
Abstract
Background
Cardiometabolic multimorbidity (CM), two or more of stroke, diabetes, and heart disease is increasing in prevalence and associated with a multiplicative mortality risk. Sex differences exist in disability outcomes for those with stroke, diabetes, and heart disease, and thus are likely for those with CM.
Objectives
To assess 1) sex differences in the prevalence of CM, 2) sex differences in disability variables amongst those with CM, and 3) the predicted probabilities of disability among people with and without CM by sex.
Methods
A secondary analysis using data from the Canadian Longitudinal Study on Aging (CLSA). The CLSA included a stratified, random sample of approximately 51,000 participants aged 45 to 85 at recruitment. Independent variables include depressive symptoms, pain, high blood pressure, eyesight, limitations with activities of daily living (ADL), and social participation.
Results
A weighted population of 13,204,82 participants were included, 659,621 had CM. Males had a higher prevalence of CM than females, accounting for 62% of those with CM. Females with CM had a higher probability than males of reporting high depressive symptoms (females: 29% [95%CI:27%-31%], males: 21% [95%CI:19%-23%]), pain (females: 49% [95%CI:47%-52%], males: 41% [95%CI:39%-43%]), and limitations with ADL (females: 27% [95%CI:25%-29%], males: 11% [95%CI:10%-13%]) Males with CM had a higher probability than females of reporting infrequent social participation (females: 18% [95%CI:16%-20%], males: 23% [95%CI:21%-25%]).
Conclusion
This study provides evidence on sex differences in the likelihood of reporting disability variables in individuals with CM. These insights into sex differences can inform targeted interventions and improve patient outcomes.
Introduction
Stroke, heart disease, and diabetes represent three of the most common chronic diseases (CD) and are among the top 10 leading causes of mortality in Canada, contributing to over 70,000 deaths annually. 1 These three conditions share common etiologies, such as health behaviours, including low physical activity, poor diet, and smoking. 2 These shared etiologies promote the simultaneous development of each disease, ultimately resulting in cardiometabolic multimorbidity (CM). CM is defined as the diagnosis of at least two of stroke, heart disease, and diabetes 3 . Research indicates that approximately 500,000 Canadians over 50 years of age had CM in 2016 2 . CM is a key health concern associated with increased mortality risk and subsequent lower life expectancy. 3 Beyond mortality, CM has important implications for functional decline and disability, including an increased risk of activity of daily living limitations, 4 depression, 5 dementia 6 and cognitive decline. 7 CM has also been reported in the past to be associated with more rapid progressions of disability. 8 Disability related to CM places a considerable burden not only on affected individuals but also on healthcare systems and society at large.
Sex (biological attributes) and gender (socially constructed roles, behaviours, and identities) influences many factors of health, including the risk of developing CD, how people respond to treatments, and how often people seek health care. 9 Studying how different biological, behavioral, and systemic health factors between sexes contribute to health outcomes is key to improving health. 10 Biological factors including sex chromosomes, gonadal hormones and their resulting effects, lead to differences in morphology, physiology, and behavior between males and females. 11 Systemic health factors which differ between males and females include social inequities and sexism, access to quality health care, and the complex interactions between a person and their community or neighbourhood they reside in. 11 Overall, identifying and understanding sex differences is required for improvements in diagnosis, treatment, and outcomes. 12
There is evidence of sex differences in both the development of CM and related outcomes (e.g. disability, recovery). For example, although more males live with diabetes, the risk of stroke associated with diabetes is significantly higher in females. 13 In addition, having type 2 diabetes is a greater risk factor for females in the development of heart disease than it is in men. 14 Finally, females generally have a higher prevalence of multimorbidity than men, and previous literature has even noted persistent differences in cardiovascular multimorbidity progression between sexes. 15
Currently, there is a paucity of knowledge on disability outcomes amongst those with CM. Moreover, the few studies that have investigated disability have not analyzed outcomes separately by sex, leaving an important gap in understanding. This leaves health professionals and policymakers with little guidance on how to treat CM patients holistically. In this study, our objectives were to 1) assess sex differences in the prevalence of CM, 2) assesses sex differences in disability variables between males and females who have CM, and 3) assess the predicted probabilities of disability among people with and without CM by sex.
