
Abstract
Introduction
Haemorrhagic breast necrosis is an extremely rare, but severe condition.
Presentation of case
We report a case of a 56-year-old woman who suffered from spontaneous haemorrhagic breast necrosis. To our knowledge, it is the first published case of breast haemorrhagic necrosis in Denmark.
Conclusion
The diagnosis of spontaneous haemorrhagic breast necrosis is challenging because of its rarity. It is crucial to consider the past medical history of the patient. In particular, if the patient is currently on anticoagulant therapy. Information of complete and accurate family medical history and possible genetic mutations must be obtained. Clinical examination plays an important role in the diagnosis of haemorrhagic breast necrosis.
Introduction
Haemorrhagic skin necrosis is a condition where the death of skin and subcutaneous tissue occurs and is the result of thrombosis of small blood vessels. 1 Sudden thrombosis of the skin vessels may be caused by haemostasis, injury to the vascular endothelium, or hypercoagulation. 2 Mutations or deficiencies of the anticoagulant factors may be associated with haemorrhagic skin necrosis. 3 Necrosis can also occur as a result of anticoagulant treatment, as there have been reported cases of Warfarin-induced skin necrosis (WSN). 4 WSN is a rare but severe reaction and typically occurs 3–10 days after the initiation of anticoagulant therapy with an incidence of 0.01%–0.1%. 5
In line with the SCARE (Consensus-based Surgical Case Report Guidelines) criteria, we report a case of a 56-year-old woman with idiopathic haemorrhagic spontaneous breast necrosis. 6
Case report
A 56-year-old woman with a background of ulcerative colitis and Factor V Leiden mutation was admitted to the Department of Breast Surgery with signs of infection in the left breast. Treatment with Dicloxacillin had been initiated by the general practitioner with sparse effect. Upon admission, the patient received daily treatment with Stelara (Ustekinumab), Prednisone, and Warfarin due to comorbidities.
When admitted to the hospital, the patient complained of severe pain in the left breast. During clinical examination, the left breast was swollen and with discolouration (Figure 1). Furthermore, the patient was febrile and had raised inflammatory markers. A breast ultrasound was performed and showed inflammation and no signs of abscesses (Figure 2). The antibiotic treatment was supplemented with Ciprofloxacin and Benzylpenicillin. Despite this treatment, the discoloured area of the breast expanded to the flank and turned blackish. A specialist in infectious diseases was consulted due to the use of immunosuppressants for ulcerative colitis. The infectious disease specialist suspected that the severity of the infection was masked by immunosuppressants and recommended to change the antibiotic treatment to Cefuroxime. Day 4 of hospitalization. Ultrasound upon admission.

The affected area of the breast developed haemorrhagic bullae and necrosis of the underlying tissue. A CT scan was performed, which did not show development of gas in the affected area nor signs of a possible abscess. Diagnosis of necrotizing fasciitis was considered and the need for surgical revision was discussed as the patient initially had experienced severe pain. The consensus among all attending surgeons was that the presence of circulatory stability, absence of fever, and only mild pain during examination did not justify the need for surgical revision. It was instead decided to continue conservative treatment. Despite the absence of bacterial growth in any of the cultures, the antibiotics were changed to the more broad-spectrum Meropenem and Clindamycin.
