
Abstract
INTRODUCTION:
Breast adenomyoepithelioma is a very uncommon tumor, which is generally considered to be benign, however malignant transformation has been reported.
PRESENTATION OF CASE:
We report two cases of two women with breast adenomyoepithelioma.
CONCLUSION:
Diagnosis of adenomyoepithelioma is challenging because tumor may mimic other breast diseases. It has neither specific clinical signs nor radiological features, and the diagnosis is based on histopathological examination of the lesion. The treatment of choice is surgery. The type of surgery depends on the tumor factors and breast size. In malignant cases treatment such as radiotherapy, chemotherapy, immunotherapy may be used as well. It is very important to give an adequate treatment, otherwise the risk of tumor recurrence, growth or even metastatic spread, when tumor has malignant potential, increases.
Introduction
Adenomyoepithelioma is an uncommon breast tumor characterized by epithelial and myoepithelial differentiation [1]. World Health Organization (WHO) divides adenomyoepithelioma into benign and malignant tumors [2]. Most cases are reported in female, but it may occur in either sex [3]. Usually, it appears in women in their sixties [4]. Adenomyoepithelioma presents as a solitary, palpable mass [4] and definitive diagnosis can only be made by histopathological examination of the lesion. No standard treatment exists due to small number of cases.
All articles related to breast adenomyoepithelioma are usually case reports or small case series. Radical surgical excision is the treatment of choice; however, radiotherapy, chemotherapy or immunotherapy may be used in malignant cases as well.
In line with the SCARE (Consensus-based Surgical Case Report Guidelines) criteria we report two cases of 55- and 56-year-old women with breast adenomyoepithelioma [5]. We want to remind physicians to keep in mind that adenomyoepithelioma might be a differential diagnosis when examining a tumor in the breast.
Case report no. 1
A 55-year-old female presented with a 3-months history of a lump in the right breast. She had no allergies, no other diseases or relevant family history, denied taking any special medications and was not a habitual smoker or drinker.
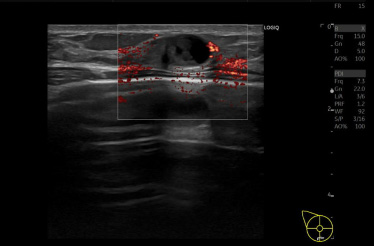
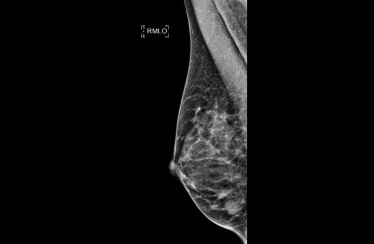
During the physical examination a 20 mm hard process was found in the lower inner quadrant of the right breast. The mammogram (MG) showed dense fibroglandular tissue without tumor masses bilateral (Fig. 1). An ultrasound scan (US) revealed a 16 mm, suspect lesion in the right breast (BI-RADS 5 (Breast Imaging-Reporting and Data System), Fig. 2). Core needle biopsy of the lesion demonstrated atypical histologic features without malignancy (papilloma).
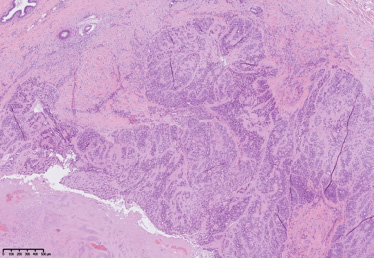
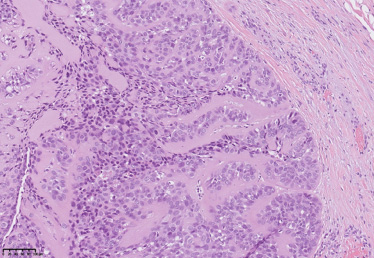
It was decided to perform an excision of the tumor. Radial skin incision over the tumor was done and a firm, well circumscribed lesion was removed. Intraoperative margin evaluation was not performed due to the non-malignant diagnosis in preoperative biopsy. Histopathological examination of the surgical material revealed a multilobular process. It consisted of glandular and cribriform structures of ductal cells surrounded by prominent layer of abluminal cells with abundant clear cytoplasm and oval nuclei with slight variation in size. The tumor showed focal squamous metaplasia and small areas of necrosis as well as acute and chronic inflammation. Mitotic activity was variable up to 8 mitoses per high power field. No atypical mitotic figures, infiltrative growth or overt cytological atypia were noted. (Figs 3 and 4). Ductal cells showed positive immunohistochemical reaction for CK18, CK7 and few cells were positive for Oestrogen receptor. Abluminal cells showed positive immunohistochemical reaction for SMMS-1, CK5, p40, p63, S100, Vimentin and focally CD10. Subsequent molecular analysis with Oncomine Comprehensive Assay showed point mutations in 2 loci of PIK3CA gene (c.1258T>C, p.C420R, c.3140A>G, p.H1047R) and no MYB rearrangement. A diagnosis of adenomyoepitelioma was made as the previously mentioned features were not regarded as sufficient for diagnosis of frank malignant potential. The patient was discussed at the Multidisciplinary Team (MDT) conference. Because of a 1 mm distance to the medial resection margin, re-resection was performed. Optimal margins around the tumor (more than 5 mm) were reached during the secondary, and no evidence of residual tumor was found in the re-resected material.