Methods
This secondary analysis utilized an observational, cross-sectional research design with data from the Canadian Longitudinal Study on Aging (CLSA) ‘tracking’ and ‘comprehensive’ cohorts. Reporting follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 16 Ethics approval was obtained by the University of British Columbia Behavioural Research Ethics Board (H19-00485).
Data source
The CLSA is a national, longitudinal study conducted to better understand the biological, medical, social, psychological, lifestyle, and economic processes and dimensions of aging that impact the maintenance of health and the development of disease and disability. 17 Canadians aged 45 to 85 years were recruited at baseline between 2010 to 2015. Participants complete study-specific questionnaires and undergo repeated waves of data collection every three years for at least 20 years or until death. In both cohorts, participants were selected through structured probability sampling methods. This included using the Canadian Community Health Survey on Healthy Aging, provincial health registries, and random-digit dialing. In the tracking cohort, baseline data from volunteer participants was collected using self-report questionnaires administered through 60-minute computer-assisted telephone interviews. To mitigate related barriers of utilizing computer-assisted telephone interviews, the CLSA had trained interviewers facilitate these interviews to support individuals who may have had difficulty using digital platforms. 18 At the time of data collection, participants experiencing hearing impairments, speech/language difficulties, or vision loss were offered accommodations as required. Procedures were in place to identify and implement appropriate accommodations, such as involving a helper or modifying test administration. In addition, the telephone interview could be broken up into multiple interviews as required. Data was collected in the tracking (n=21,241) cohort from all ten provinces with no geographic restrictions. In the comprehensive cohort (n=30,097), data was collected through in-home interviews and at data collection site visits. There are 11 data collection sites across Canada, located in Victoria, Vancouver, Surrey, Calgary, Winnipeg, Hamilton, Ottawa, Montreal, Sherbrooke, Halifax, and St. Johns. Ethics approval has been received from all associated sites.
Participants
All individuals in the CLSA were included in our analyses if data was available for our dependent and independent variables. Excluded from the CLSA and thus our research were residents in the three territories and some remote regions, persons living on federal First Nations reserves, full-time members of the Canadian Armed Forces, individuals living in institutions at recruitment, those unable to respond in English or French, or those who had cognitive impairment at recruitment.
Variables and measures
Variables included in the study were organized by The International Classification of Functioning (ICF) and can be seen in Figure 1.
19
The ICF is an internationally recognized multidimensional biopsychosocial framework of health, functioning and disability. The ICF conceptualizes functioning and disability at each of the body level (body function and structure), person level (activity), and social level (participation) and as a dynamic and complex interaction between health conditions and contextual factors.
20
Variables organized by the International Classification of Functioning, Disability and Health.
Body function and structure:
Activity:
Participation:
Biological sex: Sex was determined from the question “are you male or female?”
Statistical analyses
The sample was characterized with continuous variables presented as means and standard deviations and categorical variables as percentages and frequency counts. Sample characteristics were reported amongst those with and without CM. Responses “don’t know” and “refused” were treated as missing. To account for survey design effects and to ensure results were generalizable to the Canadian population, weighted analysis was conducted for all analyses. Per guidelines and weights provided by the CLSA, inflation weights were used in the descriptive analysis and analytic weights in the regression analysis. The use of the sampling weights helps to mitigate potential sources of bias as they account for unequal selection probabilities and differential nonresponse rates across population subgroups. 28 The inflation weights ensure that estimates generalize to the broader Canadian population by aligning the sample with known population distributions from Statistics Canada benchmarks, while the analytic weights further adjust for potential variation in response rates within the provinces and data collection sites. Ultimately, this allows for more valid inferences when examining the associations between variables. All statistical analyses were performed using Stata 29 at a significance level of p < 0.05.
