
Abstract
BACKGROUND:
In breast cancer patients, there is an elevated risk of developing osteoporosis during treatment which should be addressed by optimizing 25(OH) levels.
OBJECTIVE:
The aim was to assess the prescription, information and physician-patient communication on vitamin D and bone density in Germany.
METHODS:
We developed a standardized questionnaire concerning bone density measurement, vitamin D (blood level testing, prescription), information and communication regarding vitamin D. The questionnaire was distributed at the annual meeting of all group leaders of the Women’s Cancer Support Association to all participants.
RESULTS:
Overall, 224 participants completed the questionnaire; 77.7% reported having had at least one bone density measurement test. The number was 84.4% in patients treated with aromatase inhibitor and 43.7% reported that their bone density was too low. In total, 51.3% patients reported at least one vitamin D blood test and 45.1% reported that vitamin D had been primarily addressed by a physician. As many as 74.1% of those reporting a test result had a deficiency; 91.6% of those with a low level got a prescription and 28.4% took vitamin D autonomously.
CONCLUSIONS:
The awareness on risk of osteoporosis, prevention, early diagnosis and treatment are insufficiently addressed in a patient group with high risk of osteoporosis. More attention should be paid to the phenomenon of vitamin D deficiency or insufficiency in routine care.
Keywords
Introduction
The research on vitamin D in cancer care is a rapidly evolving field. Yet, despite nearly 10,000 articles listed in Medline in the last 10 years (search combining the MeSH terms vitamin D and neoplasms) and more than 1,500 in the last five years, evidence is controversial with respect to its role besides in the prevention of osteoporosis. While the prescription of vitamin D to prevent and treat osteoporosis is part of national guidelines [1], the importance of vitamin D with respect to prevention of cancer, its prognosis and the influence on treatment efficacy are still under discussion.
Many patients with breast cancer are at risk of developing osteoporosis [2,3]. Reasons are diverse. While endocrine therapy with an aromatase inhibitor often leads to a prescription of vitamin D, the risk for other women is less clear. Risk factors are age, lower physical activity, menopause due to chemotherapy, sedentary profession and/or lifestyle, malnutrition with lack in calcium and/or proteins. Even the German national S3 Guideline on Breast Cancer as well as the actual recommendations of the Gynecological Oncology working group in the German Cancer Society only give a general recommendation without more detailed information on risk assessment, dose and controlling [4,5].
The preponderance of vitamin D deficiency in women with breast cancer has been assessed by Nogues and colleagues who reported 88% of their patients as having 25(OH)-D levels <30 ng/ml, 21% having a severe deficiency (<10 ng/ml), and 25% having osteoporosis [6]. Moreover, there was a significant association between 25(OH)-D level and bone mineral density. In the large Women’s Healthy Eating and Living (WHEL) study, nearly a third (31.6 %) of the women had a deficit in Vitamin D (<20 ng/mL), another third (32.2 %) had a very low level (20–30 ng/mL) and only a third (36.2 %) had a normal level (>30 ng/mL) [7]. A retrospective analysis of the MA21 study on adjuvant chemotherapy revealed a rate of 20% of vitamin D deficiency (<20 ng/ml) [8].
In 2013, a systematic review on calcium and/or vitamin D supplementation reported that no controlled trials exist comparing supplements versus no supplements on bone mineral density in pre- or postmenopausal patients with breast cancer [9]. The authors reported on 16 trials that showed that the vitamin D doses tested (200-1000 IU vitamin D) are not adequate to prevent osteoporosis. While postmenopausal women may lose about 1% of bone mineral density per year, patients with breast cancer lose 2–3 fold more [10]. Consequences of lower bone mineral density are pain and fractures, both being associated with loss of function and quality of life [11–14] and higher mortality [15,16].
