
Abstract
BACKGROUND:
Mondor disease is superficial thrombophlebitis of the thoracoabdominal wall, mid-upper arm, and penis. Although it is usually a benign disease requiring no specific treatment, little is known about this disease owing to its rarity.
OBJECTIVE:
The aim of this retrospective observational study was to investigate the epidemiology and prognosis of Mondor disease.
METHODS:
We conducted a single-center observational study of patients with Mondor disease. Patients who received a diagnosis of Mondor disease between 2015 and 2020 were analyzed. The patients’ medical records were manually reviewed to obtain the following variables: date of diagnosis, patient’s age, sex, department of diagnosing physicians, underlying diseases, medications, surgery, and time until resolution of the lesion. We also reviewed the 1-year mortality, 1-year occurrence of malignancy, and recurrence of Mondor disease.
RESULTS:
20 patients were included in the study. The age of the patients ranged from 7 to 83 years, with a median of 47.5 years. Most of the patients presented with thoracoabdominal wall lesions. The underlying conditions included skin diseases, surgical procedures, breast cancer, smoking, and collagenous diseases, although more than half of the patients did not have plausible predisposing factors. About three-quarters of the patients saw a spontaneous resolution of the lesions within 4 weeks without medical or surgical treatments.
CONCLUSIONS:
Considering the good prognosis of this disease, it is essential to avoid unnecessary invasive tests or treatment once the diagnosis is confirmed.
Introduction
Mondor disease is superficial thrombophlebitis that presents a palpable cord-like induration [1]. It is classified into 3 groups according to the lesion site: anterolateral thoracoabdominal wall, mid-upper arm, and dorsal and dorsolateral aspects of the penis (Fig. 1). Although some reports have suggested its relation to the hypercoagulative state, vasculitis and other vascular diseases, carcinoma, and sexually transmitted infections, it is usually a benign disease that resolves spontaneously within 4 to 8 weeks [2].
However, because of its rarity, little is known to date about Mondor disease, leading to the underdiagnosis of this disease and patients’ doctor shopping. Fewer than 400 cases of this disease have been reported in the medical literature [3]. Therefore, the risk factors, optimal treatment, and long-term prognosis have not been well established. More confusingly, although most authors have explained that this disease is easily recognizable by the medical history and physical examination, some authors have insisted on additional testing, including biopsy of the lesion, to confirm the diagnosis [4].
Here we describe the underlying disease, treatment, and prognosis of patients with Mondor disease at a tertiary academic hospital in Ibaraki, Japan.
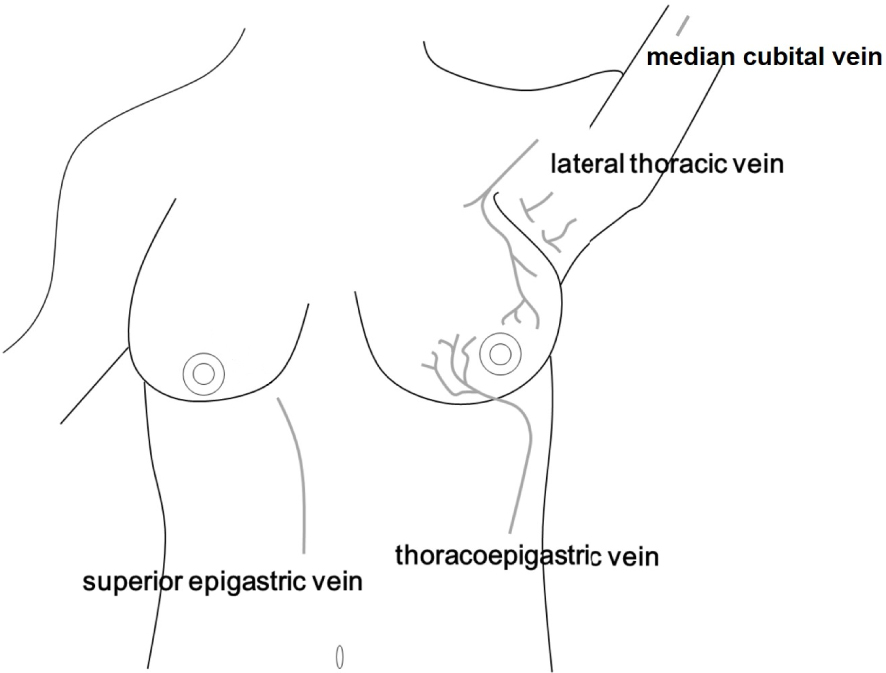
Typical location of Mondor disease.
We conducted a single-center observational study of patients with Mondor disease. Institutional review board approval was obtained from the University of Tsukuba Hospital (R03–049). Because no care interventions were required, the requirement for signed patient consent was waived.
