
Abstract
BACKGROUND:
Dynamic knee valgus (DKV) during dynamic activity is associated with patellofemoral pain, one of the most common sports disorders, especially in females. No studies have examined the factors that can lead to DKV in females as compared to males while addressing the influence of factors on each other.
OBJECTIVE:
To identify factors of pelvis and lower joints kinematics affecting DKV during single-leg squat (SLS) in females compared to males with multiple regression analysis.
METHODS:
Forty-four healthy young people (24 females, 20 males) performed SLS, and pelvis, hip, knee, and ankle 3D kinematics were recorded. The 2D knee frontal plane projection angle (FPPA) was adopted as the DKV measurement. Multiple regression analysis was performed to determine the relationship between FPPA and the kinematics of each joint and segment.
RESULTS:
Hip adduction and pelvic contralateral rotation were explanatory factors for FPPA in females. Hip adduction, hip internal rotation, and knee external rotation were explanatory factors in males.
CONCLUSIONS:
The lower limb or pelvic motion factors affecting DKV during SLS differ between the sexes, with pelvic contralateral rotation being extracted only in women, possibly due to differences in pelvic width.
Introduction
Dynamic knee valgus (DKV) described as a defect in the movement pattern where the knee collapses medially during weight-bearing may contribute to the progression of patellofemoral pain (PFP), which is one of the most common musculoskeletal conditions encountered in sports medicine [1, 2, 3]. There are a variety of clinical movement tests to identify DKV and single-leg squat (SLS) is a simple and easy test to assess the risk of lower extremity injuries for athletes. Movement in the lower extremities during SLS relates to those during more complex tasks such as landing and running [4, 5, 6]. However, we need to be careful dealing with DKV during SLS because DKV is not merely knee movement in the frontal plane motion [7], but is the result of complex movement with multiple joints. Although previous reports have suggested that the kinematic factors associated with DKV include hip, knee, ankle, and pelvic motion [8, 9, 10], these studies are based on two-group comparisons or correlations, only the one-to-one relationship between DKV and kinematic factors has been examined. Since correlation coefficients include not only direct effects but also indirect effects that affect the dependent variable through other factors, it is difficult to identify factors that have direct influences because they cannot fully explain the relationship between factors. It is necessary to examine which factors have a stronger direct influence by conducting multiple regression analysis and comparing the standard partial regression coefficients.
Furthermore, some previous studies have treated males and females as subjects without distinction, so have not taken into account sex differences in examining the factors of DKV [9, 11]. However, females were 2.23 times more likely to develop PFPS compared with males [12]. In addition, there are sex differences in the biomechanics in SLS that have been associated with DKV, such as ankle motion, hip motion on the frontal and horizontal planes [13, 14, 15]. Therefore, it is necessary to examine the kinematic factors that affect DKV separately in males and females.
Thus, in this study, we aimed to identify kinematic factors strongly associated with DKV in each sex, and clarify what kind of motion is affecting DKV and how deeply, while addressing the influence of factors on each other. Since multiple regression analysis is used in this study, factors with indirect influences that interact with each factor would be excluded and factors with direct influences would be found. Therefore, we hypothesized that pelvic factors would be excluded and hip factors would be listed. We also hypothesized that the ankle joint would be a factor in males, but not in females, because females have been reported to have greater ankle dorsiflexion than males.
Methods
Subjects
Forty-four healthy young people (24 females, 20 males) volunteered for this study. Participants were recruited by convenient sampling. Participants with no history of knee trauma or knee pathology and with full active knee flexion were included in this study. Exclusion criteria included a history of knee ligament injury, patella dislocation, knee pain within 6 months of testing, or any lower extremity symptoms that may affect testing [14]. Subjects provided written informed consent to participate in this study after receiving a detailed explanation regarding the purpose, potential benefits, and risks involved with participation. This trial was approved by the ethics review board of our institution, and performed in accordance with the Declaration of Helsinki, 1964, and comparable ethical standards. Informed consent was obtained from each participant.
