
Abstract
Breast cancer is a heterogeneous disease with different tumor subtypes. Identifying risk categories will help make better treatment decisions. Hence, this study aimed to predict the survival outcomes of invasive breast cancer in Vietnam, using St Gallen 2007 classification. This study was conducted on 501 patients with breast cancer who had surgical operations, but had not received neoadjuvant chemotherapy, from 2011 to 2013. The clinicopathological characteristics were recorded. Immunohistochemistry staining was performed on ER, PR, HER2/neu, and Ki67 markers. For HER2/neu(2+), fluorescence in situ hybridization was used as the test. All patients with breast cancer were stratified according to 2007 St Gallen categories. Kaplan-Meier and log-rank models were used to analyze survival rates. There were 3.8% cases classified as low risk (LR), 72.1% as intermediate risk (IR1: 60.1% and IR2: 12.0%), and 24.1% as high risk (HR1: 11.8% and HR2: 12.3%). Patients who were LR had the best prognosis, with a 5-year overall survival (OS) rate of 100%. Intermediate-risk patients were at 92.3%. High-risk patients had the worst prognosis, with a 5-year OS proportion of 69.3% (P < .05). For disease-free survival (DFS), risk categories were categorized as LR: 100%, IR: 90.3%, and HR: 69.3% (P < .05). Three main risk categories of breast cancer had a distinct OS and DFS. These findings suggest that the 2007 St Gallen risk category could be used to stratify patients with breast cancer into different risk groups in Vietnam.
Introduction
Breast cancer (BC) is a heterogeneous disease with different tumor subtypes that varies in prognosis and response to therapy. Adjuvant chemotherapy reduces the risk of recurrence, with effects that are proportionally greater for younger women, but are only slightly affected by nodal status, grade, or the use of adjuvant endocrine therapy. 1 -5 These findings led a National Institutes of Health consensus panel to recommend adjuvant chemotherapy for most patients, a practice that has contributed to declining BC mortality. 6,7 However, the majority of patients with early-stage BC may receive chemotherapy unnecessarily. Nowadays, there are many molecular classifications in BC which are commonly applied in selecting the exact adjuvant treatment, such as the 2013 St Gallen. 8 The 2005 and 2007 St Gallen international expert consensus conference described risk categories and provided recommendations for treatment of early-stage BC. 9 In 2005, patients were categorized into 3 risk groups: low risk (LR), intermediate risk (IR), and high risk (HR), depending on the nodal status. 10 After that, more features were added to this stratification and the modified version was published in 2007. 9 Patients with BC were then stratified into LR, IR, and HR. The IR category is subdivided, mainly based on the presence/absence of 1 to 3 positive nodes (absent: IR1, present: IR2). High risk is separated into 2 subgroups, based on the number of positive nodes (1-3 lymph nodes: HR1, 4 or more lymph nodes: HR2). These risk categories were used to help make decisions about the suitable adjuvant treatment and distant recurrence prediction. Adjuvant systemic treatment regimens are decided based on these risk groups. Basically, chemotherapy is recommended for patients who are at IR or HR while only endocrine therapy is recommended for patients at LR. 9
Although there has been much progress in diagnosis and treatment, BC is still the most common cause of cancer-related deaths in women in Vietnam. 11 To improve the survival of patients, it is very important to make more suitable decisions on the adjuvant treatment after operating for BC, especially in the early stages of the disease. This requires an essential need for the application of the appropriate treatment protocols that are used in Vietnam for managing patients with BC. Vietnam is a developing country; therefore, majority of patients with BC couldn’t spend a lots of money in the expensive molecular tests, so it is important to select tools of risk classification that are appropriate in terms of both expense and value in selecting exactly the adjuvant treatment. The 2007 St Gallen risk categories may be a good candidate and this classification hasn’t applied yet in Vietnam to identify risk groups. Hence, this study aimed to predict the survival outcomes of invasive BC in Vietnam, using St Gallen 2007 classification.
