
Abstract
INTRODUCTION:
Breast granular cell tumour (GCT) is a rare but usually benign lesion.
PRESENTATION OF CASE:
We report a case of a woman with breast GCT.
CONCLUSION:
Clinically and radiologically, GCT may mimic breast carcinoma. A conclusive diagnosis is made after a histopathological examination of the lesion. The treatment of choice is surgery.
Introduction
With a clinical and radiological resemblance to breast carcinoma, the granular cell tumor (GCT) is often misdiagnosed as a carcinoma [1]. GCT is a rare benign breast tumor approximating 1:1000 of all breast tumour cases [2]. With a myogenic origin, it is assumed to be derived from Schwann cells [3]. GCT typically arises from the interlobular breast tissue, and most patients report GCT in the upper inner quadrants compared to breast carcinomas, which usually occur in the upper outer quadrant [2,4]. Core biopsy and extensive histopathological evaluation are the golden standards, as the infiltrative growth pattern on ultrasound and mammography can be misleading, and suggestive of malignancy [4]. Malignant granular cell tumours (MGCTs) have been observed in 1–2 percent of observed cases [2,5]. Therefore, distinguishing GCT from other breast tumours and establishing a benign subtype is of paramount.
In line with the SCARE (Consensus-based Surgical Case Report Guideline) criteria, we report a case of 63-year-old female with left breast granular cell tumour [6].
Case presentation
A 63-year-old female had, within the last six months, noticed a growing lump in her left breast. On physical examination the lump was a 20 × 20 mm palpable, well-defined fixated mass on the lateral part of the sternum, by the xiphoid process, towards the left breast (Fig. 1). There were no visible indications of axillary lymphadenopathy, inverted nipple, or Paget’s changes. Aside from a sister who had had breast cancer, her medical history was unremarkable. Bilateral mammography revealed even glandular tissue, density type three without tumour forming density or suspected microcalcifications (Fig. 2). The palpable tumour was not included in these recordings. Ultrasound revealed an ill-defined hypoechoic mass of 22 mm without increased doppler signal (Breast Imaging Reporting and Data System Score, BI-RADS 5, Fig. 3). No further changes were observed in the breast, and there were no pathological lymph nodes. A core needle biopsy was performed. Upon histopathological evaluation, a benign granular cell tumour was confirmed.

The 20 mm palpable, well-defined fixated mass on the lateral part of sternum by the xylephoid process, on clinical examination.
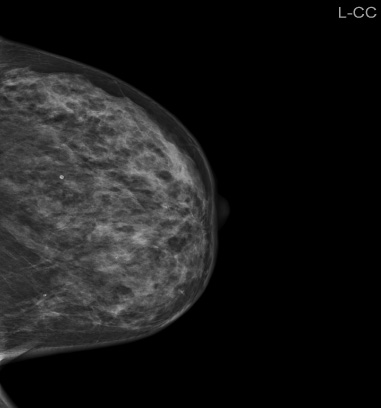
Mammography. No focal tumour is seen.
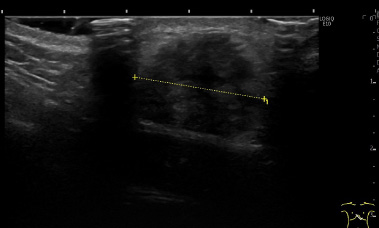
Ultrasound. An ill-defined hypoechoic process of 22 mm.
Radical excision of the tumour revealed a 27 mm granular cell tumour. Macroscopically the tumour was oval, homogenous, tan in colour and had regular borders (Fig. 4). Microscopically it was composed of scant fibrous stroma with sheets and trabeculae of oval to polygonal cells with abundant eosinophilic granular cytoplasm and round, uniform nuclei with distinct central nucleole. There was scant mitotic activity and no atypical mitotic figures. Tumor cells infiltrated adjacent subcutaneous fat and breast tissue with focal perineural involvement (Fig. 5). Tumor cells showed strong and diffuse cytoplasmic positivity for S-100 protein, moderate cytoplasmic positivity for cluster of differentiation 68 (CD68) and nuclear positivity for Transcription factor E3 (TFE3). Epithelial marker Cytokeratin 7/19 (CK7/19) was negative, as well as Estrogen receptor and Human epidermal growth factor receptor 2 (HER2). Ki67 proliferation index was low (1%). Tumor infiltrated <1 mm to the resection margins, but not directly on the ink. Postoperative diagnosis of benign granular cell tumour was confirmed. No further treatments were initiated, and the patient is scheduled for radiological follow-up in 18 months.