Four phases of single-leg squat.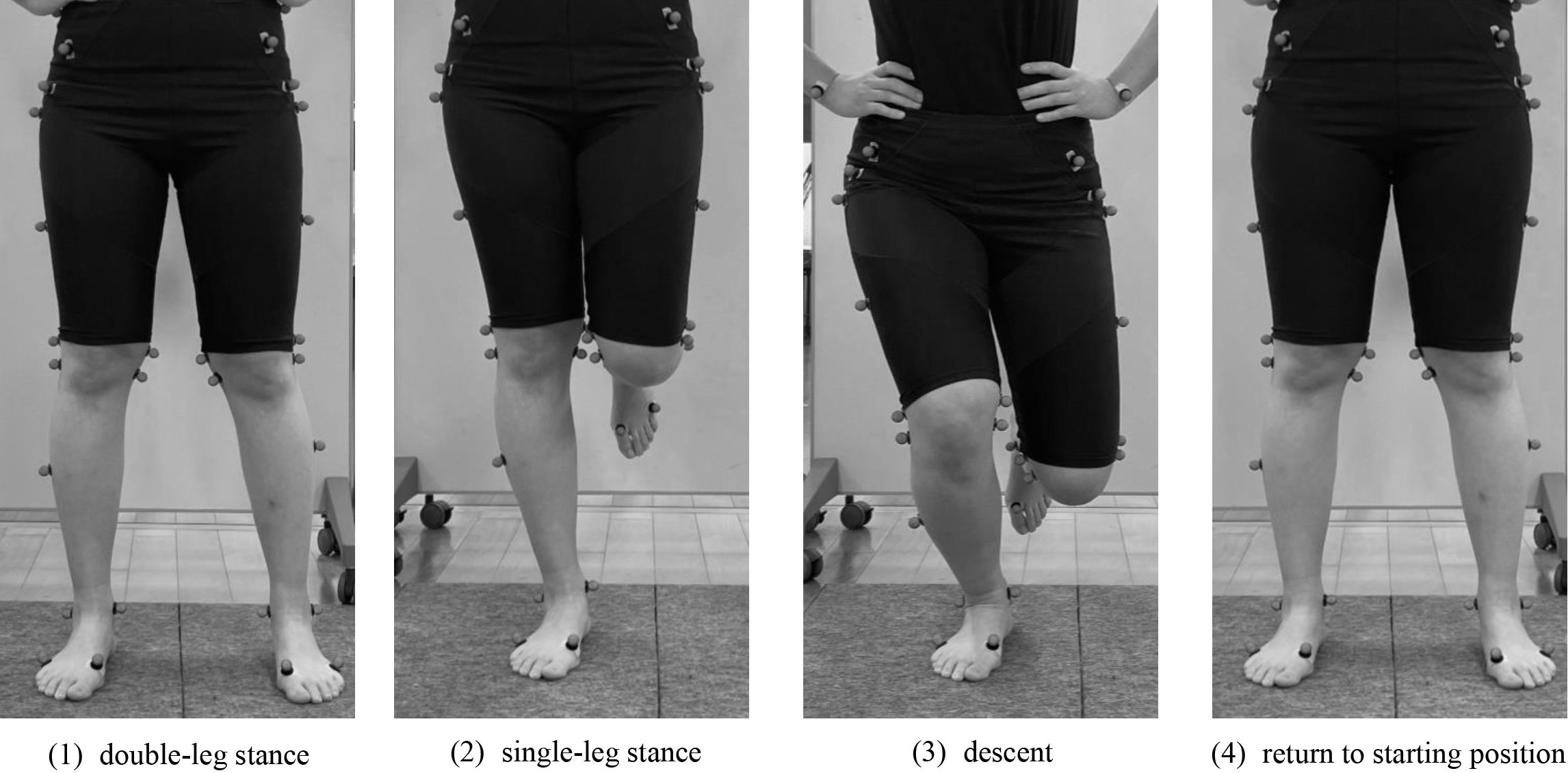
The starting position was a natural posture of standing barefoot on two force plates (Tec Gihan TF-400-A, Uji, Japan) with long toes separated at anterosuperior iliac spine interval distance (Fig. 1). They were then asked to perform a total of five SLSs with their dominant leg (preferred kicking leg) based on the procedure described by Kim et al. [16]. It has been described that DKV, a risk factor for PFP, is greater in the kicking leg (dominant leg) than in the supporting leg (non-dominant leg) [17], therefore, this study was conducted in the kicking leg. Movement speed was standardized using a metronome beat of 80 beats per minute. At the first beat, the subjects lifted their toe off the force plate to make the transition from double to single-leg stance. Then, at the next beat, they descended their body to the lowest position, they squatted to approximately 70 degrees of knee flexion. After that, they returned to the starting position. Joint motion during SLS has been found to vary between the flexed position and neutral position of the non-stance hip joint [18]. In this study, the subjects keep the non-stance thigh vertical to the ground and the knee flexed to 90 degrees. Subjects practiced sufficiently to achieve a knee flexion angle of 70 degrees before the measurement. The power analysis revealed that at least 22 participants would be necessary to achieve 80% power for an effect size
Measurements
The kinematic data during the SLS were collected using Vicon MX (Vicon Motion Systems, Oxford, UK), which is a three-dimensional motion analysis system involving six infrared cameras working at a sampling rate of 100 frames/s. Infrared-reflecting markers with a diameter of 14 mm were attached to 40 landmarks. The positions of the markers were determined based on previous studies [19]. These markers were used to construct anatomical coordinate systems for the head, trunk, pelvis, thigh, shank, and foot segments. The kinetic data were collected by two force plates at a sampling frequency of 1000 Hz. Kinematic and kinetic data were low pass filtered with a fourth-order Butterworth filter and cutoff frequencies of 6 and 15 Hz, respectively [20].
Data analysis
The results of univariate linear regression analysis for each independent variable in females
The results of univariate linear regression analysis for each independent variable in females