Methods
Patients and Samples
This is a follow-up study of 501 operable female infiltrating patients with BC aged 14 and 87 years, from 2011 to 2013, at the National Cancer Hospital (NCH), Vietnam. The NCH is the largest hospital specializing in oncology diagnoses, treatment, screening, prevention, and control in Vietnam. The patients who got the second malignant tumors or had neoadjuvant chemotherapy were excluded. All patients were noted for clinical information, such as age, location of tumor, and date at initial diagnosis, which were extracted from medical patient charts and records. Of them, 134 were diagnosed with BC at younger than 45 years and the other 65 cases were older than 65. All patients were operated on to remove the tumor by modified radical mastectomy, combined with axillary lymph node dissection. Tumors were measured in maximum diameter. The pathological tumor-node-metastasis (pTNM) staging of BC was staged, basing upon criteria by the American Joint Committee on Cancer (seventh edition). 12 Tumor and nodal samples were done via pathological tests.
After surgery, 477 of the cases were treated by adjuvant chemotherapy. All hormone receptor–positive cases were also received by endocrine therapy. Among HER2-positive BCs, only 2 patients were able to pay all expenses for target treatment by trastuzumab. All personal information was removed or disguised to ensure patient anonymity.
Histopathology
All patients with BC were operated on to remove tumors by modified radical mastectomy. Then specimens were transferred to the pathology department. Samples were collected with the minimum ischemic time (30-60 minutes) and fixed in 10% neutral formalin for 24 hours. Nodal and tumor samples were obtained by routine pathological techniques such as hematoxylin and eosin staining. Experienced pathologists evaluated all histopathological features such as tumor size, histopathological type, grade, nodal status, and peritumoral lymphovascular invasion (LVI). Immunohistochemistry staining was used with D2-40 marker to confirm LVI. Histopathological types were classified according to 2012 World Health Organization classifications. 13 Histologic grades were assigned according to Elston and Ellis. 14 The Nottingham Prognostic Index (NPI) was calculated for all BCs using the formula: NPI = 0.2 × tumor size (cm) + lymph node stage (1, 2, or 3) + histological grade (1, 2, or 3). 15
Immunohistochemistry and Fluorescence In Situ Hybridization
All immunohistochemistry (IHC) staining were tested for formalin-fixed, paraffin-embedded tissue sections. The IHC method was performed by Ventana-automated machine, using ER, PR, HER2, and Ki67 markers. We used the primary monoclonal mouse antihuman estrogen receptor (Ventana-SP01; Roche company), monoclonal mouse anti-human c-erbB-2 oncoprotein, rabbit monoclonal (Ventana-4B5; Roche company), and confirm anti-Ki67 monoclonal rabbit antibody (Ventana-30-9; Roche company), respectively. The Allred score was used to assess ER and PR status. Breast cancers were scored as ER/PR positive if the total Allred score for ER/PR was >2/8. Now, according to College of American Pathologists/American Society of Clinical Oncology (CAP/ASCO) guidelines, ER/PR positive has been altered to 1%. 16 The UK recommendations were used for assessment of HER2 expression. 15 A HER2 score of 3 plus was considered HER2 positive or overexpression. Ninety-six (19.2%) patients who had an IHC HER2 score of 2+ were tested by fluorescence in situ hybridization (FISH) to identify amplification of the HER2 gene. 17 There were 21.9% HER2 gene amplification by FISH. Several different cut points for Ki67 have been proposed. At the 2011 St Gallen consensus meeting, Ki67 index was divided into 3 levels: low (≤15%), moderate (16%-30%), and high (>30%). 18
IHC Molecular Classification and Risk Categories
All patients were classified into molecular subtypes and risk categories based on age, clinicohistopathological, and IHC data. Molecular types that follow St Gallen 2013 are Luminal A (LUMA), Luminal B HER2(−) (LUMBH−), Luminal B HER2(+) (LUMBH+), HER2, and triple negative (TN). 8 This approach uses IHC criteria for its definition of estrogen and progesterone receptor, the detection of HER2 overexpression and/or amplification, and Ki67 index, to identify molecular subtypes.