Objective 1: The prevalence of CM was calculated from the total number of respondents reporting CM divided by the total number of respondents in the sample. This calculation was stratified by sex.
Objective 2 & 3: Logistic regression was used to assess sex differences in disability variables among people with CM. All models were adjusted for contextual factor covariates including age, education, marital status, and living location. Potential interaction effects between sex and CM were tested for in each model. If no interaction was present, it was removed from the model. Results are presented as odds ratios with 95% confidence intervals and predicted probabilities.
Results
This secondary data analyses included 51,130 people (Figure 2), representing a weighted population total of 13,204,828. Of this, 659,621 (5%) had CM. Consort diagram with sample size (N) and weighted population (WP).
Sample characteristics.

aN reported as weighted frequency.
Overall weighted prevalence – by diagnostic groups (13,232,651).

Odds Ratios: Odds of females with CM reporting outcome compared to males with CM.
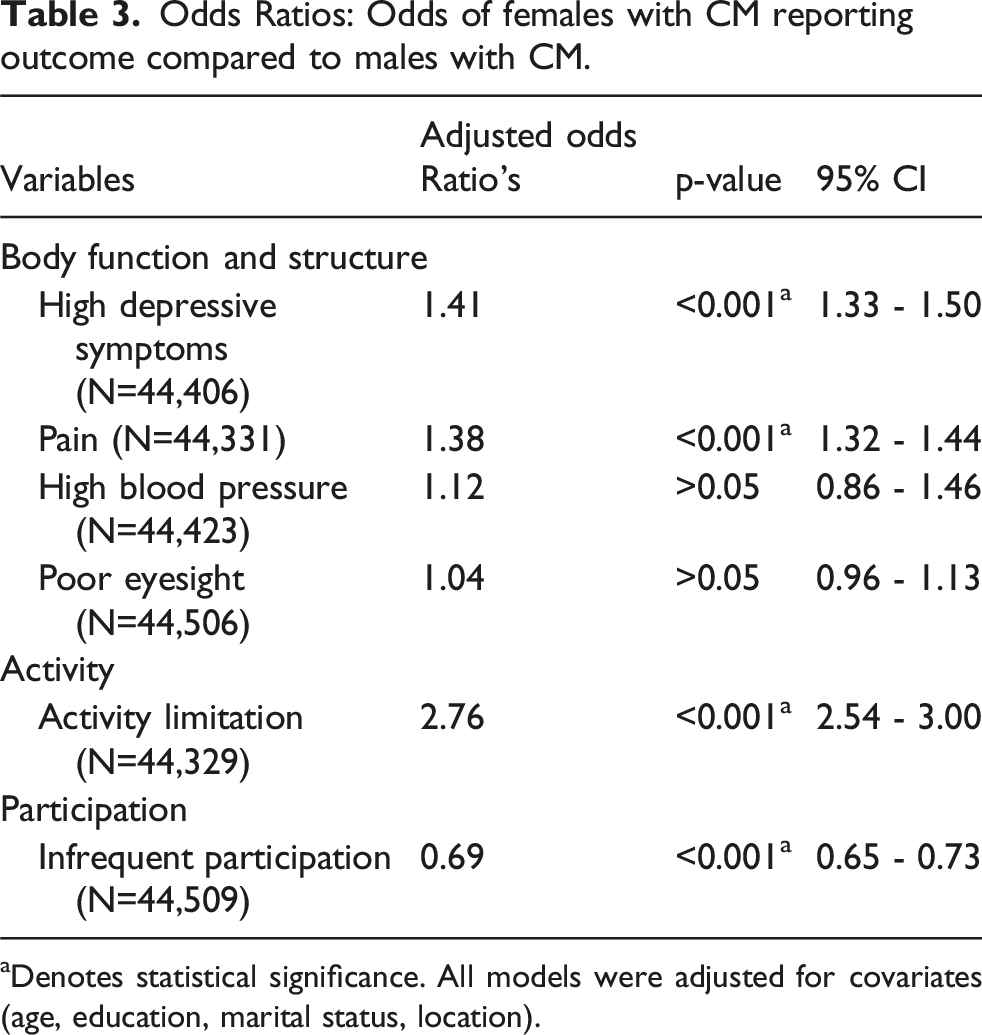
aDenotes statistical significance. All models were adjusted for covariates (age, education, marital status, location).