Once more the patient was discussed at the MDT conference. It was decided that the tumor was removed radically, and no adjuvant treatment was required. The patient’s postoperative course was uneventful, and the patient was satisfied with surgical outcome and cosmetic result.
There was no recurrence after one-year follow-up.
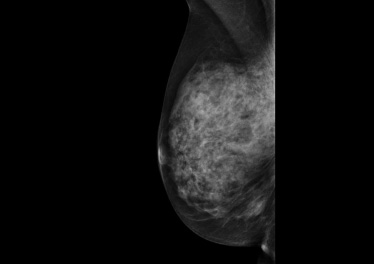
Right sided mammogram of normal breast tissue.
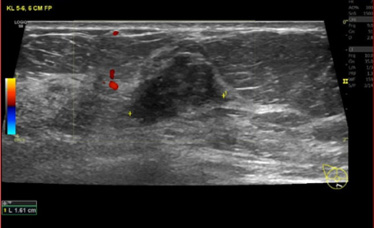
Ultrasound revealed a 16 mm lesion in the right breast.
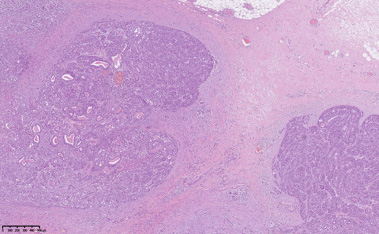
Microscopic image of the adenomyoepithelioma, showing multilobular architecture and pushing borders in fibrous stroma (Hematoxylin-Eosin, 50×).
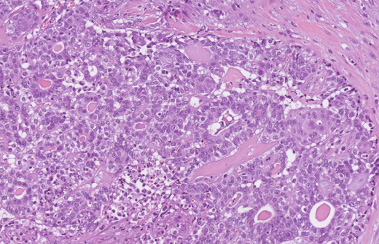
Glandular and cribriform structures of myoepithelial and epithelial cells (Hematoxylin-Eosin, 200×).
A 56-year-old woman with a history of a ductal adenoma of the right breast surgically removed in May 2019 presented with a 25 mm palpable tumor in the middle of the two lower quadrants consistent with the site of prior surgery. Her past medical history was non-significant, she had no allergies and was not a habitual smoker or drinker. The patient’s mother was diagnosed with breast cancer at the age of 68.
The MG and an US revealed a newly emerged benign tumor (BI-RADS 3, Figs 5 and 6) measuring 17 mm on the MG and 15 mm on the US. Biopsies of the tumor showed features of adenoma or adenomyoepitelioma and were categorized as an atypical histological finding according to the guidelines of Danish Breast Cancer Cooperative Group (DBCG).
Diagnostic surgery (radial incision) with broad margins was performed resulting in the removal of a firm, well-circumscribed, gray-tan tumor. Histopathological examination revealed a multinodular tumor consisting of fibrotic stroma and rounded epithelial structures in jigsaw-puzzle configuration, featuring ductal cells, prominent layer of myoepithelial cells and surrounded by thick basal membrane-like material. Myoepithelial cells were strongly positive for Cytokeratin 5 and Actin immunohistochemical staining while ductal cells were positive for Cytokeratin 7 and 18. A minor component of spindle cells and focal tumor infarction were noted. Histological features were consistent with an adenomyoepithelioma (Figs 7 and 8). Tumor was removed with safety margin of 9–10 mm.
The patient was discharged the same day and had an uncomplicated postoperative period. There was no recurrence after a one-year follow-up.
Ultrasound showed a 15 mm tumor in the right breast.
17 mm tumor was found on the right sided mammogram.
Microscopic image of the tumor 2, showing rounded epithelial-myoepithelial structures in fibrous stroma (Hematoxylin-Eosin, 50×).
Ductal and myoepithelial cells arranged in jigsaw puzzle (Hematoxylin-Eosin, 200×).
Breast adenomyoepithelioma is a very rare breast disorder, which is generally considered to be benign or to have a low-grade malignant potential. However, malignant transformation can arise in extremely rare cases [6–9]. In metastatic cases hematogenous spread is more common than the spread via the lymphatic system with lungs, brain and bones as the target organs [6,10]. The age range of adenomyoepithelioma is from 22 to 93 years with the average age of onset around 60 years [4,8,11–13]. Patients usually present with a solitary, palpable, well-circumscribed tumor, measuring from 0,3 cm to 17 cm [1,8,12,13].
