
Abstract
Mondor’s disease can be a challenging diagnosis. The case we present is of a 29 year-old Brazilian woman, under combined hormonal contraception, who consulted for a painful lump on her right breast. She presented a complete resolution after a local treatment of heparinoid cream and a non-steroidal anti-inflammatory oral treatment, but relapsed 18 months later. Oral combined hormonal contraception was the only “risk factor” found, in this case, and the modification of the latter helped resolve the relapse clinical symptoms.
Introduction
Mondor syndrome is a thrombosis of the superficial veins of the anterolateral thoraco-abdominal wall [1]. The aetiology remains unclear and fewer than 400 cases have been reported in the medical literature [2]. The first clinical description of this syndrome was made in 1869 by Fagge, who assimilated it to a scleroderma sign [3]. It was not until 1939 that Henri Mondor, a French surgeon, described it as a separate entity [4].
The estimated incidence is of 0.5% to 0.8% [5], and women from 30 to 60 years old, are more likely affected (sex ratio 3:1) [6]. The risk factors most commonly described are trauma, iatrogenic cause (postoperative or post-biopsy), infection and/or excessive physical activity [7].
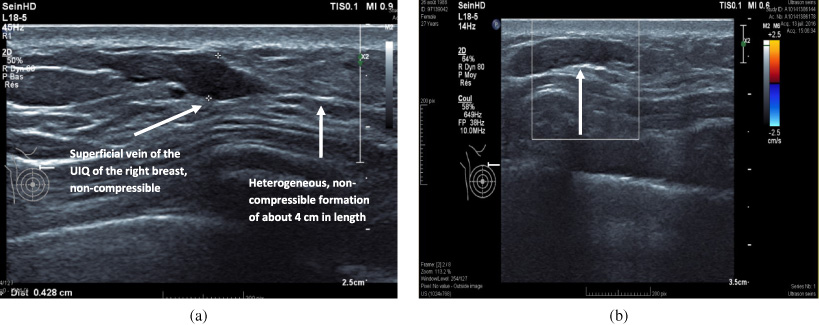
(a) Ultrasound showing a superficial vein, of the UIQ of the right breast, with a heterogeneous, non-compressible formation of about 4 cm in length, in favour of a superficial venous thrombosis. (b) Ultrasound showing a tubular, hypoechoic, non-compressible structure with no flow within in on colour Doppler (arrow), consistent with a superficial vein thrombosis.
Clinically, there is a painful subcutaneous millimetric to centimetric cord that may be bluish and is usually located in the breast or axillary region, with a topography generally in the superficial veins of the anterolateral chest wall (lateral thoracic vein, thoracoepigastric vein, superior epigastric vein) [8].
Although clinical examination is sufficient to make the diagnosis of Mondor’s disease, an ultrasound with venous Doppler, to complete the assessment, is recommended [9]. Histological examination is not necessary but should be performed if an oncologic origin is suspected and/or in case of an unfavourable evolution after 2 to 8 weeks of symptomatic treatment. Management consists mainly of simple analgesia (local and/or oral) [10,11].
A 29-year-old Brazilian woman, in Switzerland for more than 10 years, presented herself at the Breast Centre of the Geneva University Hospital after palpating a painful lump located in the upper-internal quadrant (UIQ) of the right breast. She had no other complaints.
The patient was in good health, non-smoker, and her medical history only revealed a caesarean section 7 years ago. The post-partum period was normal and she breastfed for one year and a half. The patient was under oral combined oestro-progestative contraception since she terminated her breastfeeding. She had no personal or family history of cancer and/or thromboembolic diseases (her blood count and coagulation tests were always normal).
The clinical examination revealed a 2 cm tender lump, in the UIQ, 6 cm from the areola, without any axillary lymphadenopathy, in a patient with a BMI of 24 kg/m2. There was no cutaneous involvement.
The ultrasound showed a tubular hypoechoic, non-compressible structure with multiple areas of narrowing with, about 4 cm in length of the upper-internal quadrant of the right breast. No flow was present on colour Doppler within it (Fig. 1). These ultrasound findings were compatible with a superficial vein thrombosis, also known as Mondor’s disease.
The patient was treated with local heparinoid cream and a non-steroidal anti-inflammatory oral treatment. She had regular clinical and breast-ultrasound monitoring for 9 months with a complete resolution of the Mondor’s disease.
During the course of her follow-up, the patient stopped taking her oral combined contraception and reinitiated it after the syndrome resolution.
Two months after resuming her oral combined contraception, the patient presented herself again with pain in the UIQ of the right breast. The clinical examination showed a 5 cm chord located in the UIQ of the right breast, with no other inflammatory signs. The ultrasound and the Doppler assessment confirmed the recurrence of a Mondor’s disease.
She received a local heparinoid cream treatment associated to a non-steroidal anti-inflammatory oral treatment and her birth control pill was changed from an oestro-progestative pill to a progestative pill. The patient presented a complete resolution after one-month. She was followed for 6 months after and did not relapse under a progestative-only contraceptive.
Discussion
The case presented is that of a recurrent Mondor’s disease under oral oestro-progestative contraception. In an article published by Mayor et al., the risk of recurrence of Mondor’s disease is estimated at 5% [12]. The prognosis and risk of recurrence are very poorly described in the medical literature and more investigations are needed to understand this rare breast disease [13].
The only apparent risk factor, in this case, seems to be the combined birth control. This is corroborated by the fact that a positive outcome happened when she stopped her hormonal therapy and recurred after resuming the same hormonal therapy. In addition, a rapid positive outcome occurred when the hormonal therapy was modified from an oestro-progestative pill to a progestative-only pill.
A similar case-report of a 35 year old patient presenting a Mondor’s disease with only an oral combined contraceptive, as risk factor, was described by Kadioglu and al. in 2013. As in our case, she healed in four weeks after stopping her birth control pill and did not recur [14].
A recent review of the literature, including four of the largest series published on Mondor’s disease, found that out of 124 cases, 11 (8.7%) were young patients taking a hormonal therapy [15]. Only one study makes a direct link between hormone therapy and Mondor’s disease [16].
In terms of radiographic findings, mammograms may reveal a superficially located tubular structure corresponding to the thrombosed vein. As for ultrasound findings, they include a dilated tubular anechoic or isoechoic structure with areas of narrowing, giving a beaded appearance, filled with low-level internal echoes, representing the clot. On color or spectral Doppler studies, no flow is present in the structure. The surrounding soft tissues may show a hyperechoic appearance due to inflammatory response [17,18].
Although the majority of cases in the literature have a iatrogenic cause (approximately 49.2% in the Laroche and al. study), breast cancer remains a rare cause which should be excluded, especially in cases with a negative outcome under symptomatic treatment [19]. If in doubt, a biopsy should be done, especially if there are risk factors for breast cancer in the medical history or clinical signs suspecting an oncologic origin [20].
In conclusion, we present a case of a Mondor’s disease with an oral oestro-progestative pill as only risk factor. In this case, the therapy and symptoms’ timelines are in favour of our hypothesis that combined hormonal contraception can be a risk factor for Mondor’s breast disease. This has been corroborated in only one other case report until now [14]. Even if it is described as a rare aetiology for this disease, with a few scarce case-reports described in the medical literature, further medical research is needed to verify our hypothesis.