
Abstract
Breast pain is a common concern among women in primary care clinics. A rare cause of breast pain is Mondor’s disease (MD), which can present as an acute, painful, erythematous, cord-like induration on the breast or anterior chest wall. The disorder is caused by sclerosing superficial thrombophlebitis of the anterolateral thoracoabdominal wall veins. There does not appear to be a racial or ethnic propensity for this condition; however, it is important to understand that it may be more difficult to see in darker skin types (Fitzpatrick skin types IV-VI) and requires close attention on physical exam. The cause of MD is poorly understood but may be related to direct trauma, strenuous exercise, or hormone changes. We review a case of a 54-year-old woman who presented with an anterior chest wall palpable cord, better visualized with adequate lighting and skin traction, ultimately diagnosed as MD based on clinical findings and imaging studies. Mondor’s disease often resolves spontaneously with supportive care, as in this patient’s case; however, clinicians should be aware of this rare cause of breast pain and its association with hypercoagulable state, vasculitis, and breast cancer.
Keywords
Introduction
Nearly 70% of women experience breast pain in their lifetime, 1 and it is estimated that around 16% of women 40-69 years of age will have a breast concern over a 10-year period prompting medical evaluation. 2 Common concerns in addition to breast pain include mass or nipple discharge. 2 For a palpable breast mass, a clinical examination is recommended in addition to diagnostic mammography for women older than 30 years of age and ultrasonography for women younger than 30 years of age. 2 The differential diagnosis for a breast mass includes fibroadenoma, fat necrosis, fibrocystic changes, phyllodes tumor, and malignancy. One rare cause of breast pain with a palpable area is Mondor’s disease (MD), a disorder characterized by thrombosis of superficial veins within the subcutaneous tissue of the breast. 3 It can be diagnosed clinically with history and physical examination. Mondor’s disease presents as an acute, painful, erythematous, palpable cord-like induration arising in the chest wall area or breast. 4 It can present in men or women; however, women are 3 times more likely to be affected.4,5 There does not appear to be a racial or ethnic propensity for this condition; 5 however, many MD images available include patients with Fitzpatrick skin types I-III (where the cord-like structure and erythema may be easier to visualize) and less images of Fitzpatrick skin types IV-VI.6,7 Overall, it is estimated that 50% to 60% of MD cases are idiopathic in nature. 4 Other cases may have risk factors including trauma, breast surgery (eg, augmentation, reduction mammoplasty, and breast biopsy), excessive physical exercise, hormone changes (egg, use of oral contraceptives and pregnancy), and infections. 3 In this case, we present a 54-year-old woman with Fitzpatrick skin type V with a palpable cord-like induration that was not erythematous and was diagnosed with MD.
Case Presentation
A 54-year-old woman presented to the outpatient family medicine clinic for evaluation of right breast pain for 1 week. Her past medical history was significant for hypertension treated with amlodipine, hyperlipidemia treated with atorvastatin, prediabetes treated with metformin, and menorrhagia treated with oral contraceptives (levonorgestrel-ethinyl estradiol). The patient reported feeling a “swollen vein” near her right breast. There was no antecedent trauma or history of breast surgery and no history of malignancy or clotting disorder. She denied any other symptoms including fever or chills. She was up to date on age-appropriate cancer screenings and a nonsmoker. Vital signs were unremarkable. On initial visual inspection, the area of concern was difficult to visualize due to skin pigmentation. During physical examination, additional lighting and traction was applied to the skin and revealed a firm, tender, nonerythematous palpable cord (Figure 1) originating at the lower portion of the right breast at the 6 o’clock position and extending approximately 15 cm inferiorly toward the abdomen. There was an area of skin retraction at the superior aspect of the palpable cord that appeared asymmetric to the contralateral breast in the resting position.

Tender palpable cord.
A diagnostic right breast mammogram with tomosynthesis and focused right breast ultrasound was ordered for evaluation. Right breast diagnostic mammogram with spot magnifications and tomosynthesis at the region of concern did not show focal underlying abnormality (Figure 2). Ultrasound demonstrated a superficial tubular structure with hypoechoic material and no visible internal flow, compatible with a thrombosed superficial vein (MD) (Figure 3).
