicopathological parameters
14-3-3
Characteristics
No
Low
High
Age (years)
0.48
50/ 50
29/34
11(38%)/13(38%)
18(62%)/21(62%)
Gender
0.54
Female vs. male
10/53
4(40%)/20(37.7%)
6(60%)/33(62.3%)
Tumor size (cm)
0.07
5/ 5
48/15
19(39.5%)/5(33.3%)
29(60.5%)/10(66.7%)
Tumor number
0.18
Single/Multiple
52/11
19(36.5%)/5(45%)
33(63.5%)/6(55%)
Tumor capsule
0.24
Incomplete/Complete
42/21
15(35.7%)/9(42.8%)
27(64.3%)/12(57.2%)
Differentiation
0.08
I–II/III–IV
43/20
16(37%)/8(40%)
27(63%)/12(60%)
Vascular invasion
0.02
Yes/No
16/47
3(18.7%)/13(27.6%)
13(81.3%)/26(72.4%)
TNM stage
0.01
I–II/III
50/13
24(48%)/3(23%)
26(52%)/13(77%)
BCLC stage
0.01
A–B/C
47/16
19(40%)/5(31%)
28(60%)/11(69%)
Early recurrence
0.01
Yes/No
14/49
6(42.8%)/8(16.3%)
8(57.2%)/41(83.7%)
0.05 indicates a significant difference ( test).
Serum sample analysis
Peripheral blood samples collected into anticoagu- lant-free tubes were centrifuged and stored at 70C prior to testing. An experienced researcher at Yuhuang- ding Hospital performed the assays for serum 14-3-3. This individual had no access to the patients’ clinical information. The isoform-specific anti-14-3-3 antibodies 14-3-3 (A-6) (sc-25276), 14-3-3 (L-17) (sc-31957), 14-3-3 (E-20) (sc-31962), 14-3-3 (K-12) (sc-17286), and 14-3-3 (C-18) (sc-7683) were from Santa Cruz Biotechnologies Inc. (Shanghai, China). Serum 14-3-3 (, , , , and ) levels were measured using the corresponding quantitative 14-3-3 ELISA kits according to the manufacturer’s recommendations. Positivity for 14-3-3 , 14-3-3 , 14-3-3 , 14-3-3 , and 14-3-3 was defined by the manufacturer at 0.19, 0.76, 0.43, 0.04, and 0.03 ng/mL, respectively. All measurements were performed in triplicate.
Statistical analysis
Statistical analysis was performed with JMP 10.0.0 (SAS Institute Inc., NC) and data are presented as the mean S.E. tests were used to evaluate the relationship between protein expression and clinicopathological variables. The statistical significance of differences between continuous and categorical variables was examined using the Student’s t-test or chi-squared test. The receiver operating characteristic curve (ROC) was plotted to assess the diagnostic accuracy. The relationship of the true positivity (sensitivity) and the false positivity (1-specificity) was plotted. The Kaplan-Meier analysis was used to assess survival, and differences in survival probabilities were estimated using the log-rank test. The Cox proportional hazards model was used to determine the independent factors of survival. Hazard ratios (HRs) and the corresponding 95% confidence intervals (CIs) for PFS and OS were estimated using univariate and multivariate analysis with the Cox proportional hazards model. 0.05 was considered statistically significant.
Results
Serum 14-3-3 levels
Serum 14-3-3 (, , , , and ) levels were analyzed in patients with HCC from the following subgroups: 63 patients who underwent surgical resection, 104 patients who received non-surgical anti-HCC treatments, 50 liver cirrhosis alone, 45 chronic hepatitis alone, and 50 healthy subjects. The median 14-3-3 level is shown in Table 1. 14-3-3 and 14-3-3 levels were significantly higher in patients with HCC than in healthy controls ( 0.05, Student’s test). 14-3-3 and 14-3-3 levels were higher in patients with non-surgical anti-HCC treatments; however, the difference was not statistically significant. Although 14-3-3 , 14-3-3 , and 14-3-3 levels were higher in patients with HCC than in healthy controls and patients with liver cirrhosis and chronic hepatitis, the difference did not reach statistical significance ( 0.05, Student’s test) (Table 1). Therefore, 14-3-3 and 14-3-3 were selected for further investigation.