Predicted probability of reporting disability variables of interest between males and females with and without CM.

All models were adjusted for covariates (age, education, marital status, location).
Discussion
In this study, we assessed sex differences in the prevalence of CM, assessed sex differences in disability variables between males and females who have any combination of stroke, heart disease, and diabetes (CM), and assessed the predicted probabilities of disability among people with and without CM by sex using data from the CLSA.
We observed the proportion of males with CM to be higher than females. These findings both support and conflict with existing literature, as Cheng (2022) reported findings in the United States, where CM age-standardized prevalence was observed to be higher in males (15.6%) than in females (13.4%). 30 However, a study by Zhang (2022) highlighted a notable sex difference in the progression from healthy to first condition, and from first condition to CM, revealing a stronger association in females (Hazard Ratio [HR] = 1.26, 95% CI: 1.15-1.39; HR: 1.42, 95% CI: 1.10 – 1.85, respectively) compared to males. 31 There are various biological factors that may explain why females tend to be protected against heart disease, stroke, and diabetes onset.32–34 For example, female hormones, such as estrogen, have shown protective effects on the cardiovascular system. 32 Estrogen provides a wide range of physiological effects on the female body that can be crucial to the growth and maturation of the endocrine, cardiovascular, skeletal, and metabolic systems. However, it is also important to note the complexity of estrogen’s influence on females, especially when females become older. Females also experience a reduction in estrogen levels once menopause begins, and thus can change the level of protection on the cardiovascular system it may have previously had. 35 Further, females often have better microvascular function than men, contributing to better blood flow and oxygen delivery to tissues. 32 In addition, females mount more robust immune responses, 36 which may help protect against infections and inflammation associated with heart disease.
It is worth noting that we acknowledge sex and gender as distinct concepts, with sex referring to biological and physiological characteristics and gender referring to socially constructed roles, relationships, and power dynamics. 37 The impact of biological sex versus socially constructed gender on health outcomes, including disability, is difficult to disentangle. 37 Gender was not captured by the CLSA in the baseline data, but it was introduced in follow-up datasets. 18 In the first follow-up, the number of participants reporting being transgender, gender queer, or other is less that 0.01%.38,39 As such, we operationalize sex and gender as synonymous, allowing us to speculate how socially driven factors may contribute to the observed differences in disability outcomes between males and females. Speaking to social factors, females often adopt healthier lifestyles, including better dietary choices and lower smoking rates. 40 However, this isn’t always the case as traditional gender norms may constrain female’s abilities to better take control of their health. This includes less decision-making power in family planning or limiting physical activity to avoid appearing less feminine. 41 Strong social networks and emotional support can also positively impact heart health and decrease the risk of stroke. 42 Specifically, females have previously been reported to benefit more from supportive social networks compared to males. However, females also tend to be vulnerable to any lack of supportive or conflict-filled relationships, making the type of social network important in supporting the health of females. 43 Also, females tend to seek medical care more frequently, leading to earlier detection and management of risk factors. 44 However, it is important to note that these conditions, particularly heart disease, have been diagnosed and treated differently between males and females. Specifically, females may have traditionally experienced less intensive diagnostic procedures, and delayed treatment. 45 This is supported by previous reports that show patterns of males having better access to medicine and health care services than females. 46 One previous study even highlights females being independently associated with increased odds of perceived and unmet health needs. 47 Thus, while females may be protected against these conditions, they also may be less likely to be diagnosed and treated. Overall, knowing that males are at a higher risk for CM allows clinicians or policy makers to design targeted interventions effective for this population, including preventative measures, more frequent screening, and education about managing risk factors. Investigations of sex differences and of disability in general amongst those with CM are scarce.