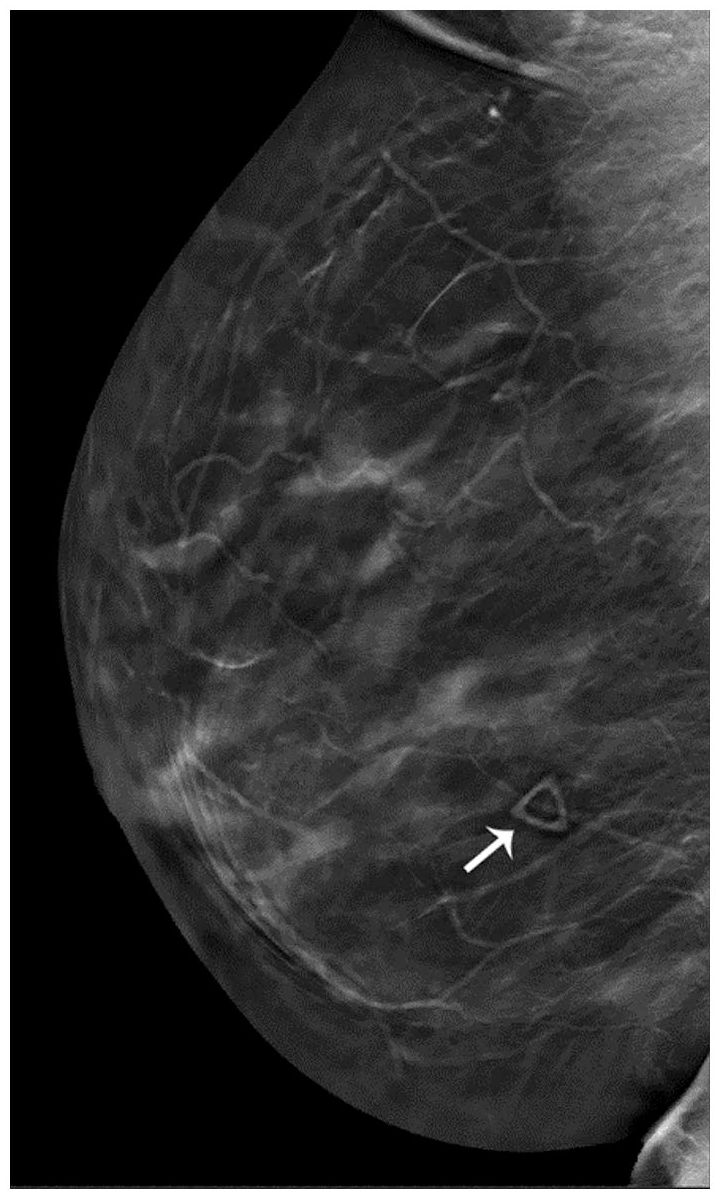
Diagnostic mammogram with tomosynthesis of the right breast.

Color Doppler ultrasound of the right breast.
The patient was advised to use supportive measures, including nonsteroidal anti-inflammatory drugs and warm compresses. A second ultrasound 3 months later showed resolution of the thrombosed superficial vein (Figure 4), and clinically, the patient’s pain resolved. A suspected risk factor for the patient was her oral contraceptive prescribed for menorrhagia. She had no signs of systemic disease or malignancy. The patient was advised to consider discontinuing the oral contraceptive or consider an alternative, such as a progesterone-based hormone therapy.