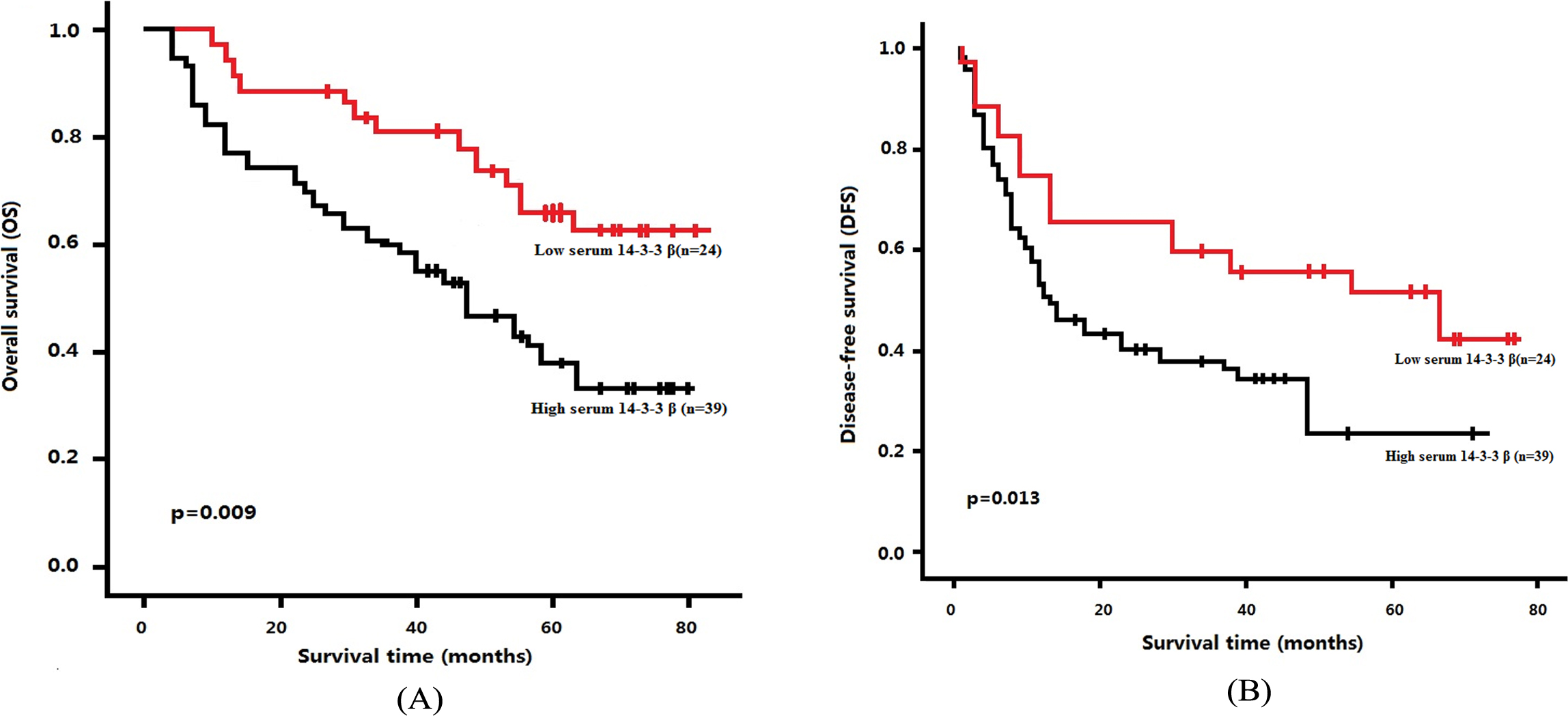
Kaplan-Meier curves for patients with HCC. (A) OS and (B) DFS curves for the two groups defined using low and high serum 14-3-3 levels in patients with HCC. Low serum 14-3-3 levels indicated better overall survival and disease-free survival of patients with HCC.
Correlation between serum 14-3-3 ( and ) and clinicopathological parameters
Because serum 14-3-3 ( and ) levels were significantly higher in patients with HCC than in healthy controls and there was no significant difference between non-surgical anti-HCC treatments and surgical HCC treatments, we investigated the correlation between serum 14-3-3 ( and ) and clinicopathological parameters in 63 patients who underwent surgical resection. Serum 14-3-3 and 14-3-3 levels were 18.2 4.4 (median 15.3, range 0.46–28.7) ng/mL and (median 7.3, range 0.39–19.7) ng/mL, respectively. We defined serum 14-3-3 15.3 ng/mL as 14-3-3 low expression and serum 14-3-3 7.3 ng/mL as 14-3-3 low expression. Of the 63 patients who underwent surgical reSection 24 were 14-3-3 -low and 39 patients were 14-3-3 -high. In addition, 19 patients were 14-3-3 -low and 44 patients were 14-3-3 -high.
