
Abstract
BACKGROUND:
Endocrine treatment for breast cancer acts largely by inhibiting tumor cell proliferation. The biomarker Ki67 is linked to the proliferative index of the tumour.
OBJECTIVE:
To identify the factors affecting the fall in Ki67 value in early-stage hormone receptor (HR) positive breast cancer patients receiving short-term preoperative endocrine therapy in an Indian cohort.
METHODS:
Women with hormone receptor positive, invasive, nonmetastatic, and early breast cancer (<T2, <N1) were assigned to short-term preoperative tamoxifen 20 mg daily (pre-menopausal women) or Letrozole 2.5 mg daily (post-menopausal women) for a minimum of 7 days after noting the baseline Ki67 value from the diagnostic core biopsy specimen. The postoperative Ki67 value was estimated from the surgical specimen, and the factors determining the extent of fall were evaluated.
RESULTS:
The short-term preoperative endocrine therapy resulted in a reduction in the median Ki67 index, which was significantly greater among postmenopausal women who received Letrozole (63.25 (31.94–80.5)) than among premenopausal women who received Tamoxifen (0 (−28.99–62.25)) (p-value 0.001). The fall in Ki67 value was particularly marked for patients with low-grade tumors with high Estrogen and progesterone receptor expression (p-value < 0.05). The duration of treatment (<2 week or 2–4 week or >4 week) did not affect the fall in Ki67.
CONCLUSION:
Preoperative therapy with Letrozole resulted in a more significant fall in Ki67, as compared to therapy with Tamoxifen. Determining the fall in Ki67 value in response to preoperative endocrine therapy could provide an insight into the response to endocrine therapy in luminal breast cancer.
Keywords
Introduction
Breast cancer is the most frequently diagnosed cancer and the leading cause of death from cancer in women worldwide [1]. The 2020 global cancer statistics showed that approximately 2.3 million women were diagnosed with breast cancer, representing 11.7% of all cancer cases [2]. In India, 1,62,468 new cases and 87,090 deaths were reported for breast cancer in the year 2018 [3]. Hormone receptor-positive (HR+) breast cancers comprise the most common types of breast cancer, accounting for 75 percent of all cases [4].
HR+ breast cancer responds well to endocrine therapy (ET). Historically, tamoxifen was the first drug used as primary endocrine therapy which demonstrated tumor shrinkage either obviating the need for or deferring surgery [5]. This was particularly favored for older, postmenopausal women with co-morbidities. The advent of aromatase inhibitors (AIs) led to comparisons of letrozole versus tamoxifen and the demonstration of the greater efficacy of the AIs over tamoxifen [6]. The ATAC trial evaluated disease-free survival in the adjuvant endocrine therapy settings, and the patients who received anastrozole resulted in a significant increase in time to recurrence compared with tamoxifen in postmenopausal women with hormone-sensitive tumors [7]. The PO24 trial confirmed the superiority of 4 months of neoadjuvant letrozole over tamoxifen in 337 patients with early breast cancer who were initially not eligible for breast conservation surgery. In HR+HER2+ disease, the superiority of letrozole over tamoxifen was even more significant, with an overall response rate of 88% versus 21% [8]. There is limited evidence on the role of neoadjuvant ET in premenopausal women. AIs are not used as a single agent for those with intact ovarian function, though they may be combined effectively with ovarian function suppression or ablation for appropriate antiestrogen therapy [9].
Currently, neoadjuvant chemotherapy is offered to patients with locally advanced breast cancer [10]. There is now sufficient evidence that neoadjuvant chemotherapy may even lead to a complete pathologic response, and this allows us to gauge the in-situ response of the tumour to chemotherapy [11]. This line of thinking can be extrapolated to evaluate if neoadjuvant ET can aid in assessing the response of the tumour to Letrozole or Tamoxifen.
In India, there is often a 2–4-week window between diagnosis and surgery. The acceptable interval between diagnosis and the primary treatment is not well-defined in the literature, however, initiating treatment within 4 weeks of diagnosis is usually considered acceptable. This window serves as an opportunity to incorporate endocrine-based therapy into clinical practice [12]. This represents the duration of time patients often have to wait before primary breast surgery while they arrange finances and leave from work, therefore having little, or no impact on the time to surgery. The preoperative window period gives us the opportunity to administer therapeutic modalities to gauge the in-situ response of the tumour by evaluating the change in certain specific biomarkers [13,14]. This approach is most validated in the setting of early-stage HR+ breast cancer using Ki67 as a biomarker, following short-term preoperative endocrine therapy (PoET) [15,16].
