
Abstract
BACKGROUND:
Only 42% of all breast cancer patients undergoing mastectomy elect for breast reconstruction.
OBJECTIVE:
We evaluate factors impacting complications, recurrence, and mortality in triple-negative breast cancer (TNBC) patients undergoing reconstruction.
METHODS:
Reconstructive TNBC patients at a single institution from 2010 to 2020 were retrospectively reviewed. Patient demographics, cancer characteristics, reconstruction choice, and complications were collected. Statistical significance was defined at p < 0.05.
RESULTS:
A total of 131 patients were identified. Average age was 47.8 years, 50.4% were Caucasian and 36.4% were African American. Most patients had invasive ductal carcinoma (90.8%), and most underwent nipple-sparing (41.2%) or skin-sparing (38.9%) mastectomies. Twenty-one patients (16.0%) experienced postoperative complications. Patients with complications tended to be older (52.1 versus 46.9 years, p = 0.052). At mean follow-up of 52.1 months, 14.5% experienced cancer recurrence and 5.3% died. Deceased patients were significantly younger at diagnosis (42.2 versus 48.5 years, p = 0.008) and had a lower BMI compared to surviving patients (21.2 versus 26.9 kg/m2; p = 0.014). Patients younger than age 45 years had higher Ki-67 than those older than 45 years (80.0% versus 60.0%, p = 0.013). Outcomes in autologous- versus implant-based reconstruction were not significantly different.
CONCLUSIONS:
In TNBC post-mastectomy reconstruction patients, age and BMI were predictors of mortality while race, smoking history, reconstruction choice, or type of implant-based reconstruction had no significant effect on these outcomes.
SYNOPSIS:
The purpose of this study is to evaluate factors that impact complications, recurrence, and mortality in triple negative breast cancer (TNBC) patients undergoing reconstruction. We identified BMI, neoadjuvant chemotherapy, and age as predictors of complications, recurrence, and mortality in TNBC.
Keywords
Introduction
Triple negative breast cancers (TNBC) are a rare and heterogenous group of breast cancers representing only 12 to 17% of breast cancers diagnosed annually in the United States [1]. TNBC, defined as tumors that lack expression of estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor (HER) 2, are aggressive tumors with relatively poor outcomes and higher likelihoods of recurrence compared to other breast cancers (Dent 2007). Although advances in surgical resection, radiotherapy, and systemic chemotherapy have demonstrated improved long-term outcomes for TNBC [2,3], patients with this breast cancer type continue to have lower 5-year survival rates and higher rates of disease recurrence [4].
Among patients who undergo breast-conserving surgery (BCS) or mastectomy, immediate or delayed breast reconstruction is becoming a more popular option [5]. Recent literature has found that 42% of all breast cancer patients who undergo mastectomy elect for immediate or delayed breast reconstruction [6]. Although a higher quality of life and high patient satisfaction is associated with breast reconstruction, increased post-operative complications and morbidities may occur with additional surgery [7,8]. Recent literature has demonstrated that among breast cancer patients who underwent mastectomy, immediate breast cancer reconstruction was not associated with worsened survival rates or local recurrence [8,9]. However, there is a paucity of literature evaluating post-reconstructive outcomes specifically in TNBC patients. A study by Kneubil et al. found that TNBC was an independent prognostic risk factor for locoregional recurrence among breast cancer patients who elected for mastectomy and breast reconstruction [10].
Given that TNBC is associated with worse survival and recurrence outcomes, and post-mastectomy breast reconstruction for this cancer subtype is increasing in popularity, we aimed to evaluate reconstructive factors associated with complications, recurrence, and mortality. With the shift toward value-based medicine, the purpose of this study is to provide additional insight into recommendations for post-mastectomy reconstruction to better serve patients with TNBC.
Methods
After institutional review board approval (IRB# 00004330) was obtained, we performed a retrospective chart review of patients with TNBC who underwent reconstructive surgery from 2010 to 2020 in a large, single institution, urban metropolitan center. Patients who did not undergo reconstruction in the breast that had cancer were excluded. In this study, we characterized the Goldilocks procedure as a mammoplasty. Inclusion criteria included patients over the age of 18 with a biopsy-confirmed diagnosis of TNBC, who underwent surgical resection followed by reconstruction.
Data collected included patient demographics, comorbidities, tumor characteristics, reconstruction details, adjunctive medical therapies, postoperative complications, and long-term outcomes including recurrence and mortality. Postoperative complications included wound dehiscence, hematoma, seroma, infection, necrosis, venous congestion, ischemia, and flap failure within 30 days postoperatively. Statistical analysis was performed using STATA version 17.0 (StataCorp, College Station, TX, USA). Univariate Chi-square and Fisher’s exact tests were used to analyze categorical variables and t-test and Wilcoxon’s rank sum for continuous variables. Statistical significance was set at values of p < 0.05. A Kaplan–Meier analysis was conducted to evaluate survival probabilities.