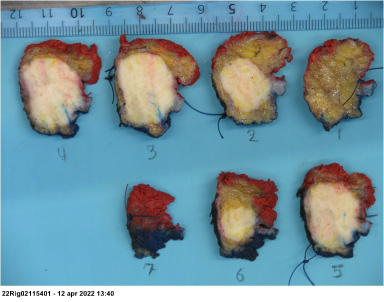
Histological tissue sections of the benign granular cell tumour.
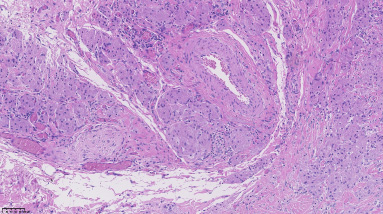
Microscopic image of the tumour, displaying close relation to neurovascular bundle (Hematoxylin-Eosin, 20×).
Granular cell tumours (GCT) are rare lesions. By reviewing the literature, it is clear, that almost all articles related are either case reports or small case series. GCT is generally a benign, solitary tumour; however, cases have also revealed malignant subtypes or present at multiple lesions [3,7]. GCT can occur at any anatomical sites [3,7–9].
Most cases are reported in women; however, cases are observed in both sexes [3,7]. GCT usually occur in adults, although paediatric GCT have been reported [3,8–10]. Patient history, clinical examination, imaging studies and histopathological examination play an important role in the diagnosis of breast GCT.
Usually, patients complain of a painless, mobile, round breast mass [10,11]. Breast ultrasound and mammogram are initially used to establish the presence of a lesion, where additional breast magnetic resonance imaging (MRI) is added.
The findings of breast imaging in GCT cases are non-specific [12], as tumours can appear well- or ill-defined, with stellation or spiculation, as in breast carcinomas [7,8,10,11,13]. Calcifications are usually absent [7,10,13].
On ultrasound, GCT presents as a heterogenous mass, well- or ill-defined lesion with variable vascularisation [7,11]. In some cases, a hyperechogenic halo may also be present [11]. On an MRI scan GCT appears as tumour with low to intermediate signals in T1 weighted images and often not visible in T2 weighted images [7,8,11]. However, on positron emission tomography/computed tomography (PET/CT) scanning GCT does not show increased metabolic activity and can thereby be differentiated from malignant tumours [7]. In our case, the tumour was fast growing and fixated to the chest wall, which mimicked malignant disease. Moreover, it would have been difficult to differentiate from breast cancer by imaging only.
The diagnosis of the GCT is confirmed by histopathological examination. Macroscopically the lesion would appear firm, yellow and with spiculated margins [14]. Microscopically, nests and sheets of large polygonal cells, abundant eosinophilic granular cytoplasm and small, round to oval eccentrically located nuclei would be present [3,10,14]. Immunostaining for S-100 protein would also be highly positive in GCT [3,7,9,10,12,13,15].
Treatment of benign GCT is wide surgical excision [7,9,10,16,17], and complete surgical excision is considered curative [17]. Prognosis is good [7], however there is a risk for local recurrence when surgical margins are positive [3].
Conclusions
The diagnosis of breast GCT is complicated due to its rarity and non-specific clinical and radiological findings. The definitive diagnosis is only confirmed by histopathological examination. Clinicians must be aware of GCT diagnosis, otherwise it can lead to overdiagnosis and overtreatment, especially when GCT coexists with a malignant lesion of the breast and can be considered a satellite.
Footnotes
Conflict of interest
None.