
Abstract
OBJECTIVE:
The aim of this study is to compare surgery with adjuvant chemoradiotherapy versus non-surgical treatments for patients with early-stage small cell lung cancer (SCLC) based on the short-term and long-term efficacy.
METHODS:
SCLC patients who underwent a pulmonary lobectomy with post-surgical radiotherapy or chemotherapy were assigned to the surgical group. SCLC patients who received radiotherapy or chemotherapy alone were classified into the non-surgical group. The clinical efficacy was evaluated as complete remission (CR), partial remission (PR), stable disease (SD), or progressive disease (PD). The total effectiveness rate was calculated as CR
RESULTS:
Compared with the non-surgical group, the CR rate and the total effectiveness rate were higher in the surgical group, and the total effectiveness rate for male patients and patients without a smoking history were also higher in the surgical group. Distant metastasis and local recurrence concurrent with distant metastasis in the surgical group were both lower in the surgical group than in the non-surgical group. Compared with the non-surgical group, the local recurrence in male patients was lower in the surgical group, and patients in the surgical group had lower distant metastasis at TNM stage IIb. The 1-, 3-, and 5-year survival rates were higher in the surgical group than in the non-surgical group.
CONCLUSIONS:
These findings indicate that for patients with early-stage SCLC, better scores in effectiveness rate, disease progression, and 1-, 3-, and 5-year survival rates were observed in patients who underwent surgery followed by adjuvant chemoradiotherapy when compared with patients without surgical treatment.
Keywords
Introduction
Small cell lung cancer (SCLC) originates from the bronchus mucous membrane or argyrophil cells in the glandular epithelium, and often occurs in the center of the lung [1, 2]. SCLC accounts for 13
SCLC consists of two clinical subgroups. The first is a limited disease, in which tumors are confined within the ipsilateral hemithorax and cover the same radiation field as primary foci (LD-SCLC) [9, 10]. The second is an extensive disease, in which tumors have spread beyond the supraclavicular areas (ED-SCLC) [6]. The main treatment option for LD-SCLC is a combination therapy consisting of surgery, radiotherapy, and chemotherapy. This therapy combines chemotherapy with two drugs concurrent with thoracic radiation. The main treatment option for patients with ED-SCLC is chemotherapy with adjuvant radiotherapy [10]. The thoracic radiation regimen shows that the prognosis of patients with LD-SCLC is improved by concurrent hyperfractionated radiotherapy combined with chemotherapy [11]. With the development of clinical research, combined chemotherapy has become the main therapeutic approach, and the standard treatment is to combine it with uranium and etoposide [12]. The traditional belief is that SCLC is highly responsive to radiotherapy and chemotherapy, thus the emphasis of SCLC therapy should be placed on chemotherapy or radiotherapy instead of surgery [10, 13]. However, reinforcement surgery does not improve the survival rate [14]. Therefore, SCLC patients who underwent surgical treatment before receiving radiotherapy or chemotherapy were enrolled in the present study. Our efforts can help provide references for the choice of the standard therapy and future clinical guidelines.