Results
A total of 465 patients were diagnosed with TNBC, of which 131 (28.2%) female patients underwent reconstruction following oncologic surgery and thus were included in this study. Average age and BMI of patients was 47.8 years and 26.6 kg/m2, respectively. The majority of patients were Caucasian (n = 65, 50.8%), followed by African American (n = 45, 35.2%), Asian (n = 7, 5.5%), and Hispanic or Latino (n = 3, 2.3%). Roughly one-quarter of the patients had a current or prior smoking history (n = 34, 26.4%). Comorbidities included diabetes (n = 4, 3.1%) and connective tissue disease (n = 4, 3.1%).
Most patients had a family history of breast cancer with 27.9% (n = 34) having a 1st-degree relative and 32.0% (n = 39) having a 2nd-degree relative with breast cancer. Twenty-five patients (19.1%) had a prior history of breast cancer. The most common TNBC histology was invasive ductal carcinoma (n = 119, 90.8%). Mean tumor size at time of diagnosis was 2.3 cm. All patients undergoing reconstruction presented with either moderate-grade (n = 20, 18.2%) or high-grade (n = 90, 81.8%) tumors at time of diagnosis. The majority of patients presented with clinical stage 2 disease (n = 60, 51.3%). Only 9.9% and 0.8% of patients presented with stage 3 and stage 4 disease, respectively. Most patients received adjuvant chemotherapy (n = 69, 57.0%) and 31.5% (n = 40) underwent adjuvant radiation. Table 1 summarizes patient demographics, comorbidities, and cancer characteristics.
Triple negative breast cancer patient demographics and cancer characteristics
Triple negative breast cancer patient demographics and cancer characteristics
an = 128, bn = 129, cn = 130, dn = 122, en = 127, fn = 110,gn = 117, hn = 121. Abbreviations: BMI, body mass index; BC, breast cancer; CA, carcinoma.
The majority of patients underwent some form of mastectomy prior to reconstruction (n = 127, 97.0%) with most undergoing a contralateral prophylactic mastectomy as well (n = 91, 72.2%). The most common type of mastectomies performed were nipple-sparing mastectomy (n = 54, 41.2%) and skin-sparing mastectomy (n = 51, 38.9%). Four patients underwent lumpectomy (3.1%). Following mastectomy, the majority of patients underwent immediate reconstruction compared to delayed reconstruction (96.2% versus 3.1%). Reconstructive technique was most commonly implant-based (n = 108, 82.4%), followed by autologous-based (n = 19, 14.5%), and mammoplasty (n = 4, 3.1%). A distribution of reconstruction techniques is shown in Fig. 1, which illustrates an increasing number of autologous-based reconstruction (ABR) over more recent years. In patients who underwent immediate implant-based reconstruction, 71.3% received tissue expanders (n = 77) while 28.7% went direct-to-implant with either silicone or saline implants (n = 31). Among the eight patients who did not undergo tissue expander to implant exchange, five underwent tissue expander removal and opted not to undergo final reconstruction. One patient experienced cancer progression and never underwent final reconstruction. The remaining two patients did not have records in their charts detailing their second stage of reconstruction. In those who received tissue expanders, time to final reconstruction was most commonly within one year (n = 60, 87.0%) with the majority undergoing final implant-based reconstruction (n = 58, 84.1%). Twenty-one patients (16.0%) experienced postoperative complications within 30 days of reconstruction. Complications most commonly included infection (n = 8, 38.1%) or necrosis (n = 5, 23.8%). Mean follow-up of included patients was 51.4 ± 33.3 months. Operative and postoperative details are summarized in Table 2.
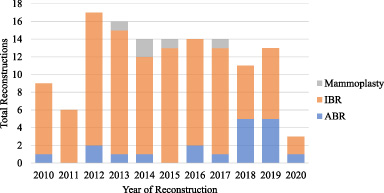
Frequency of reconstruction types in triple negative breast cancer patients from 2010–2020. Frequency of various types of reconstruction over the last decade. Abbreviations: IBR, implant-based reconstruction; ABR, autologous-based reconstruction.
Operative and postoperative details
Abbreviations: TNBC, triple-negative breast cancer; ABR, autologous-based reconstruction; IBR, implant-based reconstruction; TE, tissue expander.