Univariate and multivariate analysis of overall survival(OS) in HCC
Univariate analysis
Multivariate analysis
HR
95% CI
HR
95% CI
Variables
Gender (female vs. male)
0.83
0.53–1.73
0.47
Age, years ( 50 vs. 50)
0.48
0.28–1.42
0.72
Tumor size (cm) ( 5 vs. 5)
1.26
0.94–2.13
0.18
Tumor number (single vs. multiple)
2.43
1.38–3.57
0.07
Satellite nodule (no vs. yes)
1.37
0.82–1.94
0.08
Tumor capsule (no/incomplete vs. complete)
0.84
0.63–1.92
0.26
Tumor differentiation (I–II vs. III–IV)
1.56
1.15–2.28
0.11
Vascular invasion (No vs. Yes)
3.20
1.83–5.48
0.001
2.46
1.79–3.84
0.06
14-3-3 (Low versus High)
0.36
0.28–0.73
0.001
0.62
0.94–1.06
0.03
TNM stage (I–II vs. III)
2.18
1.24–3.52
0.001
1.79
1.28–3.76
0.01
BCLC stage (A–B/C)
1.97
1.10–3.18
0.001
1.743
1.25–3.84
0.02
Early recurrence (yes/no)
1.54
1.26–2.34
0.07
Univariate and multivariate analysis of disease-free survival (DFS) in HCC
Univariate analysis
Multivariate analysis
HR
95% CI
HR
95% CI
Variables
Gender (female vs. male)
1.26
0.65–1.83
0.47
Age, years ( 50 vs. 50)
0.98
0.45–1.56
0.72
Tumor size (cm) ( 5 vs. 5)
1.03
0.94–2.13
0.18
Tumor number (single vs. multiple)
1.54
1.27–2.86
0.07
Satellite nodule (no vs. yes)
1.15
0.89–1.34
0.08
Tumor capsule (no/incomplete vs. complete)
1.63
1.21–2.25
0.26
Tumor differentiation (I–II vs. III–IV)
1.04
0.85–1.53
0.11
Vascular invasion (no vs. yes)
1.83
1.44–2.94
0.17
14-3-3 (low versus high)
1.58
1.24–2.86
0.01
0.62
0.94–1.06
0.03
TNM stage (I–II vs. III)
1.15
0.96–2.32
0.28
BCLC stage (A–B/C)
1.35
1.14–2.29
0.14
Early recurrence (yes/no)
1.63
1.28–2.66
0.21
High expression of serum 14-3-3 was associated with vascular invasion ( 0.016), TNM stage ( 0.012), BCLC stage ( 0.01), and early recurrence ( 0.013) (Table 2). No significant correlation was observed between serum 14-3-3 level and age, gender, tumor size, and tumor differentiation (Table 2). No significant association was found between serum 14-3-3 level and clinicopathological parameters (data not shown).
ROC curves of serum 14-3-3 in diagnosing early-stage HCC.
Relationship between serum 14-3-3 and survival
The prognostic value of serum 14-3-3 for survival was evaluated by comparing patients with high and low serum 14-3-3 levels. The median OS and DFS was 49 and 23 months, respectively, in patients with low serum 14-3-3 levels compared with 34 and 13 months, respectively, in patients with high serum 14-3-3 levels. The OS rates at 1, 3, and 5 years were 93.8%, 72.4%, and 60.6%, respectively, in patients with low serum 14-3-3 levels compared with 80.2%, 53.4%, and 41.6%, respectively, in patients with high serum 14-3-3 (log-rank test, 0.009). The DFS rates at 1, 3, and 5 years were 63.4%, 52.4%, and 49.3%, respectively, in patients with low serum 14-3-3 level compared with 52.3%, 39.4%, and 24.7%, respectively, in patients with high serum 14-3-3 levels (log-rank test, 0.013) (Fig. 1). These results indicated that high serum 14-3-3 levels were significantly associated with poor prognosis in patients with HCC.