In the IMPACT trial,suppression of the proliferation marker Ki-67 after 2 and 12 weeks was significantly greater with anastrozole than with tamoxifen among postmenopausal patients [17].
Identifying a reliable, relatively inexpensive, and reproducible biomarker to assess the change in tumor proliferation for each patient is an important step in predicting the efficacy of adjuvant ET in HR+ breast cancer. The proliferative marker Ki67 is one of the important parameters involved in treatment decisions in breast cancer patients [18]. Originally identified by Gerdes et al., Ki67 is a nuclear protein associated with cellular proliferation and is expressed in the cell nucleus during the G1, S, G2, and M phases of the cell cycle, but not in the G0 phase [19]. It is therefore considered a useful marker for breast cancer subtype classification, prognosis, and prediction of therapeutic response [20,21]. At present, all treatment is based on a single baseline value of Ki67. Thus, our study aimed to explore whether the fall in the proliferative marker Ki67 after PoET could predict endocrine responsiveness better than the single baseline Ki67 value.
Materials and methods
This prospective interventional study was undertaken in early-stage hormone-positive breast cancer patients to evaluate the effectiveness of PoET by the means of fall in the Ki67 index. Women aged 18 years and above with a good performance status (PS- 0–2) who were diagnosed with operable invasive hormone-positive early breast cancer by core needle biopsy were eligible for the study. The eligible participants were required to have their paraffin fixed core needle tissue block available. Pregnant or lactating women, patients who received chemotherapy or ET for breast or ovarian cancer in the last 5 years, and those who were not willing to participate in the study were excluded from the study. The study was approved by the Amrita Institute of Medical Science institutional ethics committee.
Eligible women with early breast cancer were approached after their core biopsy specimen had been sent for Immunohistochemistry (IHC) evaluation. The PoET was initiated before the IHC report had been established, and women whose IHC showed hormone negative were asked to stop the drug and were removed from the study. All premenopausal patients were requested to take Tamoxifen 20 mg once daily and postmenopausal patients were requested to take Letrozole 2.5 mg tablet once daily during the preoperative window period. Once the biopsy report of each patient confirmed their eligibility, the patients were asked to continue the ET till the day of surgery. This roughly corresponded to 2–4 weeks that our patients needed to complete metastatic and pre-operative work-up prior to surgery.
A core biopsy of the primary tumor which was obtained before the first dose of ET provided the Baseline Ki67 (Ki67B) value, and a representative sample of the tumor which was obtained at the time of surgery provided the Post Therapy Ki67 (Ki67T) value. Both samples were fixed in neutral buffered formalin for 6–12 hours before being embedded in paraffin. Serial sections were cut and stained, using a predefined rabbit monoclonal antibody against human Ki67 (Clone MIB-1, Dako). The percentage of the invasive cancer cells expressing Ki67 was recorded from 2–3 random fields with the highest index (hotspots) by a single expert pathologist who specialized in breast cancer pathology. Nuclear staining of any intensity was considered positive. The fall in Ki67 after the preoperative endocrine therapy was defined as below:
Statistical analysis
Statistical analysis was done using IBM SPSS 20.0 (SPSS Inc, Chicago, USA). Continuous variables were represented by Mean±SD and median (Q1, Q3). Categorical variables were expressed as frequency and percentage. To test the statistical significance of the difference in the median Ki-67 between the two drugs, the Mann-Whitney U test was used. To test the statistical significance of the changes in the median Ki-67 from baseline to postoperative findings within the two drugs, Wilcoxon Signed rank test was used. To test the statistical significance of the difference in the proportion of categorical variables between two drug groups and with the fall in Ki-67, the Chi-Square test was used. A p-value <0.05 was considered statistically significant.
Result
During a period of 9 months between October 2021 and June 2022, 124 newly diagnosed breast cancer women who fulfilled the study criteria were identified and 119 were eligible for the final analysis. Among them, 86 (72.26%) were postmenopausal women who received preoperative letrozole and 33 (27.73%) were premenopausal women who received preoperative tamoxifen. Demographic details of the study population are presented in Table 1.