Patient history, symptoms, clinical examination, imaging studies and histopathological examination play an important role in the diagnosis of adenomyoepithelioma. However, the diagnosis of adenomyoepithelioma might be difficult to obtain due to non-specific findings in the breast imaging and a low incidence of this tumor [1]. On a MG adenomyoepithelioma usually appears as an oval or a round isodense mass [1,14–16]. Calcifications might be seen on MG [14], and the tumor might be occult on MG due to a very dense breast tissue [1,15]. On an US adenomyoepithelioma presents as a well-circumscribed, solid, or combined solid and cystic mass [14]. Due to a better characterization of the tumor when using MRI scanning (Magnetic resonance imaging) this examination may be performed [3,16]. In malignant cases CT scanning is recommended for disease staging [3].
The origin of the tumor is confirmed by histopathological examination. Histopathologically adenomyoepithelioma appears as a well-defined, circumscribed or multilobulated mass featuring a biphasic growth pattern. Glandular or tubular structures of ductal cells are surrounded by outer layer of conspicuous myoepithelial cells with clear cytoplasm. Myoepithelial cells may sometimes show spindle cell morphology and/or intraductal growth. A dense hyaline matrix surrounding epithelial structures is sometimes reported [17]. Luminal cells may show mild to moderate nuclear atypia without atypical mitotic figures or necrosis [1]. The immunohistochemical profile of an adenomyoepithelioma follows a biphasic pattern, where luminal cells are positive for CK7, EMA, CK9, CK19 and outer cells show typical pattern of myoepithelial differentiation (positive staining for S100, SMA, smooth muscle myosin heavy chain, p63, CK5, CK14). Adenomyoepithelioma may feature a unique inverted staining pattern with high molecular weight cytokeratins with strong positivity in luminal cells and a negative stain in myoepithelial cells [18].
The differential diagnosis of adenomyoepthelioma includes its malignant counterpart and other types of benign and malignant breast lesions. A malignant adenomyoepithelioma is a rare entity and is believed to derive from a pre-existing classic adenomyoepithelioma [19]. Malignant change occurs in the luminal and/or myoepithelial cells in the form of frank cytological atypia, increased and atypical mitoses, necrosis and infiltrative growth. A malignant epithelial component may present as invasive breast carcinoma of no special type, invasive lobular carcinoma or other special type carcinoma, while a malignant transformation of myoepithelial cells would show features of myoepithelial cell carcinoma such as infiltrative overgrowth of spindle or plasmacytoid cells. Adenomyoepithelioma should also be differentiated from intraductal papilloma, nipple adenoma, tubular adenoma, sclerosing adenosis and invasive carcinoma [1,8,9].
No standard treatment exists due to adenomyoepithelioma’s rarity. Surgical options vary depending on the size, localization and pathological features of the tumor. Wide local excision with adequate margins is recommended [8,10,11] and is considered curative in benign cases [20–22]. However, there are reported cases of distant metastasis from adenomyoepitheliomas without histological atypia or increased mitotic activity [11]. Adenomyoepithelioma might be treated with wide local excision with adequate margins as the recurrence is rare, however mastectomy with or without sentinel lymph node biopsy might be performed if malignant transformation is diagnosed [8,23,24]. Adjuvant therapy might be used in specific cases [4,8]. Recurrent benign adenomyoepithelioma might be associated with malignant potential and more aggressive behaviour, which is why it should be treated cautiously [20,25].
The prognosis is good for benign adenomyoepithelioma [1]. The expected 5-year overall survival (OS) for patients with a diagnosis of malign adenomyoepithelioma is 74.4% [4]. Older age (≥80) and non-surgical treatment is associated with worse OS, however neither the use of RT nor systemic therapy is associated with improvement of OS [4].
Due to the risk of metastatic spread some authors recommend a long follow up of malignant adenomyoepithelioma [3].
Conclusion
Breast adenomyoepithelioma is a rare and mostly benign breast lesion, which should be considered in differential diagnosis with other breast diseases. Radiological imaging is non-specific, and adenomyoepitheliomas diagnosis can only be confirmed by histopathological examination. There are no guidelines for the treatment of adenomyoepithelioma due to its rarity, however wide surgical excision with or without SN biopsy is recommended.
Learning points/take home messages
Breast adenomyoepithelioma is a rare tumor, which diagnosis is based on histopathological examination. Inadequate treatment can result to tumor recurrence, growth, or even metastatic spread, when tumor has malignant potential. The prognosis is good for benign lesion. Further studies in this area are needed.
Contributors
Lina Pankratjevaite – conception and design, data collection and writing the paper.
Katrine Lind – writing the paper.
Giedrius Lelkaitis – writing the paper.
Marco Mele – critically revised the article.
All authors have read and approved the final version of the manuscript.