Apart from this indirect mechanism on survival, several authors have addressed the influence of vitamin D on the prognosis of patients with breast cancer. However, results are heterogeneous. In an embedded matched pair study within the prospective WHEL study there was no association between prognosis and 25(OH)-D-level [17]. While there was no association with cancer specific mortality, patients with a normal vitamin D level were less likely to die (Hazard Ratio (HR) = 0.90; 95% Confidence Interval (CI) 0.50–1.61). Also, in the MA21 study [8], there was no association between vitamin D level and breast cancer specific survival or overall survival. In a prospective cohort study from Germany with 1295 postmenopausal survivors of breast cancer, there was an inverse association between 25(OH)-D level and mortality [18]. With a threshold of 55 nmol/l a hazard ratio of 1.55 for overall survival (95% CI 1.00–2.39) and 2.09 for disease free survival (95% CI 1.29–3.41) was reported. A systematic review including 25 studies reported an inverse association between 25(OH) D level and prognosis for colorectal cancer, prostate cancer and melanoma from prospective cohort studies, while for non-small-cell lung cancer there was no association. From two studies with patients with breast cancer one showed an inverse association and the other no effect [19]. Another systematic review with meta-analysis reported data from five studies. A normal level was inversely associated with overall mortality (HR 0.62; 95% CI 0.49–0.78) and tumor-specific mortality (HR 0.58; 95% CI 0.38–0.84) [20].
In this controversial debate, the communication of patients and physicians on vitamin D is not based on recommendations and patient information containing high level evidence. In a pilot study, we were able to show that about a half of the participants reported that the topic of vitamin D had been raised by a physician and 36% had brought up the topic themselves. While 68% reported having had bone density measurement, only 58% of those with low bone mineral density reported having had a test of the vitamin D level; 80% of the tested persons reported a low level [21].
The aim of our survey was to collect more detailed information on the patient-physician-communication and the dealing with vitamin D in the routine care of patients with breast cancer in Germany.
Patients and methods
Questionnaire
In cooperation with patient advocates from the Women’s Cancer Support Association [22] we set up a first draft of a questionnaire which was tested in a pilot study on 18 members of one regional group of the Association. We asked the participants to fill in the questionnaire and to give short feedback to every question as to whether it was easy to understand and fill in. With this feedback, we decided to remove one question on satisfaction with patient-physician communication and to add questions on doses of vitamin D supplements recommended by the physician or chosen by the patient in the case of taking vitamin D on their own.
The questionnaire comprises five sections: Demographic data Data concerning cancer and cancer treatment (type of cancer, time since first cancer diagnosis, former and current therapy) Data concerning bone density measurement Data concerning vitamin D (testing of blood level, patient knowing whether his/her level was normal of low, prescription, reimbursement) Data concerning information and communication regarding vitamin D
Most questions were closed questions offering a free line to give detailed data on for example date or doses. The questionnaire was anonymous.
Patients
The questionnaire was distributed at the annual meeting of the Women’s Cancer Support Association in August 2018. This meeting was attended by more than 500 group leaders (all current or former cancer patients) of the organization from all parts of Germany. Participation was voluntary.
Statistics
Data were managed by IBM SPSS Statistics 24 for data collection and analysis. To analyze associations between variables, chi-square tests were used and p-values smaller than 0.05 were considered significant.
Results
Demographic data
All in all, 224 patients’ representatives took part in our survey of whom 223 were female and one male (the organization has a section for male patients with breast cancer). Median age was 63.0 years and ranged from 35 years to 80 years. Demographic data are presented in Table 1.
Demographic data of the participants (n = 224)
Demographic data of the participants (n = 224)
1 = 38 Aromatase Inhibitor, 31 Tamoxifen, 1 Fulvestrant
With respect to bone density measurement, 174 (77.7%) reported having had at least one test while 41 (18.3%) reported not having been tested. From the 38 patients taking an aromatase inhibitor, 32 (84.2%) reported boned density measurement.
From the 174 patients who reported having been tested for bone density, 94 (54.0%) answered that the result was normal and 76 (43.7%) reported that their bone density was too low. Eighteen patients reported having had a second assessment of bone density (10.3%) but only four reported the result (three normal (1.7%) and one low (0.6%)). Only two patients with a low density at first measurement reported a control measurement (2.6%).