Risk categories were grouped by following St Gallen 2007. Initially, patients were categorized into 3 risk groups: LR, IR, and HR, based on the nodal status. 19 After that, more clinicopathology and IHC features were added to this stratification and the modified versions were published in 2007. 9 Risk categories of patients with BC were classified as LR, IR, and HR. The IR category was subdivided into IR1 and IR2 and HR was separated into HR1 and HR2.
Follow-Up and Outcomes
Overall survival (OS) was calculated as the date of diagnosis to the date of death from BC or the last available date before loss of follow-up. 20 If a patient died from other diseases, it would be censored. Death dates of the patients were obtained from death certificates issued by the commune government in Vietnam. Radiological and/or histopathological data were used to confirm the recurrence and dates. Patients who died without any recurrence were censored to the date of death. 20 Disease-free survival (DFS) was calculated as the date of surgery to the date of the recurrent BC diagnosis or BC-specific death, which included locoregional and distant recurrences. 20
Our 144 patients were followed up to evaluate recurrence or death up to 7 years. The mean follow-up time was 72.1 ± 15.7 months. The actual minimum and maximum follow-up period were 12 and 92 months (>7 years), respectively. Approximately one-tenth of the 144 patients were followed up after more than 4 years from the date of initial diagnosis (4.2% for 24 months, 1.4% for 36 months, 3.5% for 48 months, and 7.1% for 5 years or more). There were 18 patient deaths and 3 distant metastasized alive patients. One hundred twenty-three patients were alive and free of disease.
Statistical Analysis
All of our patients were categorized into groups using criteria from the 2007 St Gallen list of risk categories: LR, IR, and HR. The IR and HR categories were subdivided into IR1 and IR2, and HR1 and HR2, respectively. The Pearson χ2 test, likelihood ratio, and Fisher exact test were performed to determine the clinicopathological differences between the groups. The Kaplan-Meier model was employed to evaluate the 5-year OS and DFS, according to the LR, IR, HR, and IR/HR subgroups. A log-rank test was used to compare survival curves. A P value <.05 was considered as statistically significant. All of the analyses were conducted using SPSS version 19.0 statistical software.
Results
Baseline Clinicopathological Features and Risk Categories
This study was composed of all 501 patients with BC who had undergone operations. Table 1 shows the patients’ baseline clinicopathological features. The median age at diagnosis was 50 years. Most patients were between the ages of 40 and 60 years. Young BCs (67.3%) and left lateral BCs (53.9%) were more common than older BCs and other lateral BCs, but they were not significantly different from risk category. With regard to pathological features, more than half (53.7%) of the patients had large tumors that were more than 2 to 5 cm in size (diameter). Less than half (36.1%) of the cases had positive ipsilateral axillary lymph nodes. Of all, 12.3% of the patients had more than 3 metastasized axillary lymph nodes. High histological grade, moderate NPI, and stage II were the most common (52.7%, 59.2%, and 68.9%, respectively). Low Ki67 index rate was the highest, which was accounted in 42.1%. Luminal A tumors were the most common (28.7%), followed by LUMBH− (23.6%), TN (22.7%), and HER2 (15.8%). Only 46 (9.2%) patients had LUMBH+ tumors.
Baseline Clinicopathological Features in 501 Operated Patients With Breast Cancer.

Abbreviations: LVI, lymphovascular invasion; NOS, not otherwise specified; NPI, Nottingham Prognostic Index; pTNM, pathological tumor-node-metastasis; TN, triple negative.
The italics are not significantly different.