Materials and nethods
Study subjects
Between January 2005 and January 2010, a total of 208 patients diagnosed with early-stage SCLC via bronchoscope and biopsy were recruited from Central Hospital of Linyi. The inclusion criteria were: 1. pathologically identified SCLC patients with complete clinical information; 2. patients with no pulmonary disease history such as pulmonary tuberculosis and asthma, radiochemotherapy or pulmonary surgery. The exclusion criteria were: 1. patients without pathological identification; 2. patients with advanced SCLC; 3. patients with radiochemotherapy contraindication and an over/under sensitivity reaction to radiochemotherapy; 4. patients declining experiment requirements and demanding a withdrawal. The operative indications were: 1. lesion restricted to unilateral lobectomy; 2. general conditions tolerable to surgery; 3. no systematic dysfunction; 4. positron emission tomography/computed tomography (PET/CT) changes were consistent. One hundred and two patients who underwent a pulmonary lobectomy and post-surgical chemotherapy and radiotherapy were enrolled in the surgical group, including 76 males and 26 females aged from 36 to 79 years old, with a median age of 54.3
Treatment regimens
The 102 patients in the surgical group all underwent a pulmonary lobectomy prior to routine adjuvant chemotherapy (Etoposide & Cisplatin regimen, EP regimen) and thoracic radiotherapy (prophylactic irradiation using 6MV-X ray was delivered in the drainage area of the mediastinum in patients without residual tumors after operation and chemotherapy; dose 30
Efficacy evaluation and follow-up
The clinical efficacy was evaluated according to Eff-
Clinical efficacy in SCLC patients with different pathological characteristics
Clinical efficacy in SCLC patients with different pathological characteristics
ective Evaluation Criteria in solid tumors version 1.1 [15]: a. complete remission (CR); b. partial remission (PR); c. stable disease (SD); d. progressive disease (PD). Two months after treatment, pulmonary computed tomography (CT) was performed and compared with the CT before treatment. The total effectiveness rate was calculated as CR
The SPSS 19.0 software (SPSS Inc., Chicago, Illinois, USA) was used for the statistical analysis. The ranked data were compared using the Wilcoxon test. The comparison between enumeration data was analyzed using the
Results
Efficacy of two treatment regimens for SCLC patients with various clinicopathological characteristics
The comparison of efficacy between the non-surgical group and the surgical group is shown in Table 1. The CR rate and the total effectiveness rate were higher in the surgical group than in the non-surgical group (both
Comparisons of disease progression between the surgical and non-surgical groups
Comparisons of disease progression between the surgical and non-surgical groups
Comparisons of the 1-, 3- and 5-year survival rates between the surgical and non-surgical groups
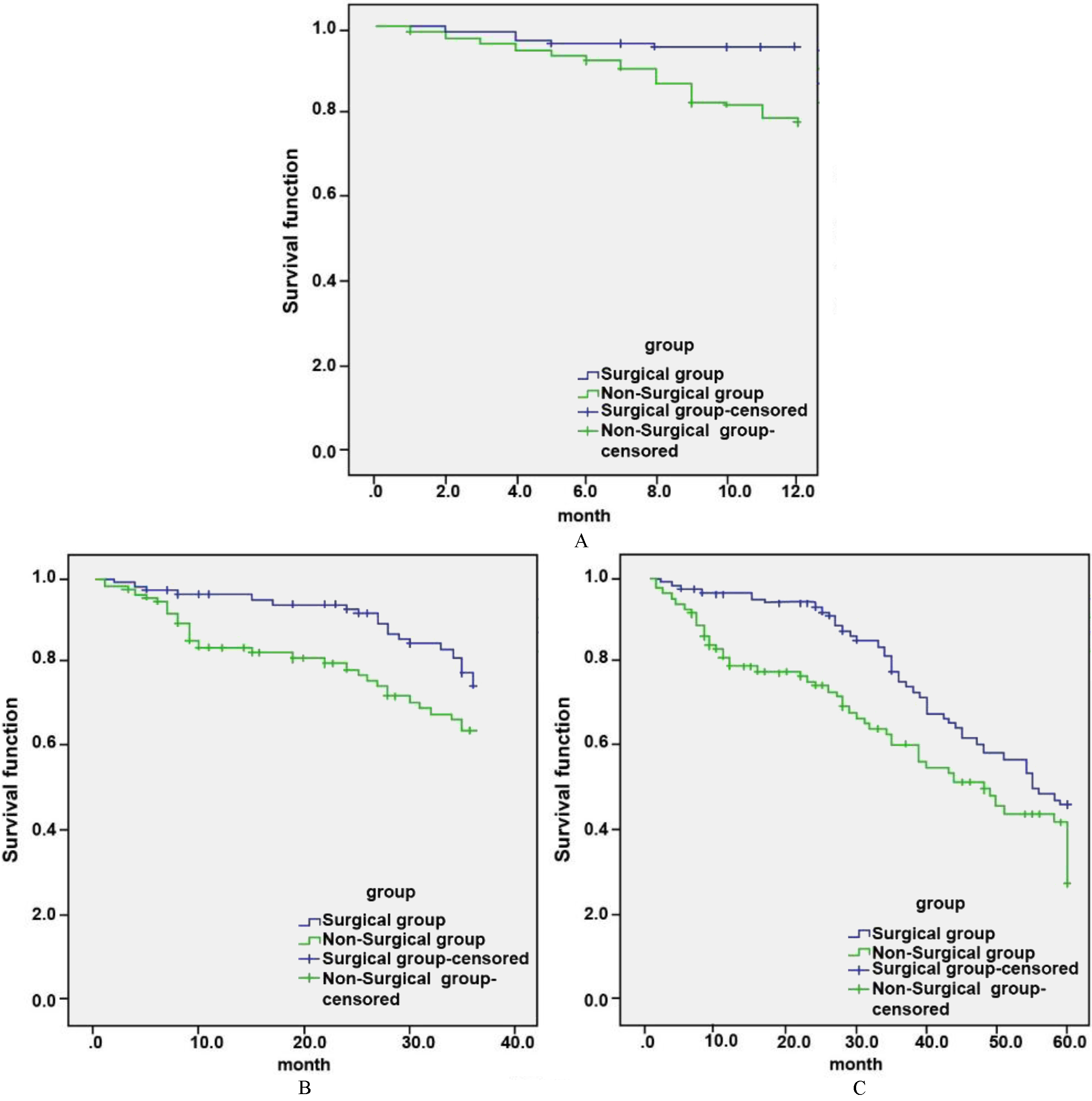
Survival curves of SCLC patients in the surgical group and the non-surgical group. A. 1-year survival; B. 3-year survival; C. 5-year survival.