Patients registered as having “Mondor disease,” “superficial vasculitis”, or “thrombophlebitis” from January 2015 to March 2021 were included in the study. Patients who did not have thrombophlebitis consistent with Mondor disease were excluded. The University of Tsukuba Hospital is a large, single-site, tertiary teaching hospital in eastern Japan with about 800 beds, 700 inpatient admissions, and 1800 visits per day. The hospital offers several specialist services, including general medicine, dermatology, urology, and breast surgery.
Mondor disease was defined as superficial thrombophlebitis occurring in the anterolateral thoracoabdominal wall, the dorsal or dorsolateral aspects of the penis, or the mid-upper arm. Thrombophlebitis in other sites was not regarded as Mondor disease in this study. The patients’ medical records were manually reviewed to obtain the following variables: date of diagnosis, patient’s age, sex, department of diagnosing physicians, underlying diseases (cardiovascular disease, coagulation abnormality, malignancy, trauma, dermatosis, and endocrine disease), medications, surgery, and time until resolution of the lesion. We also reviewed the 1-year mortality, 1-year occurrence of malignancy, and recurrence of Mondor disease.
Results
A total of 712 patients were registered as having “Mondor disease”, “superficial vasculitis”, or “thrombophlebitis” during the study period. After excluding 692 patients who presented with thrombophlebitis and vasculitis inconsistent with Mondor disease (635 due to deep venous thrombosis, 51 due to infusion-related phlebitis with peripheral intravenous catheters (i.e. nicardipine-related phlebitis), 4 due to varicose veins of the legs, 1 due to stasis dermatitis, and 1 due to Lemierre syndrome), 20 patients were included in the study.
The 20 patients were aged between 7 and 83 years, with a median of 47.5 years, and 16 (80.0%) were women (Fig. 2). Seventeen patients (85.0%) presented anterolateral thoracoabdominal wall lesions, and 3 patients (15.0%), mid-upper arm lesions (Table 1). Of note, we identified no patients with penile Mondor disease. In terms of laterality, 9 patients (45.0%) presented right-sided lesions, and 11 patients (55.0%), left-sided lesions. The diagnosis was made in more than half of the patients (13 of 20) by dermatologists, and in the remaining patients, by primary care physicians, breast surgeons, and plastic surgeons. Notably, all cases of Mondor disease of mid-upper arm were diagnosed by dermatologists.
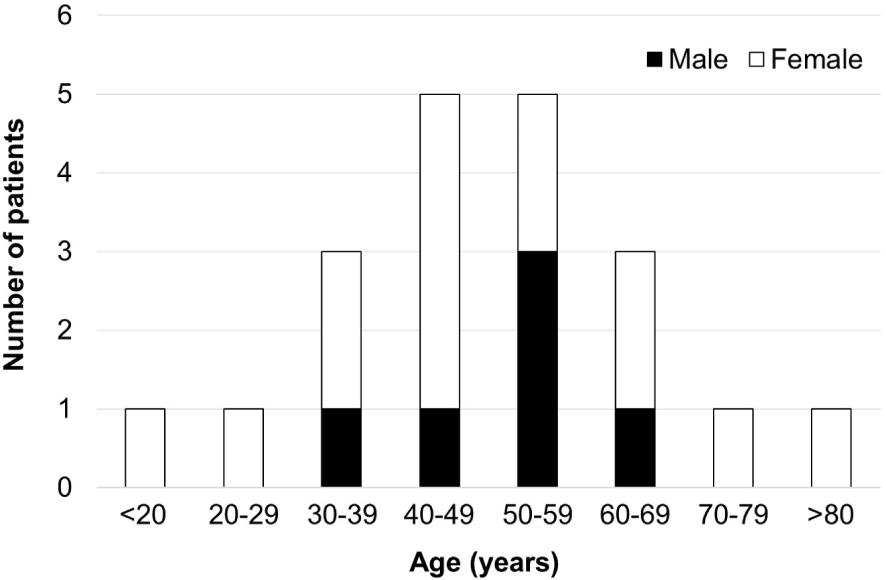
Age distribution of patients with Mondor disease.
Characteristics of 20 patients with Mondor disease
Seven patients (35.0%) had more than 1 plausible predisposing factor, ie, skin diseases, surgical procedures, breast cancer, smoking, and collagenous diseases (Table 2). In most of the cases, Mondor disease was diagnosed on the basis of the medical history and physical examination; in 1 case, it was diagnosed on the basis of the surgical biopsy. Although 80% of the patients (16 of 20) did not receive medications, 70.0% of the patients (14 of 20) saw a resolution within 4 weeks. No patients died or developed malignancy within 1 year of diagnosis. However, 1 patient who underwent a surgical biopsy for a primary Mondor disease lesion experienced a recurrence of Mondor disease 4 years after the procedure.