There were 19 (3.8%) cases classified as LR, 362 (72.3%) cases as IR, and 20 (23.9%) as HR. Among the IR group, 301 (60.1%) were node negative (IR1) and 61 (12.2%) had up to 3 positive nodes (IR2). For the HR group, 58 (11.6%) had 1 to 3 positive axillary lymph nodes (HR1) and 62 (12.3%) had 4 or more positive lymph nodes (HR2).
Clinicopathological Features of Different Risk Categories
To evaluate the relationship between clinicopathological features and risk categories, all patients with BC were classified into 3 main risk groups: LR, IR, and HR subgroups (according to 2007 St Gallen). Table 2 displays the relationship between clinicopathological features and risk categories for invasive BC. Patients aged more than 50 years were more common in the LR category (50-59 years and 60-69 years: 36.9% in both), while those aged from 40 to 60 years were more common in IR and HR groups. In young and older groups, no trends were observed in risk category by young and older groups, as well tumor location. A significant difference was observed in age group, tumor size, and grade to risk groups (P < .001). There were 4 (0.8%) tumors located bilaterally, and they belonged to IR1, IR2, and HR2 subgroups.
Associations of Risk Categories and Clinicopathological Features in 501 Operated Patients With Breast Cancer.

Abbreviations: HR, high risk; IR, intermediate risk; LVI, lymphovascular invasion; NOS, not otherwise specified; NPI, Nottingham Prognostic Index; pTNM, pathological tumor-node-metastasis; TN, triple negative.
The italics are not significantly different.
aFisher exact test.
bLikelihood ratio.
cPearson χ2 test.
Regarding tumor size and histological grade, tumors with ≤2 cm in size and grade I were only seen in LR categories, and IR and HR subgroups were more common than other risk categories in size group >2 to 5 cm (56.5%, 60.0%, 50.8%, and 53.2%) and grade III (45.2%, 53.3%, 72.9%, and 85.5%), respectively. For risk groups, characteristics of histopathology type and NPI were significantly different (P < .001). A good NPI only appeared in the LR group. In contrast, IR1, IR2, and HR1 were the most common for moderate NPI. A poor NPI indicated the largest proportion of HR2 tumors (87.1%). More tumors with a low Ki67 index displayed LR and IR1 disease (63.2% and 47.5%, in turn). On the contrary, HR1 and HR2 having a high Ki67 index was more common (56.6% and 48.4%, respectively).
In addition, a statistical difference was observed between risk groups and molecular subtypes in the pTNM stage (P = .001). Low-risk tumors were found only in LUMA and LUMBH− subtypes (52.6% and 47.4%, respectively), while HR1 and HR2 had more HER2 subtypes (33.9% and 27.4%, respectively) and TN subtypes (37.3% and 37.1%, respectively). Low-risk tumors were the most common in stage I (78.9%). High-risk tumors were not existent in this stage. In opposite, HR2 patients had the highest proportion of stage III tumors. However, IR1, IR2, and HR1 had more stage II tumors (72.1%, 91.7%, and 88.1%, in turn).
Survival
The 5-year OS rate for these operated-on patients with BC was 85.01 ± 1.61 months, while their 5-year DFS was 71.04 ± 1.39 months. Survival curves according to different risk groups are summarized in Figure 1. Patients who were in the LR categories had the best prognosis, with an OS rate in the 5-year follow-up of 100%. Intermediate risks were at 93.2%. By contrast, those in the HR categories had a clearly reduced 5-year OS proportion (69.3%). These differences were statistically significant (P < .05). Figure 2 shows a statistically significant difference of 5-year OS rates, according to 5 different risk groups (P < .05). The 5-year OS rate of HR1 was higher than that of HR2 (76.5% vs 64.9%, respectively). However, IR subgroups and HR subgroups did not affect OS (P = .292 and P = .650, in turn), perhaps due to a small sample size (Figures 3 and 4).

Five-year relative overall survival of low, intermediate, and high risks according to St Gallen categories for invasive breast cancers. The log-rank test shows that there was a significant difference between these 3 survival curves.