The comparison of disease progression in the two groups is shown in Table 2. Distant metastasis and local recurrence concurrent with distant metastasis in the surgical group (12.75%, 4.90%) were both lower when compared with the non-surgical group (20.75%, 11.32%) (both
The 1-, 3-, and 5-year survival rate of SCLC patients in the non-surgical and surgical groups
The 1-, 3-, and 5-year survival rates are compared in Table 3 and Fig. 1. The 1-, 3- and 5-year survival rates of the surgical group (96.08%, 78.43% and 50.90%) were higher than those of the non-surgical group (78.30%, 69.81% and 44.34%) (all
Discussion
The combined modality treatments of SCLC mainly include systematical chemotherapy, thoracic radiation therapy, and prophylactic cranial irradiation [16]. Early radiotherapy reduces the repopulation of tumor stem cells and eliminates resistant tumor cells before distant metastasis, thus improving the local control rate and decreasing the distant metastasis rate [17]. Recently, the recombinant human granulocyte colony stimulating factor and antibiotic have been reported may suppress bone marrow compromise or comorbidity caused by chemotherapy or radiotherapy, thus preventing severe infections [18]. Even so, chemotherapy and radiotherapy-related death remains an important threat to the short-term survival rate [19]. Therefore, the present study was conducted, focusing on the several items related to the survival rates in the treatment SCLC, including gender, age, smoking history, TNM stage, and tumor location, to compare the treatment efficacy and prognosis between surgery plus post-operational radiotherapy/chemotherapy and radiotherapy or chemotherapy alone.
We found that the total effectiveness rate in the surgical group was higher than in the non-surgical group. The 1-, 3-, and 5-year survival rates were also higher in the surgical group than in the non-surgical group, suggesting that the surgery option contributes to more effective tumor removal. Despite the advantages of surgery, the reduced lung tissues can negatively affect the lung function [20, 21]. However, the long-term survivors had a better quality of life despite a declined physiological function [22]. Wong et al. demonstrated that the use of postoperative radiation therapy reduced the overall survival rate of early-stage SCLC patients at pathologic Node 0 (N0) stage, but significantly enhanced the overall survival of patients at N2 stage [23]. A recent study has shown that the metastasis of SCLC was well controlled by surgery, as indicated by the prognosis results [24]. The research of Fox et al. produced the 10-year results of a controlled trial for the comparison of surgery and radical radiotherapy in the treatment of SCLC, which reinforced that radical radiotherapy may has a better proven efficacy in the survival rate than surgery [25]. Lad et al. also argues that pulmonary resection fails to improve the survival rate for SCLC patients who respond to chemotherapy or influence the pattern of relapse [26]. In our study, there was a lower metastasis rate in the surgical group when compared with the non-surgical group, suggesting that there may be a higher efficacy of surgery combined with radiotherapy or chemotherapy in controlling distant metastasis and in reducing the toxicity and side effects. Consistent with our results, the retrospective analysis by Dai et al. showed that radiotherapy after surgery markedly improved the survival rates [27].
The present study also found that the efficacy of SCLC was also associated with sex, age, smoking history, TNM stage, and tumor location. Puma et al. found that surgery delivers positive outcomes for SCLC patients in stage T1-T2, and patients who received surgery in combination with chemotherapy displayed a mean survival time of 23 months with a fairly good prognosis [28]. Bremnes et al. reported that age affects the prognosis of LD-SCLC and that the efficacy is better in patients under 60 years old, which maybe because patients at a young age have better cardiopulmonary function, better tolerance for chemotherapy or radiotherapy, and fewer complications [29]. Tamura et al. found that the effects of lung cancer therapy on females were better than those in male patients. This can be associated with the high mutation rate of epidermal growth factor receptor (EGFR) [30]. The expression of EGFR in lung cancer is distributed differently in male and female patients, and is more common in female patients [31]. This suggests that the efficacy and prognosis of lung cancer therapy will be different depending on the gender of patients. Smoking is closely associated with lung cancer, and the difference in the incidence rate is a reflection of the number of smokers and the extent of smoking [32]. Patients with lung cancer who have smoked for a long time are not able to tolerate surgery because of their poorer lung function [33]. These data suggest that some external factors, including sex, age, smoking history, TNM stage, and tumor location, can also influence the efficacy of approaches with surgery or without surgery.
However, some limitations of the present study are worth mentioning. Whether or not the age of SCLC patients determines their outcome after receiving surgical and non-surgical treatment remains controversial. Also, if poor prognoses are correlated with the advanced age requires further investigation. It is generally thought that the elder population had a low tolerance for surgery, and when the surgery duration is prolonged, the risks are increased. Based on the indexes of cardiopulmonary function, the surgical option and the postoperative recovery were limited. The results would be more compelling if the associations of age with efficacy of treatment, disease progression, and survival time were considered in the present study.
Conclusion
In conclusion, SCLC is associated with sex, age, smoking history, TNM stage, and tumor location. In patients with early-stage SCLC, surgery supplemented with post-operational radiotherapy or chemotherapy reduced local recurrence and distant metastasis, and prolonged survival time, suggesting that the surgical option is more effective. Our study provides references for the regimens of SCLC therapy. However, the mechanisms of these regimens on SCLC require further investigation.
Footnotes
Acknowledgments
We would like to acknowledge the helpful comments on this paper received from our reviewers.
Conflict of interest
None.