Women after menopause significantly more often reported having been tested (p = 0.023). This was also true for women with university diploma (p = 0.027). In contrast, neither endocrine treatment nor taking an aromatase inhibitor was associated with testing.
Vitamin D
Communication on vitamin D
Only 101 participants (45.1%) reported that the topic of vitamin D primarily had been raised by a physician. Most often named was the general practitioner (n = 15; 14.9% of those addressed by a physician), followed by the oncologists or gynecologist (n = 17; 16.8% both). Sixty-three patients (28.1%) reported that they brought up the topic. Of these, 27 (42.9%) addressed the general practitioner and 10 (15.9%) the gynecologist (Fig. 1). Overall, 141 participants answered the question on how they rated the quality of communication on vitamin D (62.9%). About two thirds of those participants (n = 77; 54.6%) rated communication as good or very good (Fig. 2). Rating of quality was not associated with age or education.
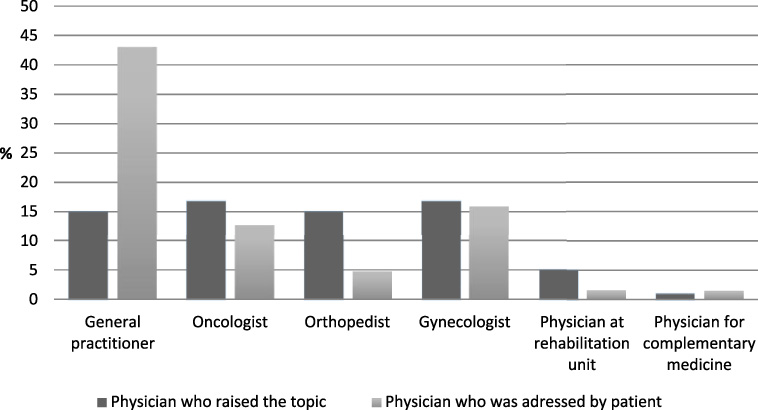
Person initiating communication about vitamin D (n = 224).
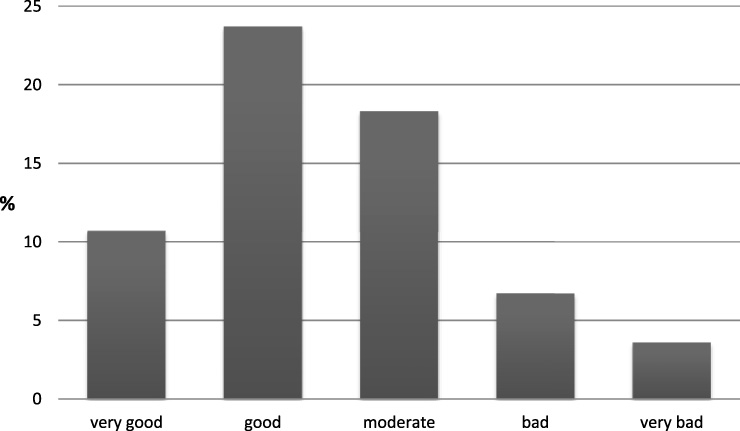
Rating of the quality of communication about vitamin D by the patients (N = 141).
Overall, 115 patients reported having had at least one blood test (51.3%). From those, 31 (27.0% of all tested) had paid for it themselves and 69 (60.0%) got a reimbursement from the statutory health service. The result of the test was reported by 112 patients. Seventeen (15.2% of those reporting a result) reported a normal level, and 83 (74.1% of those reporting a test result) had a deficiency of vitamin D. While age or endocrine treatment was not associated with assessment of vitamin D level, patients with university diploma more often reported reimbursement by health service (p = 0.04). There was no association between the result of the bone mineral density test and a test on vitamin D level.
Vitamin D supplements
All in all, 95 patients (42.4%) reported taking vitamin D by prescription. Seventy-six patients with a low level (91.6%) got a prescription while seven patients (8.4%) had not received one. One hundred and two participants (45.5%) reported taking vitamin D without a physician’s prescription.