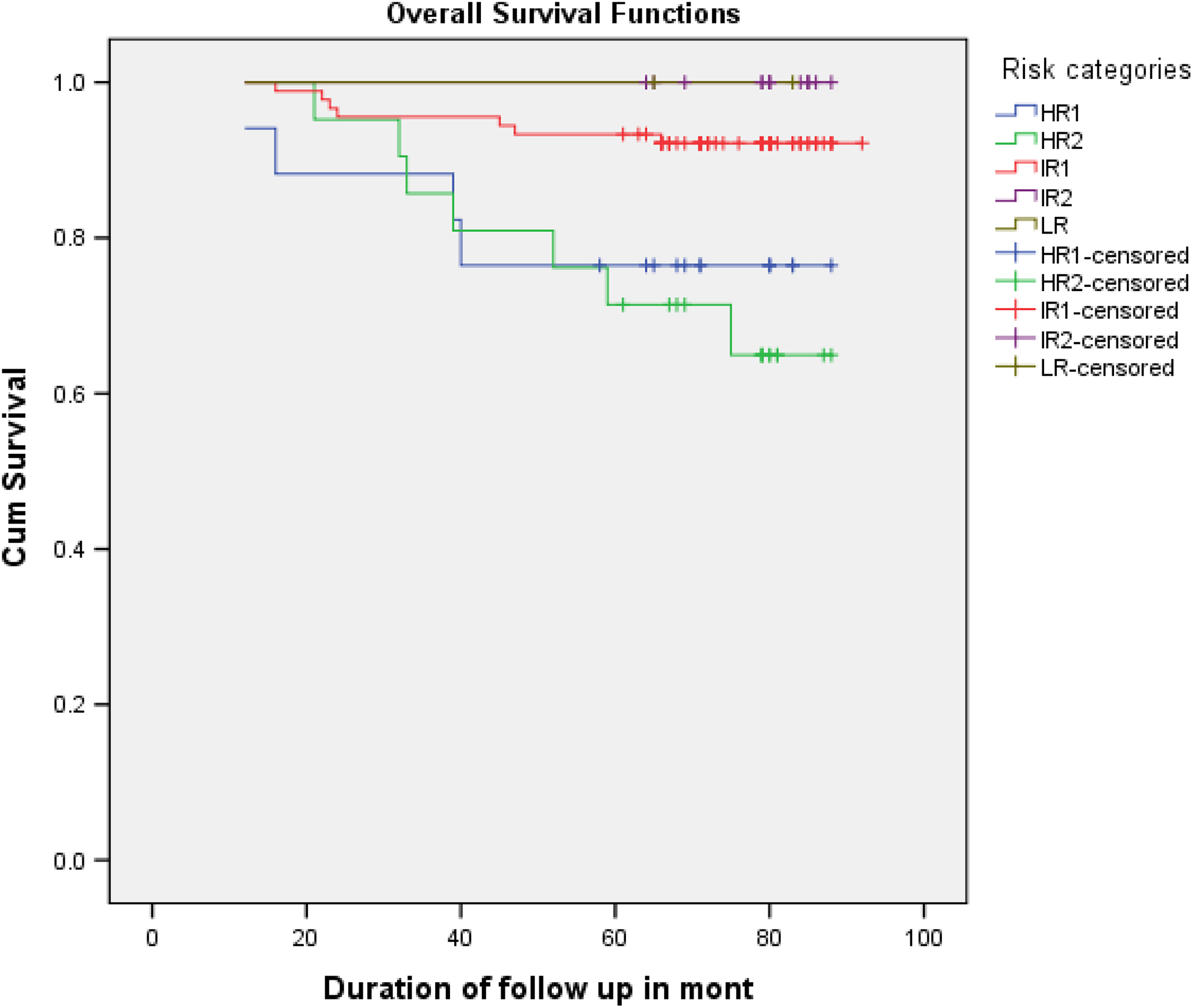
Five-year relative overall survival of low risk, intermediate risk (IR1, IR2), and high risk (HR1, HR2) according to St Gallen categories for invasive breast cancers. The log-rank test indicates that there is a significant difference between these 5 survival curves.