Univariate and multivariate analyses were performed to examine the effect of serum 14-3-3 level on HCC prognosis using a Cox proportional hazard model. Serum 14-3-3 levels were significantly correlated with improved OS and DFS in HCC patients by univariate analysis (Table 3). Multivariate Cox regression analysis further indicated that serum 14-3-3 level was an independent predictor of OS and DFS (Table 4). Accordingly, serum 14-3-3 level may be useful for predicting survival in patients with HCC.
Diagnostic accuracy of serum 14-3-3 in HCC
According to the ROC curve, the serum 14-3-3 cutoff value was calculated as 18.7 ng/mL. Comparing low and high serum 14-3-3 levels in patients with HCC, the AUC of the ROC curve was 0.798 (95% CI, 0.617–0.859; 0.0015) (Fig. 2). The sensitivity was 91.4%, and the specificity was 75.3%, suggesting that the detection of serum 14-3-3 levels could provide a new complementary tumor marker for HCC diagnosis.
Discussion
HCC, the neoplastic transformation of hepatocytes, is one of the leading causes of cancer-related death worldwide. People at risk of developing HCC include chronic liver disease patients with hepatitis B or C, obese or diabetic people, and heavy drinkers [24]. HCC develops from chronic liver cirrhosis, in which a decrease in hepatocyte growth and proliferation occurs along with scar tissue formation, providing a platform for neoplastic tumor growth. Current methods of HCC management and treatment are tumor oriented (chemotherapy, radiotherapy, surgical methods such as liver resection and transplantation, and ethanol injection into tumor cells) [25]. However, these methods constitute a palliative approach to HCC, and aim to extend the lifespan of patients rather than devising a curative approach. The lack of a proper curative treatment for HCC underscores the importance of preventing the onset of HCC and detecting the disease at an early stage.
Selective 14-3-3 isoforms are overexpressed in HCC and are potential prognostic markers for HCC. 14-3-3 isoforms contribute to migration/invasion and are associated with a high risk of HCC extrahepatic metastasis [13, 19]. Overexpression of 14-3-3 proteins is thus a potential effector and can serve as a diagnostic marker for the more malignant types of HCC. Tseng et al. reported that elevated serum 14-3-3 levels are highly correlated with the number of lymph node metastases, tumor size, and a reduced survival rate, suggesting the potential of 14-3-3 level as a diagnostic and prognostic biomarker in gastric cancer [17]. In the present study, we specifically analyzed the value of serum 14-3-3 isoforms as diagnostic markers for the more malignant types of HCC. Our results showed that serum 14-3-3 and 14-3-3 levels were significantly higher in patients with HCC than in those with liver cirrhosis, chronic hepatitis alone, and in healthy subjects. The levels of serum 14-3-3 , , and did not differ significantly between the HCC group and the other groups. These results suggested that the serum levels of 14-3-3 isoforms were not consistent with the levels in HCC tissues.
We next analyzed whether serum 14-3-3 and 14-3-3 levels could serve as diagnostic markers in patients with HCC. 14-3-3 has been implicated in modulating cell proliferation, migration, and tumor growth in HCC [26]. The expression of 14-3-3 is elevated in HCC tumors and significantly associated with distant metastasis, whereas only rare incidences of metastasis are found in 14-3-3 -negative HCC patients [26]. These results suggest that 14-3-3 plays an important role in promoting migration, invasion, and metastasis in patients with HCC. In our study, high serum 14-3-3 levels were associated with vascular invasion, TNM stage, BCLC stage, and early recurrence. Therefore, serum 14-3-3 is a potential prognostic marker to predict the clinical outcomes of HCC.
14-3-3 plays a “bipolar” role in HCC. Despite the frequent occurrence of 14-3-3 hypermethylation [27], high 14-3-3 expression was reported in tissues from patients with HCC [28]. The expression of 14-3-3 is correlated with histological grade and micro-vascular thrombi in HCC [28]. In our study, although serum14-3-3 level was increased in HCC patients, there was no significant association between 14-3-3 levels and clinicopathological parameters. Liu et al. [12] showed that increased 14-3-3 expression in primary tumors predicts a high 5-year cumulative incidence of subsequent extrahepatic metastasis, and multivariate analysis identified 14-3-3 overexpression as an independent risk factor for extrahepatic metastasis. Patients with increased 14-3-3 expression in primary tumors had worse 5-year OS rates, and 14-3-3 overexpression was an independent prognostic factor on Cox regression analysis. In our study, high serum 14-3-3 levels were associated with low 1-, 3-, and 5-year survival rates. A significant independent association between serum 14-3-3 and HCC was observed by univariate and multivariate analyses. Serum 14-3-3 could effectively discriminate HCC patients with 91.4% sensitivity and 75.3% specificity. Therefore, serum 14-3-3 may be a potential biomarker for diagnosing early-stage HCC.