The dosage chosen was reported by 102 patients (45.5%). From those, 7.8% took 400 I.E. per day, 3.9% 800 I.E., 14.7% 1000 I.E. and 45.1% 20.000 I.E. per week. Twenty-nine (28.4%) marked “other dosage”.
The most frequently named sources of information on vitamin D were self-help organizations (n = 32; 25.0%) followed by the Internet (n = 20; 15.6%) (Fig. 3).
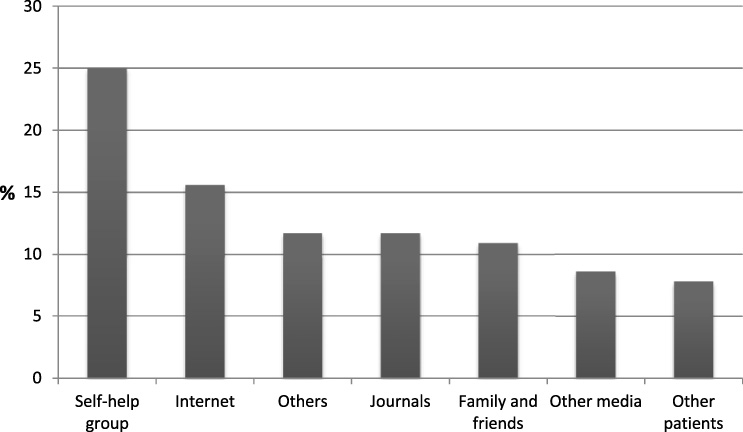
Sources of information regarding vitamin D used by the participants who took vitamin D on their own (n = 128).
About three quarters of the patients reported having had at least one bone density measurement. Yet, our data show that some patients at risk of osteoporosis due to aromatase inhibitors did not get an assessment despite recommendation in the national guideline on breast cancer [4]. Nearly half of the patients reported having a too low bone density. Control measurements as recommended in case of low density only were reported by a minority. Overall, risk assessment of osteoporosis and more to management of the risk do not seem to be satisfactory.
Considering vitamin D, only half of the patients had a blood test. More than three quarters reported having a low level. These data are even higher than those in the literature [6,17,21,23]. There may be several explanations for this discrepancy. First of all there might be differences between different countries (USA vs. Germany) or between collectives which may be due to exposure to sunlight, usage of supplements as well as other lifestyle factors. However, other studies also point to a higher prevalence of vitamin D deficiency. Peppone et al., for example, reported a rate of 66.5%, which is near to the data published by the Robert Koch Institute for Germany: 57% of all adult men and 58% of adult women have a low vitamin D level. For women between 65 and 79 years of age, 75% had a low level [24,25]. Accordingly, the actual German S3 guideline on Complementary Oncology strongly recommends to measure vitamin D levels and to supplement in case of deficit for all cancer patients [31]. With the according patient version of the guideline, all patients may get access to this information and the vitamin D topic should be part of routine cancer care.
Consequences with respect to a prescription of a supplement were taken in 92% of these patients. In contrast, 8%, in spite of a low level, did not get a prescription. Most often prescribed were 20.000 IU/week, yet nearly 30% only got a low dose of 1000 IU per day or less, which most probably is not sufficient to raise the level. One possible explanation of lack in prescription may be the discussion on the threshold between a low level and a vitamin D deficiency, which some authors put at 25(OH)-D levels <30 ng/ml, some at 25(OH)D levels <20 ng/ml [26–29]. Moreover, in Germany, the S3 guideline on osteoporosis proposes 1.000 I.E. per day [1]. Nearly half of the participants decided to take vitamin D on their own. Thus, the question arises whether this might be harmful and lead to overdose. As far as we know, no data have been published on this risk. However, most patients stick to 1000 IU/d and those without a prescription in Germany are not allowed to buy the 20.000 IU capsules, so most probably the intake will not result in higher levels [23–25,29]. As no data from prospective studies in cancer patients exist, choosing the appropriate dosage is difficult. Due to this, control of levels might be appropriate but is seldom done. Regarding communication on vitamin D, patients most often seem to be left alone by the physicians. Actively addressed were that less than a half and more than a quarter took the initiative and addressed the physician. All-in-all, two thirds rated communication as good or very good. However, this leaves a third being unsatisfied.