Five-year relative overall survival of intermediate-risk subgroups (IR1, IR2), according to St Gallen categories for invasive breast cancers. The log-rank test exhibits that there is not a significant difference between these 2 survival curves.

Five-year relative overall survival of high-risk subgroups (HR1, HR2) according to St Gallen categories for invasive breast cancers. The log-rank test shows that there is not a significant difference between these 2 survival curves.
Disease-free survival curves, according to different molecular subtypes, are shown in Figure 5. A significant difference was observed in the 5-year DFS rate according to risk groups (P = .01 < .05). The DFS rates in the 5-year follow-up of the patients who were in the LR and IR categories were 100% and 90.3%, respectively. On the contrary, patients in the HR categories had the lowest 5-year DFS proportion (69.3%).

Five-year relative disease-free survival of low, intermediate, and high risk according to St Gallen categories for invasive breast cancers. The log-rank test demonstrates that there is a significant difference between these 3 survival curves.
Discussion
Breast cancer is a heterogeneous cancer that exhibits variable clinicopathological features and survival according to different age groups, races, and regions. The prognosis of patients with BC has improved recently. 19,21 Multiple regimens of chemotherapy further reduces BC mortality rates when it is given in addition to endocrine therapy, improving the rate, on average, by one-third. 2 However, not all women with ER-positive tumors will benefit from chemotherapy. This includes those with a good prognosis, taking into consideration that their endocrine therapy could not benefit meaningfully from additional treatment. When used in adjuvant decision-making, 2007 St Gallen risk categories stratify patients into LR, IR, and HR categories. Patients in the LR range are usually recommended to receive endocrine therapy alone. Those in the HR range are offered chemotherapy in addition to endocrine therapy and/or trastuzumab. There is no consensus as to the optimal treatment for those in the IR range. 9
To the best of our knowledge, we are the first in Vietnam to employ the 2007 St Gallen classification to consider its utility in prediction BC survival. One of the other strengths of this study is that the primary characteristics of all of the patients have been reviewed centrally by 2 senior pathologists. All histopathological characteristics and IHC staining used the international guidelines for the evaluation of results. The quality control of histopathology is needed to define the risk category. So pathology departments of each hospital in Vietnam should standardize the subjective criteria used for histological/nuclear grading of BCs. 8
Although adjuvant chemotherapy improves survival of early-stage BC, for some patients, the associated potential toxicities and the negative impact on their quality of life may outweigh the benefits of treatment. 1 The diverse clinical behavior of BC relates to its individual molecular pathology. Gene expression profiling can provide better risk discrimination relative to traditional clinicopathological factors and more accurately identify patients with BC in an LR group who are predicted to derive minimal benefit from chemotherapy. The ability to personalize treatment based on tumor biology and thus to reduce unnecessary chemotherapy is key to optimizing patient care. 22,23 To make better adjuvant therapeutic decisions regarding early-stage BC, different types of clinical guidelines are used. Nowadays, clinicians have a variety of resources and guidelines to assist in treatment decisions for patients with early-stage BC. 24 Adjuvant! Online, the guidelines of the National Comprehensive Cancer Network, and gene tests such as Oncotype DX, MamaPrint, Prosigna (PAM 500), or EndoPredict are well known to most oncologists. 25 -30 However, it is so costly to do these tests, especially for low- to middle-income countries such as Vietnam, that it is not suitable for routine practice. Thus, the St Gallen Consensus Statements remain a valuable tool, especially in developing countries, because of its simplicity and ease of risk determination. Every St Gallen conference since 1988 has produced treatment guidance based on available evidence and expert opinion for the therapy of patients with early-stage BC outside clinical trials. 19 Various iterations of the St Gallen Consensus recommendations have been validated, and compliance with these recommendations for systemic therapy has been shown to improve the survival of women with node-negative BC. However, refinements have been suggested and some shortcomings have been described. 31 -36 The above tools, which are included in the guidelines, are not being practiced routinely in our setting. A simple, low-cost tool is the best option for the management of patients with BC in Vietnam, as it is a developing and low- to medium-income country. A set of guidelines and recommendations for the selection of adjuvant systemic treatment based on risk categories, which were proposed by the experts in the St Gallen international consensus meeting, can be still useful for our best choices. 9,10 The findings of this study can demonstrate that the 2007 St Gallen risk categories are an useful tool for making accurate adjuvant therapeutic decisions regarding infiltrating BC, both in Vietnam and in other similar settings in the world.