Patient characteristics
Patient characteristics
DCIS Ductal carcinoma in situ, ER estrogen receptor, HT Hormone therapy, NST no special type, PR progesterone receptor.
The women were representative of the population with operable early-stage HR+ breast cancer. Five patients with a very weak hormone receptor (ER/PR <10%) status were initially included in the study. All of these patients showed a poor response to the endocrine therapy with no fall or an increase in Ki67 index after therapy. These patients were not included in the final analysis dataset. Among the eligible population, patients who received letrozole exhibited a better response to therapy when compared to those who received tamoxifen (p-value 0.001). Over half of the patients (n = 18, 54.54%) who received tamoxifen had an increase or no fall in their proliferation index after the therapy. However, among patients who received letrozole, only 10 (11.62%) patients showed a poor response to the endocrine therapy. Among the study participants, 36 (30.25%) patients received PoET for less than 2 weeks, while 68 (57.14%) received ET for 2 to 4 weeks and 15 (12.6%) received it for more than 4 weeks.
Change in Ki67 index
IQR interquartile range, Ki67B Ki67 at baseline, Ki67S Ki67 after surgery, n number of patients.
Tissue sections of both the biopsy sample and surgical specimen to estimate the Ki67 index was available for all 119 enrolled subjects. A large majority of postmenopausal women (n = 72, 83.72%) showed endocrine responsiveness with at least a 10 percent fall in Ki67 with short-term preoperative letrozole, while among premenopausal women who received preoperative tamoxifen, only 15(45.45%) patients showed endocrine responsiveness (fall in Ki67 > 10%). Of all the enrolled subjects, 14 (11.76%) patients showed a fall of >90%, of which 13 were postmenopausal women. In addition, 17 (14.28%) patients showed a fall of 80–90% of which 14 were postmenopausal women. In the study cohort, 14 (11.76%) of them presented with low Ki67 at baseline (Ki67B < 10%). Among them, 6 (42.85%) were premenopausal and 8 (57.14%) were postmenopausal women. After PoET, in patients with low Ki67B, the Post Therapy Ki-67 (Ki67T) value remained low in 12 patients, and two patients’ Ki67T values had become high. 78 postmenopausal women and 28 premenopausal women had tumors that had a high Ki67B. After subjecting postmenopausal women to preoperative letrozole therapy, 42 patients’ Ki67T became low (<10%). However, 36 of them continued to have a high Ki67T value after therapy. Among premenopausal women with High Ki67B, only 5 patients’ Ki67T value became low after their preoperative window period, whereas 22 remained High (Ki67T > 10%). The median average fall in Ki67 index after preoperative endocrine therapy in our study population was 63.25 (31.94–80.5) with Letrozole and 0 (−8.99–62.25) with Tamoxifen (p-value 0.001). The fall in Ki67 index in patients who received PoET is presented in Table 2. Percentage of fall in Ki67 in patients receiving Letrozole or Tamoxifen is represented graphically in Fig. 1, highlighting the trend that a higher percentage of fall in Ki67 was noted among patients on Letrozole.
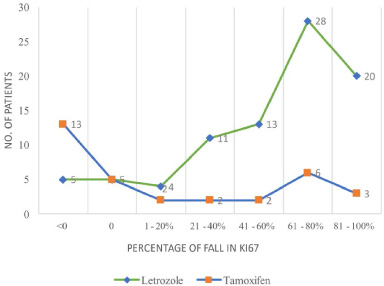
Percentage of fall in Ki67 in early-stage hormone positive breast cancer patients receiving preoperative letrozole among postmenopausal women and preoperative tamoxifen among premenopausal women.
In our analysis, the fall in Ki67 index was more marked among postmenopausal women who received Letrozole than among premenopausal women who received Tamoxifen. There was a statistically significant correlation between the fall in Ki67 after preoperative letrozole with tumor grade (0.034), Estrogen receptor (ER) status (p < 0.001), and progesterone receptor (PR) status (p < 0.005). The decrease in proliferation seen with 2 weeks of PoET was similar to that seen in 4 weeks or more duration. Results are shown in detail in Table 3.
Factors affecting Fall in Ki67 index
DCIS Ductal carcinoma in situ, ER estrogen receptor, HT Hormone therapy, NST no special type, PR progesterone receptor.