Table 3 describes predictors of complications, recurrence, and mortality in our patient population. A trend was observed in older patients experiencing complications (52.1 versus 46.9 years, p = 0.052). At a mean follow-up time of 51.4 months (range 4.6 to 131.4 months), 14.5% of patients (n = 19) experienced TNBC recurrence. Those who underwent adjuvant chemotherapy were significantly less likely to develop recurrence compared to those who underwent neoadjuvant chemotherapy only (p = 0.022). Seven patients (5.4%) died. Patients who died were significantly younger at time of diagnosis compared to those who survived (42.2 versus 48.5 years, p = 0.008) and had a lower BMI compared to surviving patients (21.2 versus 26.9 kg/m2; p = 0.014). Other factors, including race, smoking history, reconstruction choice, or type of implant-based reconstruction had no significant effect on these outcomes.
Predictors of recurrence, complications, and mortality in triple negative breast cancer patients undergoing reconstruction
Abbreviations: BMI, body mass index; TE, tissue expander.
The overall survival curve using Kaplan-Meier analysis is seen in Fig. 2. Five patients died within 3 years of their reconstructive surgery, one died 4 years later, and another patient died 7.4 years after surgery. No mortality occurred after 7.4 years. The overall 3-year and 5-year survival rates were 95.1% and 93.6%, respectively.
Table 4 depicts compares cancer characteristics in our TNBC patients stratified by age. A higher Ki-67 was observed in patients who were 45 years or younger compared to patients older than age 45 (80.0% versus 60%, p = 0.13). Tumor size, grade, and stage were not significantly different between the two age groups.
Cancer characteristics in triple negative breast cancer patients stratified by age
an = 39, bn = 127, cn = 110, dn = 117.
TNBC is an aggressive subtype of breast cancer that has a higher rate of distant recurrence and mortality in women compared to most other types of breast cancer [4]. The majority of patients opt out of post-mastectomy breast reconstruction even though immediate breast reconstruction has been associated with an improved quality of life [11]. Furthermore, oncological outcomes have been shown to be similar in patients who receive immediate reconstruction compared to those who do not [12]. In our study, we found that 28% of our TNBC patients underwent post-mastectomy reconstruction, which is much lower than the reported 42% in the literature [6]. Although this finding may be affected by lack of data on patients who were lost to follow-up, this potential difference in rate of reconstruction is interesting and warranted further investigation. Notably, the distribution of reconstruction techniques used over the past decade in our cohort shows an increasing number of ABR over more recent years with the exception of 2020 when all elective cases ceased due to the COVID-19 pandemic.
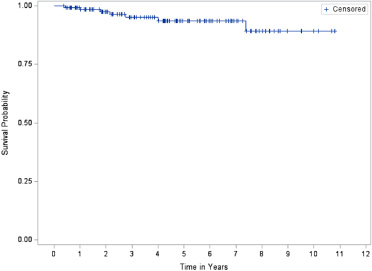
Overall survival analysis of triple negative breast cancer patients undergoing reconstruction. Survival probabilities based on Kaplan–Meier analysis. The overall survival rate for TNBC patients undergoing breast reconstruction at year 3 and 5 are 95.09% and 93.65% respectively.
Kneubil et al. previously reported that a BMI ≥ 25 and TNBC diagnosis are independent prognostic factors for locoregional recurrence after immediate breast reconstruction with a 5-year recurrence rate of 10.9% [10]. However, our findings suggest that there is no significant difference in BMI in patients with or without cancer recurrence, which should be discussed in pre-operative planning. We did see a trend towards higher BMI being associated with increased postoperative complication rates, which is expected based on previous reports [13]. It is suggested that obese women are more likely to experience complications in both autologous and implant-based reconstruction with obese women having a complications rate of 25% compared to 14% for non-obese women [13].
Interestingly, patients who died had a significantly lower BMI and younger age at diagnosis than patients who survived. This lower BMI may indicate that more aggressive cancers precipitate at younger ages. One simple explanation for this is that younger females have less percent body fat than older women which can also mean a lower BMI. One study looking at age and sex related differences in body composition observed a decrease in fat-free mass and increase in percent body fat with aging [14]. Malnutrition due to systemic therapy or progression of disease has been previously suggested as one of the possible causes for this association in mortality [15]. However, it is less likely the cause in this cohort. Nutritional markers were not explicitly collected in this patient cohort and it may be an area of interest in future studies. The mortality in younger TNBC patients undergoing reconstruction in our study is consistent with known poorer outcomes in younger TNBC patients overall. Patients younger than age 40 with TNBC have been found to have more aggressive tumors in regard to histopathological grade and Ki-67 [16]. We found that TNBC patients undergoing reconstruction who were age 45 or younger had a significantly higher Ki-67 (80% versus 60%), As a nuclear protein, Ki-67 in an indicator of tumor cell growth and proliferation and has been established as a prognostic measure of tumor aggressiveness [17]. This supports the notion that more aggressive tumors often emerge at younger ages, thus we believe the increased mortality observed in our younger TNBC patients was due to tumor aggression (Ki-67) rather than a product of reconstruction itself. Importantly, age did not have an association with cancer recurrence, which is consistent with prior studies [18–20]. While older age (52.1 years) trended toward higher complication rates compared to younger age (46.9 years), this finding was not significant. Prior studies have reported similar rates of complications in older women undergoing reconstruction compared to younger patients [18–20]. This finding may provide reassurance to older patients who are contemplating whether or not to pursue reconstruction.