In this study, the IR category is the largest of the main 3 risk categories defined in the 2007 St Gallen, including 72.1% of all patients. Low-risk patients were the smallest (3.8%), and HR patients were at 24.1% (shown in Table 1). We found that only 3.8% of the BCs were at LR, and they had a 100% 5-year OS. According to St Gallen 2005, the LR category included patients who had node-negative BC with all good prognostic features such as tumors ≤2 cm in size, grade I, no LVI, age ≥35 years, and HER2 negative. 10 However, at the 10th St Gallen expert consensus meeting in March 2007, the LR category was added to good prognostic factors such as ER and/or PR expression. 9 The features of the LR category display good prognoses for BC. Previous studies also have found that node-negative BCs have good prognoses compared to node-positive BCs, irrespective of other factors. 33,37,38
In the current study cohort, a majority of the patients belonged to the IR or HR categories. The 2 subgroups of the IR category did not have a significant survival difference (Figure 3). Use of the ER/PR/HER2 expression clearly separates the IR category into 2 different survival groups (all ER-negative). This separation persists for the node-negative subgroup (IR1) as well as the node-positive subgroup (IR2); although in the latter subgroup, the ER−/PR+/HER2− subtype is quite rare. According to the 2017 St Gallen risk categories, these subgroups (IR1 and IR2) are composed of both adverse and good prognostic features. Therefore, they seem to have nullified the effect of giving the other a similar prognosis to both subgroups. Hence, they have similar survival curves. 38
When the axillary lymph node is metastasized by BC, patients who have 1 to 3 positive nodes and at least 1 of the poor prognostic features, such as the absence of ER and PR, or being HER2 positive, 4 or more nodes are positive, irrespective of the other prognostic features, are categorized into the HR group. This group includes 2 subgroups, HR1 and HR2. 9 However, the HR category that has the worst survival rates includes 2 subsets of patients with a distinct difference in OS (Figures 1 and 2). Marked variations in 5-year survival rates are noted within the HR category, in both of the subgroups with 1 to 3 positive axillary lymph nodes (HR1) and 3 or more positive axillary lymph nodes (HR2). 37 Therefore, this study emphasized the worst survival rates of patients with 4 or more positive lymph nodes, irrespective of any other clinicopathological factors. Similar to 2 IR subgroups, in 2 HR subgroups, the difference in the 5-year OS also didn’t exhibit statistically significant data (Figure 4). The previous clinical studies, based on the 2007 St Gallen risk categories, have demonstrated that there is no significant difference between the 5-year relative survival rates of the 2 IR categories. Those with 4 or more positive lymph nodes (HR2) had poorer survival than the subgroup HR1. 37,38 Based solely on 5-year relative survival rates, there is not much difference between LR and IR, but a clear separation in the HR category is noted. Bauer et al also demonstrated this finding. 37
In the present study, the 5-year DFS was an average time as 71.04 ± 1.39 months. The relationship of DFS to risk categories is displayed in Figure 5. Low-risk tumors had a 100% 5-year DFS, IR had a 90.3% proportion, and HR had the lowest rate as 69.3%. A significant DFS difference was observed among the 3 main risk categories (P = .01). The DFS of the subgroups of the IR or HR categories did not show a significant difference. The factors that were considered for dividing the subgroups of IR and HR categories have not significantly affected the DFS of the particular subgroup. Therefore, the IR and HR categories are homogenous with regard to the DFS. 38