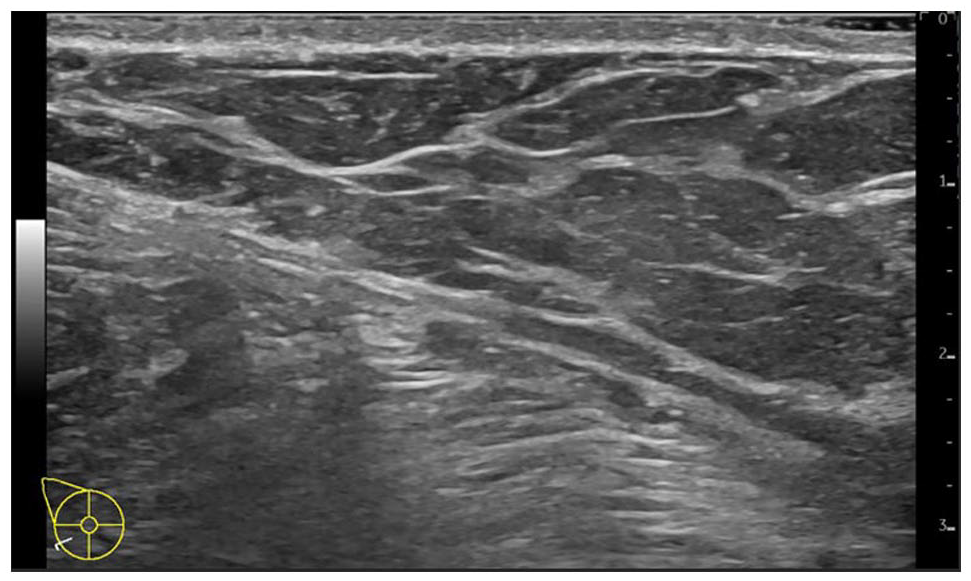
Grayscale ultrasound of the right breast.
Discussion
Mondor’s disease of the breast is a rare clinical condition that most commonly affects women aged 30 to 50 years with less than 400 cases reported and an incidence ranging from 0.08% to 0.94%.8-11 Differences in incidence among geographic areas suggest there could be a variety of epidemiologic factors influencing incidence of MD. The pathophysiology of MD is not well understood, but it is theorized that inciting factors (ie, trauma, surgery, breast cancer, smoking, hormone replacement therapy, or oral contraceptive use) can cause sclerosing thrombophlebitis of superficial veins.10,12 This process provokes an inflammatory response leading to development of a fibrosed, cord-like vein that is palpable and can cause pain, erythema, and swelling. 5 The superior epigastric vein is the most commonly affected vessel and is seen in the inferior outer quadrant of the breast. 5 Diagnosis may be made on physical examination, but imaging is often obtained for further evaluation. Radiologic findings include a superficial vessel on ultrasonography with or without an intraluminal thrombus and corresponding tubular density on mammography. 13 It is important to document cases and publish images in a variety of skin types because MD may present differently in patients of different racial or ethnic backgrounds. In general, there is an underrepresentation of darker skin types in textbooks, educational curricula, and literature, especially in the field of dermatology.6,7
When the diagnosis of MD is made, it is important to determine if the cause is primary (idiopathic) or secondary (due to an underlying disease or process). 12 Clinicians should assess for other symptoms or family history that may indicate an underlying condition associated with MD, such as hypercoagulable conditions (eg, protein S deficiency, factor V Leiden, protein S deficiency), vasculitis or vascular disease (eg, giant cell arteritis, polyarteritis nodosa, Burger disease, Behçet syndrome), or malignancy. 14 It is important to ensure that cancer screenings are up to date, particularly mammograms in women, as 12.7% of cases have been linked to breast cancer. 3 In addition, individuals meeting criteria for lung cancer screening should have updated low-dose computed tomography, given MD’s known association with smoking. A thorough medication review should also be conducted as resolution of recurrent MD has been report after discontinuation of oral combined hormonal contraception. 14 More recently, cases have been documented in association with COVID-19 infection, likely secondary to hypercoagulability and systemic inflammation. 3 In general, MD is self-limiting and will resolve within 4 to 8 weeks with no treatment. 4 First-line treatment options include warm compresses, nonsteroidal anti-inflammatory drugs, and abstinence from irritating clothing or activities. 4
Conclusions
Mondor’s disease of the breast is a rare, self-limiting condition that can cause considerable pain in women. It can be diagnosed with history and physical exam alone but may require close inspection with adequate lighting, palpation, and skin retraction, particularly with patients with darker skin pigmentation. There are associations with breast cancer, vasculitis, and hypercoagulable conditions, which highlight the importance of awareness among clinicians. A thorough history, including medication reconciliation, family history, and social history are critical for identifying modifiable risk factors or possible underlying conditions.
Footnotes
Acknowledgements
The authors acknowledge The Scientific Publications staff at Mayo Clinic provided copyediting, proofreading, administrative, and clerical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.