Summary of 20 cases of Mondor disease
In our study, Mondor disease developed mainly among patients aged 30 to 50 years. Besides, it occurred more frequently in women than in men, particularly when it affected the lateral thoracic vein. According to a literature review, thoracoabdominal Mondor disease generally occurs unilaterally in middle-aged women, with a female to male ratio of 9:14 [5]. Our results are consistent with those of that previous report; however, our results also suggest that Mondor disease can develop among the wider population. Primary care physicians, as well as dermatologists and breast surgeons, can encounter Mondor disease and should recognize this disease to avoid underdiagnosis and unnecessary tests and treatments. Notably, there were no cases of penile Mondor disease in our study, suggesting the underdiagnosis of this disease among urologists. Because of similarity in the presentation, penile Mondor disease can be misdiagnosed as other conditions such as Peyronie disease, hypercoagulability, blood stasis, genitourinary infection, and malignancy [6,7]. Penile Mondor disease may be related to neoplasms, excessive sexual activity, trauma, or abstinence; however, we could not investigate the risk factors for penile Mondor disease due to the lack of cases.
In terms of the laterality of Mondor disease, 1 patient with left-sided breast cancer and one with surgical resection for a right-sided epidermoid cyst developed Mondor disease in the left upper arm and right axilla, respectively. This result suggests the effect of a mass and of trauma on the development of Mondor disease. This notion is consistent with that in a review article by Amano and Shimizu, in which they describe its association with surgical operation, radiation, hormone therapy, and breast cancer [2]. Notably, Mondor disease has been known as a complication after breast surgery, and Mondor disease after axillary manipulations is especially called axillary web syndrome. However, the incidence varies according to studies. For example, the incidence was as low as 2.4%, according to a retrospective study from Taiwan [8]. In contrast, 8 patients out of 63 Mondor disease patients (12.7%) had breast cancer in a retrospective study from Italy [9]. Ultrasound-guided core needle biopsy of the breast may also lead to Mondor disease [5], and thus interventional breast radiologists should be aware of this disease. Furthermore, direct trauma from tight clothing and repeated muscle training have been reported as causes of Mondor disease [10]. Nevertheless, among the 18 patients without any localized factor in our study, Mondor disease occurred almost equally on both the right and the left side. Considering that most people are right-handed [11], there seems to be little association between the laterality of Mondor disease and handedness. However, it should be noted that 4 out of 9 cases (44.4%) of right-sided lesions took more than 4 weeks, which suggests the association between the laterality and delayed cure. Unfortunately, we did not find any information on the handedness of the patients included in our study, and further studies are needed to confirm this relationship.
About three-quarters of the patients in our study did not receive any medical treatments, and many patients saw a resolution of the lesion within 4 weeks. However, the symptoms lasted more than 8 weeks in 4 patients. Most of the patients with Mondor disease did not develop life-threatening complications, and explaining this nature to patients seems essential to prevent doctor shopping. Although one of our patients had preexisting breast cancer, no patients developed breast cancer within 1 year of Mondor disease diagnosis. Owing to the scarcity of data, it is still too early to conclude that breast cancer has a direct relation with Mondor disease.
The strength of our study is that it included relatively many cases of Mondor disease when most of the literatures on this disease were case reports. However, several limitations of this study should be acknowledged. First, it was a single-center observational study in a tertiary care academic center in Japan, where physicians offer several specialist services, including general medicine, dermatology, urology, and breast surgery. Therefore, the results may not be generalizable to other institutions with different patient, physician, and health care characteristics. For example, it is undeniable that we overestimated the proportion of Mondor disease patients with underlying diseases because patients without any other comorbidities may visit clinics rather than tertiary academic hospitals. To increase external validity, we are planning to perform a multicenter study with an increased sample size in the near future. Second, although we attempted to ascertain the diagnosis and associated factors through a meticulous chart review, the results could have been subject to incomplete documentation owing to the retrospective nature of this study. Third, blood tests and other diagnostic tests were not performed in most cases. Although most of our patients did not develop complications after the diagnosis of Mondor disease, it is undeniable that our patients may have had some overlooked conditions.
In conclusion, we found that Mondor disease can develop among a broadly aged population, and specific treatments were not necessary in most cases. The diagnosis of Mondor disease is rather straightforward and based on physical findings; however, some cases occurred “secondary” to another underlying disease in our study. Therefore, it is critical to precisely identify Mondor disease, evaluate any possible underlying condition, and avoid unnecessary invasive tests or treatment.
Footnotes
Acknowledgements
We are grateful to Dr. Flaminia Miyamasu, Medical English Communications Center, University of Tsukuba, for the grammatical revision of this manuscript.
Ethics approval
Local hospital ethics approval was obtained for this study (R03–049). Data are available upon reasonable request from the corresponding author via email.
Conflict of interest
None of the authors have any conflicts of interest to disclose.
Funding sources
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.