The present study analyzed the effect of short-term PoET on breast cancer proliferation, as assessed by the change in the percentage of cells expressing the Ki67 index. In addition, the factors associated with the fall in Ki67 were also evaluated. A review of the literature reveals that the addition of a short-term PoET resulted in a significant reduction in Ki67 in the postoperative surgical specimen [23,24]. Our study aimed at analyzing this trend among HR+ early breast cancer patients in the Indian context.
The study uses fall in Ki67 index, a proliferative marker, in HR+ early breast cancer patients receiving PoET to determine the subset of patients who are likely to respond well to ET. An important corollary would be to be able to identify the subset of patients in whom the disease can recur while on ET. The TAILORx Trial, which evaluated 6419 post-menopausal women with early breast cancer identified only 982 (15.29%) patients having a Recurrence Risk Score >26, necessitating chemotherapy. Among the 3300 premenopausal women with early breast cancer, 407 (12.33%) patients had a Recurrence Risk Score >26 [25]. Where relevant, multigene prognostic assays like Oncotype Dx and Mammaprint are used to determine the recurrence risk in patients, which can guide the need for chemotherapy in these patients. However, in developing nations, this is far from possible due to financial and time constraints. Analyzing the fall in Ki67 in these patients could help identify those patients who may respond poorly to ET and may therefore benefit from adjuvant chemotherapy to prevent disease recurrence [26].
In our analysis, we found that the duration of the therapy did not influence the fall in the Ki67 index with either letrozole or tamoxifen therapy. The decrease in Ki67T observed with 2 weeks of endocrine therapy was similar to that seen with 4 weeks or more duration. Our study therefore reiterates that it would be sufficient to treat patients with a short duration of 2 weeks of therapy to identify the endocrine-sensitive patients.
The proliferative marker Ki67 has a predictive and prognostic significance in early-stage breast cancer. Previous clinical trials focusing on the proliferative changes of PoET use a 10 percent cut-off to distinguish between low and high Ki67 index since this value gives more transparency to tumor characteristics and reduces the impact of inter-observer variability [22,23]. Our study evaluated the proliferative index at the baseline and after the preoperative window period to evaluate endocrine responsiveness. Our study revealed that PoET resulted in a significant fall in the proliferation marker, with nearly half of the patients (59, 49.57%) having a Low Ki67T after the preoperative endocrine therapy. The establishment of a decreasing trend in Ki67 during the primary treatment period may predict improved outcomes in the adjuvant setting. This observation reflects the findings of the study done by Ianza A et al., which concluded that the percentage fall in the proliferation index was strongly associated with the clinical response. The majority of participants of this study also recorded a significantly longer disease-free survival (DFS), with a fall in the Ki67 index between baseline and end of treatment greater than 60% associated with a prolonged recurrence time [26]. The POETIC trial classified patients also evaluated the impact of preoperative endocrine therapy, and classified patients into 3 categories based on the fall in Ki67: the Low-Low group, the High-Low group, and the High-High group. The trial showed that 5-year recurrence risk among women belonging to the Low-Low group was 4.5 (2.9–6.3), 8.4 (6.8–10.5) in the High-Low group, and 21.5 (17.1–27.0) in the High-High group [23]. In our study, among the women who received Tamoxifen, 5 (15.15%) women belonged to the Low-Low group, 5 (15.15%) women belonged to the High-Low group, and 22 (66.67%) women belonged to High-High group. Among the women who received Letrozole, 7 (8.13%) women belonged to the Low-Low group, 42 (48.83%) women belonged to the High-Low group, and 36 (41.86%) women belonged to High-High group. Categorizing women with luminal early breast cancer into these groups could allow us to tailor adjuvant therapy based on their endocrine responsiveness. Greater Ki67 variation could indicate a greater susceptibility of the tumor to ET, which could translate to prognostic significance.
Our study recorded a significant reduction in the expression of the Ki67 index in post-menopausal HR+ early breast cancer patients after short-term preoperative letrozole in our population, and the results were concordant with existing literature. Ian Smith et al., have reported that postmenopausal HER2-ve breast cancer patients receiving 2 weeks of preoperative AIs showed a decrease in Ki67 by a median % change of 76.8 as compared to the control group 5.3% [23]. On the other hand, short-term preoperative tamoxifen in premenopausal women did not result in a significant fall in Ki67T value. This was in contrast to the findings of the POWERPIINC trial by Adam L Cohen et al., which reported the changes in tumor proliferation index after 7 days of preoperative tamoxifen and observed a Ki67 decrease of 40% [27 ]. Similarly, a significant reduction in the Ki67 index (median change from 7.9 (42.9) to 1.8 (40.7)) was observed with 4 months of tamoxifen in another trial by Mathew J Ellis et al. [28 ]. This further highlights the need for population-based studies to determine the characteristics of breast cancer biology and response to therapy within the Indian context.