When investigating sex differences in functioning and disability, we found that females have a higher odds of reporting high depressive symptoms, pain, higher blood pressure and activity limitations than males. Our findings are largely consistent with previous literature. One study of approximately 138,000 older adults from Canadian, European and American cohorts found that females reported greater depressive symptoms than males. 48 This is further supported when comparing our findings to a previously published 23-year prospective cohort study, in which the authors reported the risk of multimorbidity with depression to be higher in females than males. 49 Furthermore, data obtained from the Canadian Community Health Survey indicates that females to be more likely to suffer from chronic pain than males, with 18% of Canadian females reporting pain compared to only 14% of males. 50 Interestingly, we observed an interaction effect between sex and CM status among people with high blood pressure. More specifically, our results indicate that females without CM have a lower odds of reporting high blood pressure than males, but once they develop CM there is no longer a significant difference between females and males. The literature shows that for a variety of reasons, males typically do have higher blood pressure than females, yet with advancing age, the prevalence of hypertension amongst females rises to levels higher than age-matched males. 51 Our findings could be explained by CM populations typically being older, and this is most likely true for those with CM in our study as well. In terms of activity limitations, our results align with previous literature of older adult females in Canada have a significantly higher odds of reporting activity limitation: among those in their 60s, 18% of females versus 16% of males, and among those in their 70s, 24% versus 21%. 52 Looking to previous evidence on social participation amongst older Canadians, two studies conflicted our results by showing that males and females have similar participation levels,53,54 yet one of these studies found that females want to participate more than males (26.6 vs. 20.7%). 54 Indicating that the self-reported nature of participation levels reflects what individuals think they want, rather than the actual difference between males and females. In our study, males with CM had a higher odd than females of reporting infrequent community and social participation, but not limitation. It’s possible that females may be emotionally more impacted by the absence of social participation than men, leading to depression.
Our findings largely corroborate previous literature on sex differences in disability amongst the general population. However, this study adds to the body of knowledge specific to CM by providing novel information on the potential disabilities amongst those with CM face, and how they differ by sex. Our results indicate that people with CM have an overall higher odds of reporting some form of disability compared to those without CM. Diseases that comprise CM share common risk factors, such as tobacco smoking, 55 excessive alcohol consumption,55,56 unhealthy diets,55,56 and low physical activity.55–57 When these conditions coexist, they plausibly increase the likelihood of disability. 58 For example, chronic inflammation, stress, impaired organ function, narrowing of arteries, and reduced blood flow resulting in impaired cardiovascular function, muscle weakness, joint problems, and other CM-related issues gradually contribute to functional decline, making activities such as walking, climbing stairs, and self-care challenging. Further, CM is more prevalent in older adults, and as age increases, the cumulative effects of multiple conditions become more pronounced, leading to disability. 58
The observed sex differences in disability among those with and without CM can be explained by a variety of intersecting biological and social considerations. Hormonal influences, including fluctuations in females, play a crucial role in mood and pain perception, 59 potentially accounting for some of the reason females had a higher odds of reporting high depressive symptoms and pain in this study. Having pain and high depressive symptoms may in turn contribute to the higher prevalence of activity limitations seen in females. 52 Moreover, various societal factors (i.e., gender roles, gender norms) can contribute to differences between males and females, especially in the case of social participation. Gender driven social influences can also create biological differences in males and females. 60 For example, psychosocial stress can affect neuroendocrine functions that contribute to cardiometabolic CD onset. 61 While this seems like purely a biological influence, there may be gendered psychosocial stressors like caregiver stress or wage inequalities that are influencing these biological phenomena. 61
Overall, our findings may support the idea of focusing on sex-specific approaches to managing CM. For example, females may benefit from community-based interventions that include exercise and mental health support to improve depressive symptoms and activity limitations. A recent review reports exercise as an effective treatment for depression. 62 Another review highlights how social connection is protective against depression, 63 suggesting that community-based interventions may improve overall well-being in women with CM. At the same time, men may benefit from preventative health management interventions to decrease blood pressure at a young age. Due to a lack of attendance of men in such programs, a scoping review from 2015 identified factors that may increase attendance, including a preference to participate with men similar to themselves in terms of demographics and/or interests, the use of humor in the content, the integration of nutrition and physical activity, and some form of competition. 64 A greater understanding of the sex-related experiences of males and females with CM could lead to upstream prevention strategies to address their specific vulnerabilities to subsequent disability. Future research may continue looking into these differences to develop personalized strategies to the differences between males and females with CM.