In summary, the results of our study indicate that high serum 14-3-3 levels are associated with metastasis and poor prognosis in patients with HCC, and may be a potential biomarker for diagnosing early-stage HCC. These results support that targeting 14-3-3 may be a beneficial strategy for the treatment of HCC, and the 14-3-3 protein is a promising prognostic marker and therapeutic target in HCC.
References
1.
SiegelR.NaishadhamD. and JemalA., Cancer statistics, 2013, CA Cancer J Clin63(1) (2013), 11–30.
2.
TrinchetJ.C.ChaffautC.BourcierV.DegosF.HenrionJ.FontaineH.RoulotD.MallatA.HillaireS.CalesP.OllivierI.VinelJ.P.MathurinP.BronowickiJ.P.VilgrainV.N’KontchouG.BeaugrandM. and ChevretS., Ultrasonographic surveillance of hepatocellular carcinoma in cirrhosis: A randomized trial comparing 3- and 6-month periodicities, Hepatology54(9) (2011), 1987–1997.
3.
AghoramR.CaiP. and DickinsonJ.A., Alpha-foetoprotein and/or liver ultrasonography for screening of hepatocellular carcinoma in patients with chronic hepatitis B, Cochrane Database Syst Rev9(4) (2012), CD002799.
4.
BruixJ. and LlovetJ.M., Prognostic prediction and treatment strategy in hepatocellular carcinoma, Hepatology35(3) (2002), 519–524.
5.
McShaneL.M.AltmanD.G.SauerbreiW.TaubeS.E.GionM. and ClarkG.M., Reporting recommendations for tumor marker prognostic studies (REMARK), J Natl Cancer Inst97(16) (2005), 1180–1184.
6.
TzivionG.GuptaV.S.KaplunL. and BalanV., 14-3-3 proteins as potential oncogenes, Semin Cancer Biol16(3) (2006), 203–213.
7.
TzivionG. and AvruchJ., 14-3-3 proteins: Active cofactors in cellular regulation by serine/threonine phosphorylation, J Biol Chem277(5) (2002), 3061–3064.
8.
LiZ.ZhaoJ.DuY.ParkH.R.SunS.Y.Bernal-MizrachiL.AitkenA.KhuriF.R. and FuH., Down-regulation of 14-3-3 zeta suppresses anchorage-independent growth of lung cancer cells through anoikis activation, Proc Natl Acad Sci U S A105(1) (2008), 162–167.
9.
NealC.L.YaoJ.YangW.ZhouX.NguyenN.T.LuJ.DanesC.G.GuoH.LanK.H.EnsorJ.HittelmanW.HungM.C. and YuD., 14-3-3 zeta overexpression defines high risk for breast cancer recurrence and promotes cancer cell survival, Cancer Res69(8) (2009), 3425–3432.
10.
KoB.S.ChangT.C.HsuC.ChenY.C.ShenT.L.ChenS.C.WangJ.WuK.K.JanY.J. and LiouJ.Y., Overexpression of 14-3-3 ε predicts tumour metastasis and poor survival in hepatocellular carcinoma, Histopathology58(5) (2011), 705–711.
11.
KoB.S.LaiI.R.ChangT.C.LiuT.A.ChenS.C.WangJ.JanY.J. and LiouJ.Y., Involvement of 14-3-3 γ overexpression in extrahepatic metastasis of hepatocellular carcinoma, Hum Pathol42(1) (2011), 129–135.
12.
LiuT.A.JanY.J.KoB.S.ChenS.C.LiangS.M.HungY.L.HsuC.ShenT.L.LeeY.M. and ChenP.F., Increased expression of 14-3-3β promotes tumor progression and predicts extrahepatic metastasis and worse survival in hepatocellular carcinoma, Am J Pathol179(6) (2011), 2698–2708.
13.
ChoiJ.E.HurW.JungC.K.PiaoL.S.LyooK.HongS.W.KimS.W.YoonH.Y. and YoonS.K., Silencing of 14-3-3 ζ over-expression in hepatocellular carcinoma inhibits tumor growth and enhances chemosensitivity to cis-diammined dichloridoplatium, Cancer Lett303(5) (2011), 99–107.