Patients who received neoadjuvant chemotherapy had higher rates of recurrence compared to patients who underwent adjuvant chemotherapy in our cohort. However, this finding may be due to selection bias. The medical oncology literature has previously reported that neoadjuvant chemotherapy provides the best outcomes for TNBC given a complete pathological response; specifically, neoadjuvant chemotherapy has been found to be more effective for TNBC patients with locally advanced disease [21,22]. Recent guidelines recommend the use of neoadjuvant chemotherapy for the treatment of all patients with TNBC since TNBC patients are more likely to respond to neoadjuvant therapy than patients with ER-positive breast cancer [23]. Downstaging TNBC prior to surgery also improves cosmesis [24]. This finding in our data is likely because of a selection bias in that our cohort consisted predominantly of patients with localized disease with 87.6% having stage 2 or lower, and not those with advanced disease who have been shown to benefit even more from neoadjuvant chemotherapy. A higher powered, large multi-institutional study may help elucidate this in the future to evaluate if there is a true effect.
In regards to choice of reconstruction, we found no differences in recurrence, complications or mortality in our TNBC patients who underwent autologous versus implant-based reconstruction or reconstruction with tissue expanders versus direct-to-implant. This is consistent with other studies that have shown no significant differences between type of reconstruction, complication rates, and most patient-reported outcomes [25]. This information is valuable to aid in the decision-making process that TNBC patients will face. Additionally, when looking at overall survival, it is important to note that in TNBC patients undergoing reconstruction, the 5-year overall survival rate is 93.65%. Compared to national data for the 5-year relative survival rate for all types and stages of breast cancer of 90%, TNBC patients undergoing reconstruction tend to survive equally to other breast cancer patients [26]. Based on The Surveillance, Epidemiology, and End Results (SEER) data, the 5-year relative survival rate for TNBC specifically is 77% for all stages combined and 91% for localized disease [27]. This is consistent with our overall survival rate of 93.65% given that 73.7% of our patients with documented nodal involvement had localized disease. These findings are important because it helps reassure TNBC patients with localized disease that their mortality is not affected by their choice to pursue reconstruction.
This study was limited by its retrospective nature. In addition, the majority of our patient population presented with lower-stage TNBC; thus, our data may be more targeted to patients who inherently have better oncological outcomes. Our cohort was also noted to have a higher number of patients receiving adjuvant chemotherapy (n = 69) versus neoadjuvant chemotherapy (n = 48) for TNBC. It is well established that neoadjuvant chemotherapy is standard of care for TNBC and many of those patients who received adjuvant chemotherapy did so earlier, between 2010 and 2014, before some of the larger studies were published detailing the advances in neoadjuvant treatment of TNBC. In addition, variables such as the use of immunotherapy which may introduce additional confounding were not collected as part of the study design and should warrant further study. Additional sub analyses of risk factors for each complication were unable to be successfully completed due to low sample numbers within each category of complications. Larger scale studies of reconstructive complications in TNBC patients are warranted to determine additional risk factors unique to this population. Lastly, because TNBC is a rare disease, our study had a small sample size, limiting the power of our study. Larger, multi-institutional prospective studies are warranted to further investigate the impacts that reconstruction may have in patients with TNBC.
Overall, this study provides insight into postoperative and long-term outcomes in TNBC patients who undergo post-mastectomy breast reconstruction. Lower BMI and younger age were predictors of mortality. We did not identify any differences in adverse outcome based on type of reconstruction. TNBC patients with localized disease undergoing breast reconstruction have 5-year overall survival rates comparable to patients with other types of breast cancer. Therefore, we advocate that reconstruction options should be offered routinely to patients with TNBC.
Footnotes
Conflict of interest and financial disclosure statement
There are no financial disclosures, commercial associations, or any other conditions posing a conflict of interest to report for any of the above authors.