Limitations & future directions
This research is not without limitations. First, because of the cross-sectional nature of our research, we were not able to establish cause-and-effect relationships. Secondly, there are limitations from the CLSA sample itself, as the sample consisted of 95% white participants. Excluded from the CLSA and thus our research were residents in the three territories; persons living on federal First Nations reserves; full-time members of the Canadian Armed Forces; individuals living in institutions at recruitment; inability to respond in English or French; or cognitive impairment at recruitment. Thus, the generalizability of the data is limited. Third, there is a risk of self-selection bias, including individuals who may have chosen not to participate if they were uncomfortable using or did not have access to technology (e.g. telephone interviews). Future research may consider how similar results can be generalizable to other groups that were not robustly included in the CLSA data.
Data collection via telephone interviews may impact data quality due to hearing, cognitive, or attentional challenges, possibly increasing measurement error. Despite the accommodations the CLSA provided as outlined in the methods section, it remains possible that there may be greater measurement errors in the telephone interviews. In addition, our reliance on self-reported disease status introduces the potential for recall and reporting bias. This is especially relevant given the age group and the cognitive load required for such interviews and the complexity of differentiating conditions. Future work would benefit from using clinical objective evaluations or validating self-reports with disease-related information (e.g., taking medications).
Changes in clinical guidelines and diagnostic thresholds for cardiometabolic conditions over time may impact how cases of CM are identified in the future. This could influence future prevalence estimates observed in longitudinal studies. Similarly, evolving definitions of disability may shape self-reported measures and functional assessments differently across time points. While our study uses consistent operational definitions of disease and disability, future research should consider how shifting definitions might affect comparability across cohorts and time periods. Furthermore, the current definition of CM does not consider the severity of individual diseases, as the CLSA does not include detailed clinical data on disease stage or severity. While our approach aligns with previous population-based cohort studies that operationalize CM based on the presence of conditions rather than their severity, future research with access to more detailed clinical data could explore how disease severity influences the relationship between functional disability and CM onset.
Conclusion
Our study revealed that males have higher odds of developing CM than females. In addition, females are more likely to report disability related to the body function and structure domain, as well as the activity domain of the ICF. On the other hand, male participants were more likely to report infrequent participation. These findings could inform sex-specific strategies to prevent and manage CM.
Footnotes
Acknowledgement
This research was made possible using the data collected by the Canadian Longitudinal Study on Aging (CLSA). This research has been conducted using the CLSA Baseline Comprehensive Dataset version 4.0, Baseline Tracking Dataset version 3.4, under Application ID 180906. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland.
Ethical considerations
This study received ethical approval from the University of British Columbia Behavioural Research Ethics Board (H19-00485) on April 12, 2019.
Consent to participate
This was a secondary-analysis, all participant information was de-identified and participant consent was not required.
Funding
Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta and British Columbia, and Heart and Stroke Foundation of Canada National New Investigator Award (to BMS).
Declaration of conflicting interests
All authors declare they have no competing interests.
Disclaimer
The opinions expressed in this manuscript are the authors’ own and do not reflect the views of the Canadian Longitudinal Study on Aging.