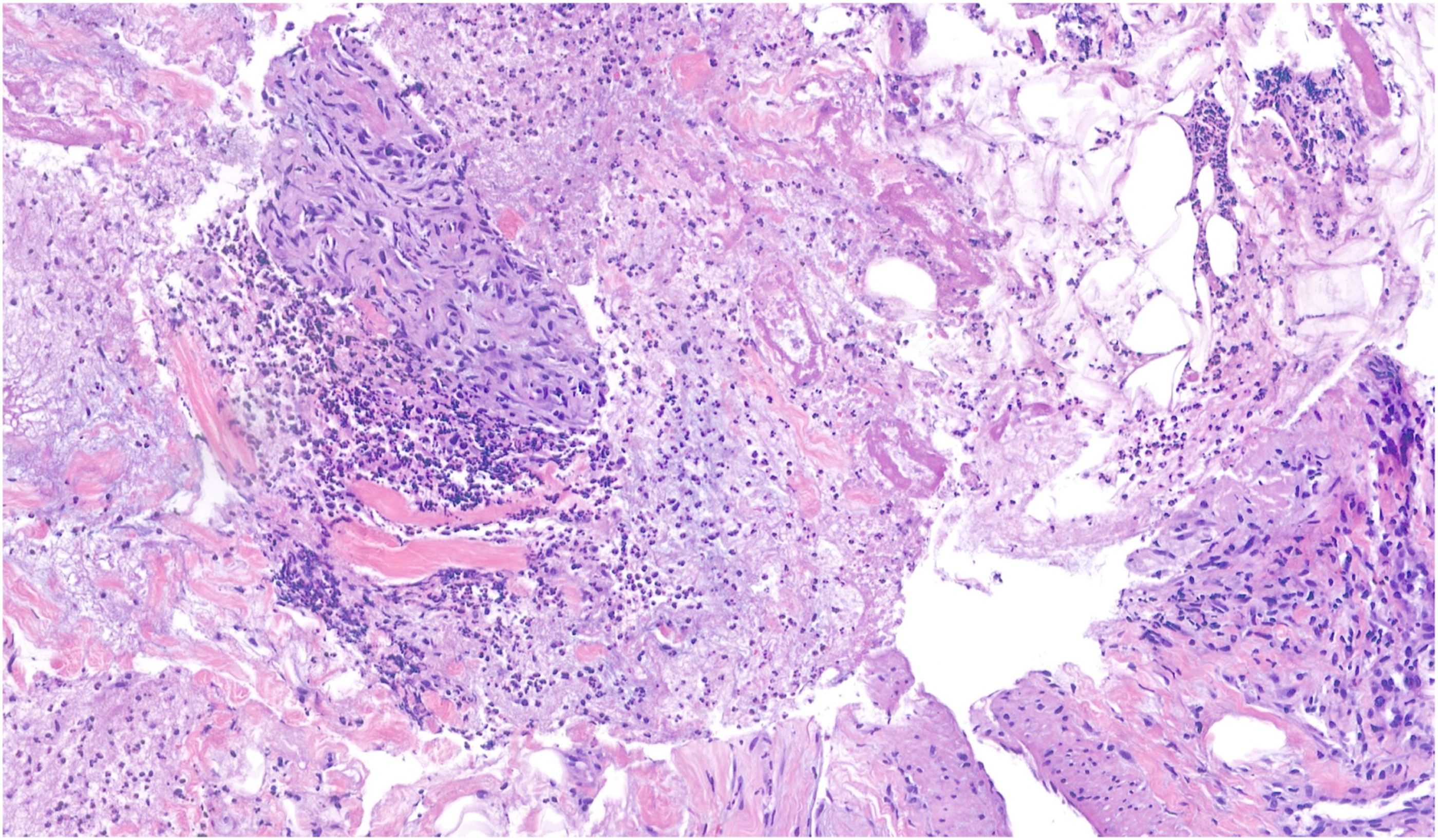
At this point, the infection markers started to decrease and the area changed to a dry necrosis (Figure 3). However, the patient experienced thrombocytosis, which was discussed with a haematologist, who believed it was a reaction to the current circumstances. Up until this point, there had been no signs of an abscess on ultrasound examination, and therefore, a decision was made to take random biopsies to rule out underlying cancer. The biopsies showed acute inflammation, necrosis, and fibrin thrombosis (Figure 4). Day 8 of hospitalization. Histology of the biopsy.