Peiris et al analyzed 713 patients with BC (LR: 2%, IR1: 45%, IR2: 10%, HR1: 13%, HR2: 30%). The 5-year BC OS was LR: 100%, IR: 91%, and HR: 66%, and DFS was LR: 85%, IR: 84%, and HR: 65%. Both OS and DFS curves were significantly different among the 3 risk categories (P < .001). No survival difference was evident between the IR1 and IR2 (OS: P = .232; DFS: P = .118). Both HR1 and HR2 had a distinctly difference OS (P = .033), but no difference in DFS (P = .190). 38 Iwamoto et al conducted a study of 920 node-negative invasive BCs. At 10 years, the DFS and OS rates of all patients were 84.6% and 86.7%, respectively. The DFS and OS of patients in the LR category (25 patients) both showed 100%. The DFS and OS of patients in the IR category (356 patients) showed 92.0% and 93.1%, respectively. The DFS and OS of patients in the HR category (539 patients) showed 79.4% and 82.2%, in turn, indicating a significant difference among those in the LR/IR category (381 patients; P < .001 in both). The DFS and OS of patients who had one pathological lymph node metastasis (775 patients) showed 72.7% and 75.2%, respectively, which indicates a nonsignificant difference between those in the HR category (381 patients; P = .10). 33
Peiris and Iwamoto’s studies also validated the St Gallen recommendations, particularly for patients in the HR category who should be candidates for adjuvant therapy. 33,38 The current study assessed the value of the St Gallen classification as a tool for identifying HR patients who may benefit from chemotherapy and LR patients for whom adjuvant chemotherapy may be not necessary.
Limitations of the Study
At present, there are still some limitations of this study. First, not all patients were followed up. This is due to the patient database not being systematically managed in the computer system, and in Vietnam, patients have a tendency to change their phone numbers. Therefore, it was hard to keep in contact with them when they completed their treatment. Continued follow-up and analysis of all patients are planned. Second, a majority of HER2-positive patients didn’t receive anti-HER2 therapy, and thus, the lack of anti-HER2 treatment data may have only a slight confounding effect or may have affected the survival rates of the cohort. If all these patients had received the target treatment, their survival rate would have been improved better. This is due to the majority of Vietnamese patients being poor, and insurance companies don’t cover all expenses of this therapy. Therefore, their families cannot pay for all regimen of the trastuzumab treatment.
Conclusions
The current study indicates that the 3 main 2007 St Gallen risk categories show distinct survival rates (OS and DFS). Subgroups of the IR and HR categories had indistinct survival differences. These findings suggest that the 2007 St Gallen risk categories can be used in Vietnam in routine to classify patients into different risk groups. However, it is necessary to investigate further on risk subgroups, especially subgroups of IR.
Recommendation
Considering the Vietnamese condition, we should apply the 2007 St Gallen risk stratification for identifying the risk groups for infiltrating BC.
Footnotes
Authors’ Note
All objects of the protocol’s this study was approved by the Scientific and Ethical Committee of Hanoi Medical University as number: 965/QD-DHYHN. Written informed consent was applied to all patients before enrolling them to the study. Patients could withdraw from the study at any time without any threats or disadvantages and for no stated reasons.
Acknowledgments
The authors thank Prof Tran Van Thuan, MD, PhD, so much who is Director of the National Cancer Hospital and National Cancer Institute, Vietnam, and Associate Prof Ta Van To, MD, PhD, who is head of the Biomolecular and Pathology Center, National Cancer Hospital, for their assistance and support with this study.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.