Positive value: ankle dorsiflexion, knee external rotation, hip abduction, hip external rotation, pelvic drop toward the weight-bearing limb, pelvic rotation toward the weight-bearing limb;
The result of the regression model in females
Positive value: hip abduction, pelvic rotation toward the weight-bearing limb, hip external rotation, ankle dorsiflexion; FPPA: knee frontal plane projection angle; VIF: variance inflation factor.
Data analyses were performed using Vicon Nexus software (Vicon Motion Systems, Oxford, UK). The centers of joint coordinates were calculated as previously described [21, 22]. Using the collected marker coordinates, a rigid link model consisting of nine segments (head, chest, pelvis, both thighs, both shanks, and both feet) was constructed. Anthropometric parameters for mass and center of mass (COM) for each segment were obtained from a previous report [23]. Segment angles refer to the orientation of a segment relative to the global space. Joint angles were calculated as the distal segment relative to the proximal segment (i.e., ankle angle is the foot angle relative to the shank segment, knee angle is the shank angle relative to the thigh segment, and hip angle is the thigh angle relative to pelvic segment. A fixed laboratory coordinate system was defined at
Statistical analyses were performed using JMP Pro 15.0.0 (JMP Pro, SAS Institute Japan Ltd., Tokyo, Japan). We used multiple linear regression to evaluate whether the variables of interest predicted FPPA for males and females, respectively. The 6 angles (ankle sagittal plane angle, knee transverse plane angle, hip frontal plane angle, hip transverse plane angle, pelvic frontal plane angle, and pelvic transverse plane angle) have been reported to influence DKV based on previous studies [8, 9, 10, 24] were adopted as independent variables. We performed univariate analysis for each independent variable with FPPA as the dependent variable. Variables that showed a significant association of
The results of univariate linear regression analysis for each independent variable in males
The results of univariate linear regression analysis for each independent variable in males
Positive value: ankle dorsiflexion, knee external rotation, hip abduction, hip external rotation, pelvic drop toward the weight-bearing limb, pelvic rotation toward the weight-bearing limb;
The result of the regression model in males
Positive value: hip abduction, pelvic rotation toward the weight-bearing limb, hip external rotation, ankle dorsiflexion; FPPA: knee frontal plane projection angle; VIF: variance inflation factor.