Following consultation with a haematologist, it was decided to switch from Warfarin to a high dose of Tinzaparin (12.000 IE/day) due to suspicion of WSN. The patient was discharged after 19 days of hospitalization to follow-up in the outpatient clinic (Figure 5). The patient was last seen at the Department of Breast Surgery 3.5 months after the onset of symptoms and only a small remnant of the dry necrosis persisted. Day 18 of hospitalization.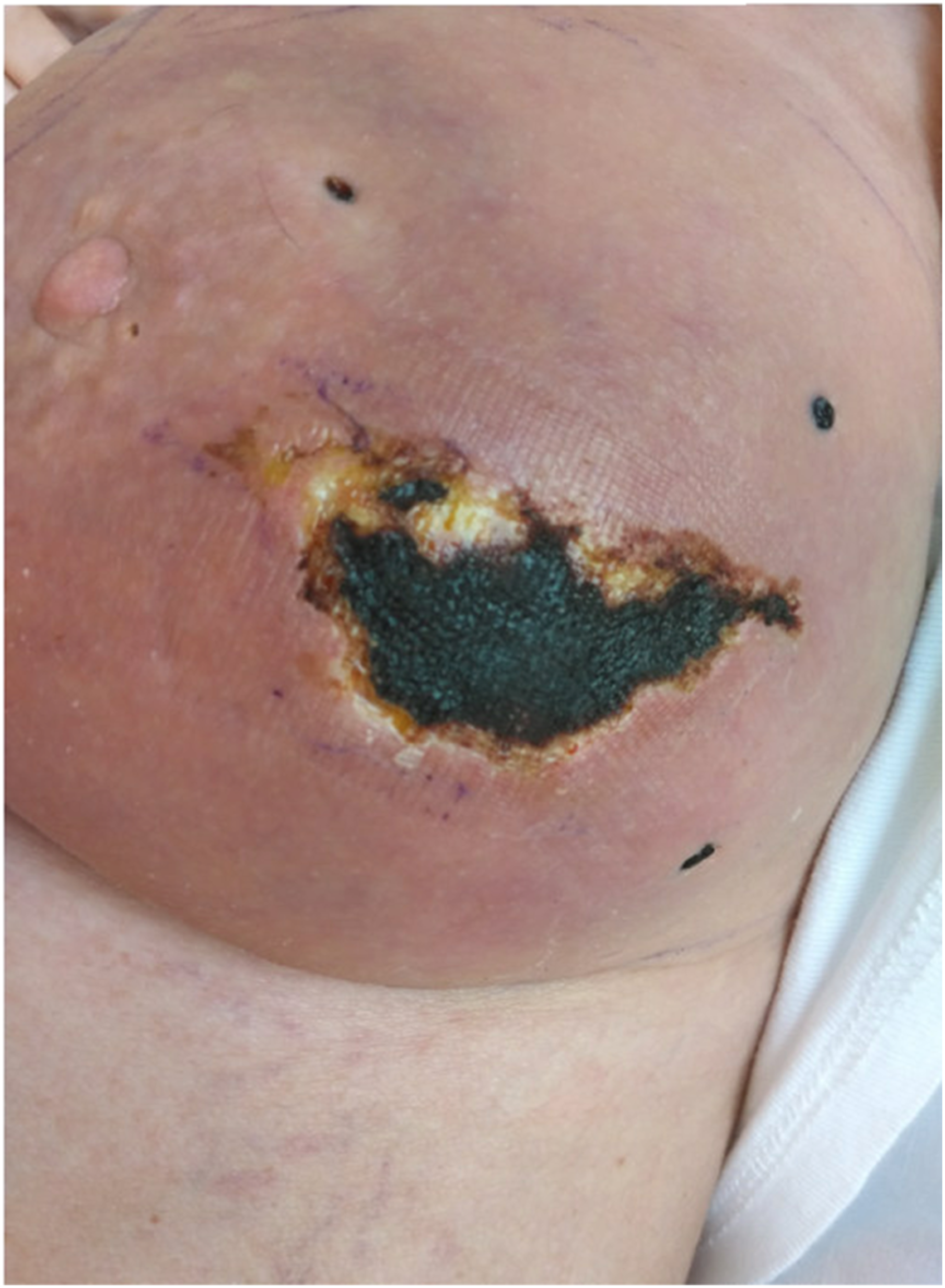
Discussion
Spontaneous haemorrhagic breast necrosis is a rare yet serious condition. It is crucial to initiate the necessary investigations and accurately diagnose the condition promptly to prevent any delay in the management of the patient.