The proliferation index on residual tumors holds additional prognostic importance. Ianza A et al. have reported a poorer DFS and a reduction in the overall survival in patients with a high Ki67 value on residual tumors after treatment [26]. Similarly, our results reflect that greater attention should be given to the percentage decrease in Ki67, which could indirectly assess the in-situ response of the tumor to endocrine therapy. Considering the possibility of tumor heterogeneity in patients, this would be a more inclusive and patient-oriented approach that could promote precise and personalized medicine. A reduction in the proliferative index after PoET may indicate a less aggressive tumor, a more stable response over time with adjuvant endocrine therapy, and in turn, longer survival [26,29]. This could also provide an early indication of endocrine sensitivity or resistance in early-stage HR+ HER2-ve breast cancer patients in whom adjuvant chemotherapy is not routinely considered. Furthermore, this could be an inexpensive approach to help our clinicians to make decisions regarding adjuvant chemotherapy, in patients who cannot afford multigene prognostic assays.
Our study also aimed to determine the clinical and pathological factors influencing the fall in Ki67 index. A study by Madani SH et al. concluded that a higher Ki67 index had a direct significant correlation with higher grade, P-53 positivity, and HER2 positivity [30]. In our study, we found that the tumor grade, ER status, and PR status showed statistical significance with the fall in Ki67.
The limitation of our study was that the Ki67 value was interpreted for each patient by one of two expert pathologists specialized in breast pathology, both of whom were blinded with regard to preoperative endocrine therapy. As the Ki67 estimation is subjective, this may result in inter-observer variability. To overcome this, our study focused on determining the fall in Ki67, with an aim to decrease the observer bias. Another confounding factor is the possibility of tumour heterogeneity, which can result in variable Ki67 value within a single tumour. A control group where Ki67 value was estimated in the core biopsy specimen, as well as the surgical specimen, could help establish the concordance between the two. We acknowledge the limitations of the study, and we intend to overcome the same in our subsequent research within this avenue.
Our study is the first to evaluate the fall in the Ki67 index following preoperative endocrine therapy in the Indian context, and the results could pave way for the individualization of treatment in hormone receptor-positive early breast cancer. Hence, larger clinical trials focusing on the personalization of adjuvant treatment in HR+ HER2 -ve early-stage breast cancer patients based on the fall in the Ki67 index after a short-term preoperative endocrine therapy is warranted.
Conclusion
Neoadjuvant endocrine therapy represents an avenue that is still largely unexplored, and our aim was to understand the in-situ tumour response to endocrine therapy. Our study showed that the duration of therapy did not affect the fall in Ki67, implying that a short term therapy of 2 weeks may be enough to assess the response. Our study also concluded that the majority of postmenopausal early-stage HR+ breast cancer patients responded well to preoperative letrozole and had a significant fall in the Ki67 value. However, 10 (11.62%) postmenopausal women did not show a reduction in their proliferative index after preoperative therapy, suggesting that this could be a subset of HR+ patients who are inherently poor responders to ET. Furthermore, it may be possible that these patients could benefit from adjuvant chemotherapy. This can be confirmed with large clinical trials analyzing the concordance of fall in the Ki67 index in patients receiving PoET with a multigene prognostic test like Oncotype Dx, which could predict the need for adjuvant chemotherapy in patients. On other hand, 18 (54.54%) premenopausal women did not show a reduction in Ki67 index after preoperative tamoxifen, suggestive of poor response to tamoxifen over letrozole. Other than menopausal status, other factors that influenced the fall in Ki67 were ER, PR expression and grade of the tumour.
We recommend further research to verify the significance of the fall in the Ki67 index in patients receiving preoperative Letrozole, with a prime focus on validating the fall in Ki67 with established multigene prognostic assays. Long-term follow up of these patients is also warranted, to give further insight into recurrence patterns based on fall in Ki67 index.
Footnotes
Conflict of interest
This study was conducted in the absence of any external funding and there is no conflict of interest