Participants in our study had mean and standard deviations for age, height, and weight of 21.7
Discussion
A better understanding of the kinematic factors of DKV during SLS may promote the early identification of females with a high risk of PFP. Therefore, the purpose of this study was to identify kinematic factors strongly associated with DKV in each sex, and clarify what kind of motion is affecting DKV and how deeply, while addressing the influence of factors on each other. In females, among the six variables adopted in this study, only two were found to be explanatory factors of FPPA. The findings of our study demonstrated that hip adduction and pelvic contralateral rotation predicted DKV during SLS; individuals with greater hip adduction and greater pelvic contralateral rotation showed higher DKV during the SLS task. Among these, pelvic contralateral rotation was a female-specific factor. In males, among the six variables adopted in this study, three were found to be explanatory factors of FPPA. In our study, hip adduction, knee external rotation, and hip internal rotation.
The first explanatory factor for DKV was hip adduction which was a common factor for both females and males. Several studies have identified that hip adduction is an associated factor of DKV [8, 25, 28]. The hip adduction angle has a great influence on FPPA because a large motion occurred in the hip joint on the frontal plane. It also can be explained by the large
The other independent variable in females is pelvic contralateral rotation. This result supports previous studies that have shown the correlation between DKV and pelvic contralateral rotation [8]. In the single leg task, the COM needs to remain in the base of support, which is narrowed in the mediolateral direction. One of the strategies may be pelvic contralateral rotation pivoting on the hip joint of the supporting leg to shift the COM toward the supporting leg and remain in the base of support. It was reported that females had a wider pelvic width [30], therefore, they might require more pelvic rotation to shift the COM compared to males. This motion means relatively more external rotation at the hip joint, which is in agreement with reports that females exhibit greater hip external rotation during SLS [15]. In females, hip adduction and pelvic contralateral rotation are listed as explanatory factors, suggesting that pelvic rotation as an effect of motion in the transverse plane affects DKV. On the other hand, in males, hip internal rotation and knee external rotation are listed as explanatory factors in addition to hip adduction, suggesting that thigh internal rotation may influence DKV in males. These gender differences in motor control may be one reason why PFP is more common in females.
Previous studies have shown that the ankle dorsiflexion range of motion in the non-weight-bearing position is related to DKV during SLS [11]. Therefore, in this study, we expected that ankle dorsiflexion motion could be an explanatory factor for DKV. Contrary to expectations, ankle sagittal plane angle did not predict the degree of FPPA in females. Ankle dorsiflexion motion was excluded from the independent variables, but this was probably due to the statistical method of multiple regression analysis. In our study, multiple regression analysis showed that hip adduction was the most significant predictor. Rabin et al. and Bell et al. reported that ankle dorsiflexion was related to hip adduction during the dynamic task [31, 32]. Therefore, the previously reported effects of ankle dorsiflexion may be indirect effects through hip adduction, and not direct.
The results of the multiple regression analysis of this study showed that hip adduction and pelvic contralateral rotation were predictors of DKV in females. In previous studies, it has been reported that trunk and hip muscle strength are associated with FPPA during SLS [33, 34]. The ability to control the proximal segments and joints such as the trunk, pelvis, and hip during weight-bearing activity may contribute to preventing DKV.
This study is a cross-sectional study of healthy young subjects, and thus the risk factor cannot be accurately identified. In the future, it is necessary to conduct a prospective cohort study based on the factors identified in this study and others to examine risk factors more precisely.
Conclusion
The findings of the present study showed that hip adduction and pelvic contralateral rotation predicted 77% of the variance for DKV in females. Among these factors, pelvic rotation was a female-specific factor. Ankle dorsiflexion has no direct influence on DKV.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Committee for Epidemiology of Hiroshima University (E-467-4).
Funding
Not applicable.
Informed consent
Written informed consent was obtained from all subjects.
Author contributions
Study conception and design: Ryosuke Takeuchi, Yoshitaka Iwamoto, Makoto Takahashi.
Data collection: Ryosuke Takeuchi, Yasutaka Takeuchi, Fumiya Miyoshi, Wataru Kawakami.
Data analysis and interpretation: Ryosuke Takeuchi, Yoshitaka Iwamoto.
Preparation of the manuscript: Ryosuke Takeuchi, Yoshitaka Iwamoto, Yosuke Ishii, Makoto Takahashi.
Revision for important intellectual content: Ryosuke Takeuchi, Yoshitaka Iwamoto.
Footnotes
Acknowledgments
Not applicable.
Conflict of interest
The authors have not conflict of interests to declare.