Spontaneous haemorrhagic breast necrosis is frequently linked to an underlying hypercoagulable state. 1 The majority of cases involving this condition develop quickly following the start of anticoagulant treatment with Warfarin. 5
Calciphylaxis, disseminated intravascular coagulation syndrome, haematoma, purpura fulminans, venous thrombosis, necrotizing fasciitis, cellulitis, snake venom induced skin necrosis, decubitus ulcers, cryoglobulinemia, inflammatory breast cancer, warfarin induced skin necrosis should be considered as differential diagnosis.4,7–10 To differentiate between the above-mentioned differential diagnosis, a combination of histological evaluation and thorough review of the clinical history, including the timing of onset, distribution of lesions on the skin, and laboratory results can be used. 7 Skin necrosis induced by warfarin typically presents with paraesthesia and a sensation of pressure, accompanied by an ill-defined sudden erythematous flush. It is often painful and the lesions are well-localized. They are initially haemorrhagic or erythematous, but the accumulation of oedema in the tissues results in a peau d’orange effect that delineates the border of the lesions. 9 Other diseases also exhibit distinct characteristics; purpura fulminans can manifest in the paediatric population following an infection but may also affect adults presenting with shock, fever, and gangrene. 7 Necrotizing fasciitis is identified by its rapid progression of deep cutaneous infection, high mortality rate, and early positive results in wound culture and tissue Gram stain. 7 Cutaneous calciphylaxis is marked by calcium deposition in vessel walls, intimal hyperplasia, and fibrin thrombosis in capillaries and small to medium dermal vessels, particularly occurring in patients with end-stage renal disease undergoing haemodialysis. 7
In this case, the patient received Warfarin treatment and had a Leiden factor V mutation. However, there is no conclusive evidence to suggest that either the treatment or this condition was the cause of the necrosis. The triggering factor in our case was difficult to identify. We believe that this case of spontaneous haemorrhagic breast necrosis was idiopathic.
Prompt diagnosis of haemorrhagic breast necrosis and identification of its aetiology is crucial. The diagnosis and treatment pose challenges that necessitate the cooperation of a multidisciplinary team. The haematologists should be involved in the management of the patient with this condition. 9
If Warfarin is determined to be the cause of skin necrosis, it is recommended to discontinue its use and switch to low molecular weight heparin. 4 While skin necrosis often heals naturally over time, deeper or wider necrosis may necessitate surgical intervention. 9 Extensive breast necrosis may require debridement, skin grafting, or even wide excision. In some cases, a mastectomy may be necessary if the breast tissue is significantly affected. However, surgical excisions can result in reduced breast volume and breast deformity, with potential psychological challenges and impacts on the quality of life.
Clinicians should be aware of this serious condition, as delayed recognition and management may result in severe morbidity or even death. 5
Conclusion
Awareness of spontaneous haemorrhagic breast necrosis is essential for prompt diagnosis and management. The primary concern is determining the trigger that led to necrosis. It is crucial to promptly initiate the necessary investigations and accurately diagnose the condition to prevent any delay in the management of the patient.
Learning points/take home messages
• Breast haemorrhagic necrosis is a rare and serious condition affecting the breast. • The diagnosis and management of breast haemorrhagic necrosis can be challenging. • Further studies in this area are needed.
Footnotes
Author contributions
All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.