14.
Shiba-IshiiA.KanoJ.MorishitaY.SatoY.MinamiY. and NoguchiM., High expression of stratifin is a universal abnormality during the course of malignant progression of early-stage lung adenocarcinoma, Int J Cancer129(10) (2011), 2445–2453.
15.
CarrierN.MarottaA.de Brum-FernandesA.J.LiangP.MasettoA.MénardH.A.MaksymowychW.P. and BoireG., Serum levels of 14-3-3 η protein supplement C-reactive protein and rheumatoid arthritis-associated antibodies to predict clinical and radiographic outcomes in a prospective cohort of patients with recent-onset inflammatory polyarthritis, Arthritis Res Ther18(7) (2016), 37.
16.
TsaiH.C.HuangY.L.ChenY.S.YenC.M.TsaiR.LeeS.S. and TaiM.H., 14-3-3 β protein expression in eosinophilic meningitis caused by Angiostrongylus cantonensis infection, BMC Res (7) (2014), 97.
17.
TsengC.W.YangJ.C.ChenC.N.HuangH.C.ChuangK.N.LinC.C.LaiH.S.LeeP.H.ChangK.J. and JuanH.F., Identification of 14-3-3 β in human gastric cancer cells and its potency as a diagnostic and prognostic biomarker, Proteomics11(8) (2011), 2423–2439.
18.
WangZ.H.JahnM.SuoZ.H.ClaesG. and TropeR.H., The prognostic value of 14-3-3 isoforms in vulvar squamous cell carcinoma cases: 14-3-3 β and ε are independent prognostic factors for these tumors, PLoS One6(9) (2011), e24843.
19.
ChristopherL.YaoJ.YangW.T.ZhouX.Y.NguyenN.T.LuJ.DanesC.G. and YuD.H., 14-3-3 ζ overexpression defines high risk for breast cancer recurrence and promotes cancer cell survival, Cancer Res69(8) (2009), 3425–3432.
20.
BruixJ. and ShermanM., Practice guidelines committee, american association for the study of liver diseases, management of hepatocellular carcinoma, Hepatology42 (2005), 1208–1236.
21.
ChunY.H.KimS.U.ParkJ.Y.KimD.Y.HanK.H.ChonC.Y.KimB.K.ChoiG.H.KimK.S.ChoiJ.S. and AhnS.H., Prognostic value of the 7th edition of the AJCC staging system as a clinical staging system in patients with hepatocellular carcinoma, Eur J Cancer47(17) (2011), 2568–2575.
22.
FornerA.ReigM.E.de LopeC.R. and BruixJ., Current strategy for staging and treatment: the BCLC update and future prospects, Semin Liver Dis30(1) (2010), 61–74.
23.
KimD.Y.KimS.U.AhnS.H.ParkJ.Y.LeeJ.M.ParkY.N.YoonK.T.PaikY.H.LeeK.S.ChonC.Y. and HanK.H., Usefulness of FibroScan for detection of early compensated liver cirrhosis in chronic hepatitis B, Dig Dis Sci54(8) (2009), 1758–1763.
24.
BoschF.X.RibesJ.DíazM. and ClériesR., Primary liver cancer: Worldwide incidence and trends, Gastroenterology127(5 Suppl 1) (2004), S5–S16.
25.
WongR. and FrenetteC., Updates in the management of hepatocellular carcinoma, Gastroenterol Hepatol (N Y)7(1) (2011), 16–24.
26.
ZhouW.H.TangF.XuJ.WuX.FengZ.Y.LiH.G.LinD.L.ShaoC.K. and LiuQ., Aberrant upregulation of 14-3-3 expression serves as an inferior prognostic biomarker for gastric cancer, BMC Cancer11 (2011), 397.
27.
LizcanoJ.M.MorriceN. and CohenP., Regulation of BAD by cAMP-dependent protein kinase is mediated via phosphorylation of a novel site, Ser155, Biochem J349(Pt2) (2000), 547–557.
28.
Shiba-IshiiA.KanoJ.MorishitaY.SatoY.MinamiY. and NoguchiM., High expression of stratifin is a universal abnormality during the course of malignant progression of early-stage lung adenocarcinoma, Int J Cancer129(10) (2011), 2445–2453.