Considering patients who talked to a physician on vitamin D, the general practitioner was most often named closely followed by specialized physicians. This points to a deficit in the specialized care of patients with breast cancer as in these, the oncologist or gynecologist should have addressed the topic already while initiating or during treatment. As already shown in the pilot study, the most important information source of information on vitamin D is self-help groups [21].
As our data suggest, there may be social inequalities in osteoporosis prevention among breast cancer patients. Women with higher education were more likely to get a bone mineral density testing. Moreover, patients with university diploma more often reported reimbursement by health service, which might be due to academics being more likely in a private insurance than in a statutory health service. However, for blood testing and prescriptions, there was no association. Physicians should watch out for such inequalities. Moreover, self-help groups may be good partners for patients to gather information and to be actively informed, as many self-help groups have regular meetings and often choose medical topics or invite referents. In fact, self-help is currently the most important source of information on the topic.
Concerning payment for vitamin D tests, which was an important topic for the survey for the self-help organization, a third had paid themselves and slightly fewer had paid for the control measurement.
Considering the detrimental effects of osteoporosis on survival time, quality of life and the ability to care for oneself, more attention should be paid to patients at risk of bone mineral density loss. Simple and cheap options exist to prevent osteoporosis. Besides drugs and supplements, patients at risk should be informed on healthy lifestyle (physical activity and nutrition) and, in case of impairments, training and fall prophylaxis should be considered. In this, the general practitioner already is an important part but might even gain more importance. In fact, with respect to other risk factors and comorbidities increasing risk of osteoporosis, the general practitioner may help to address lifestyle and prescribe, for example, rehabilitation sports.
Strengths and limitations
As far as we know, this is the first study that asked self-help representatives about vitamin D throughout Germany. Since the 224 persons interviewed are group leaders of self-help groups, who can be considered as experienced persons in the German healthcare system due to their own experiences and those brought to them due to their work, the collected data allow a realistic estimation of the current daily care. The patient perspective is another important strength of this work. In this way, further need for care can be identified. Further strength of this work is the additional items on communication within the used questionnaire. In oncological care, patient-centered communication with the goal of shared decision-making is a concern of the German National Cancer Plan [30] and similar initiatives in other Western countries.
On the other hand, there are several limitations to our study. First of all, the questionnaire we used was not validated. Moreover, we only have reported data from the perspective of the patients and have neither an access to the data of vitamin D levels nor of bone density measurements. We also did not ask patients on the actual vitamin D level but only whether this was normal, low or unknown. Another limitation is that we did not discriminate between insufficiency and deficiency of vitamin D, which most probably would have been too complex for the participants. Demographic data which would also contribute to assess the risk of osteoporosis as body mass index, smoking or comorbidities were not included in our questionnaire. With respect to the results concerning patient-physician communication, the relevant information is what is remembered and retold by the patient and not what had been intended by the physician. Last but not least the participants of our survey were highly selected. Group leaders of the Women’s Cancer Support Association most probably are better educated and more interested in actively taking part. One might speculate whether patients with less opportunities of information may even have worse supply with respect to prophylaxis and treatment of osteoporosis.
Conclusion
To conclude, more attention should be paid to the phenomenon of vitamin D deficiency or insufficiency. The awareness on risk of osteoporosis and prevention, early diagnosis and treatment are insufficiently addressed in routine care in a patient group with high risk of osteoporosis.
Footnotes
Acknowledgements
We thank the members of the “Frauenselbsthilfe nach Krebs” (Women’s Cancer Support Association) for their engagement in this project.
Funding
There was no financial funding for this study.
Disclosure of potential conflicts of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent was given by the individual participants by filling in the questionnaire.