
Abstract
INTRODUCTION:
Primary rhabdomyosarcoma (RMS) of breast is an uncommon entity and axillary lymph node (ALN) involvement is exceedingly rare.
METHODS:
Herein, we are reporting a case of RMS of breast with ALN metastasis in an adolescent girl. We searched Pubmed and Cochrane databases with keywords rhabdomyosarcoma and breast. All studies published in English language literature were included. Articles describing metastatic involvement of breast with RMS were excluded.
RESULT:
The initial search yielded a total of 8468 studies, out of which 03 were found to be duplicate. 8420 studies were excluded based on title and abstract as they did not fulfill inclusion criteria. Full text of the remaining 48 studies was screened. After full text screening, 26 case reports describing primary breast RMS were included. Overall 21% patients had axillary lymph node metastasis.
CONCLUSION:
Axillary staging should be considered in every patient undergoing surgery for breast RMS. However, it’s impact on recurrence and survival could not be determined based on current review.
Introduction
Rhabdomyosarcoma (RMS) is a common soft tissue neoplasm in paediatric and adolescent age groups [1]. However, primary RMS of breast is a rare occurrence accounting for less than 1% of all breast malignancies [2]. As lymph node metastasis from soft tissue sarcomas is uncommon, management of axilla is also not well defined for primary RMS of breast. Because of it’s rarity, management guidelines are lacking which worsens up the prognosis further. Herein we are reporting a case of primary RMS of breast in an adolescent girl with axillary lymph node (ALN) metastasis and review of literature with regards to incidence and management of axilla.
Case description
A 14 year old post menarche girl presented with breast lump involving whole of right breast of five months duration which was rapidly progressive. The right anterior axillary lymph node was also palpable. There were few dilated veins over chest wall (Fig. 1A).
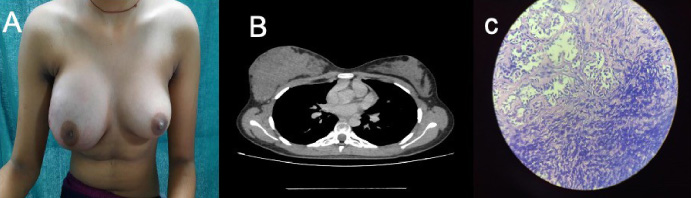
(A) Clinical picture of patient showing right breast mass involving whole breast; few dilated veins can also be seen; (B) computed tomography of thorax showing irregular hypodense lesion in right breast without any invasion of underlying muscle; (C) Histopatholgy of the resected specimen showing invasion of small round blue tumour cells into normal breast stroma, note the classical arrangement of tumour cells in tigroid pattern.
Ultrasonography revealed a 5.4 * 3.5 cm heterogeneous hypoechoic mass involving whole of right breast with interval vascularity accompanied by 12 * 14 mm axillary lymph node. A core needle biopsy was done which was suggestive of RMS. Computed Tomography (CT) chest was done to find the extension of the disease which showed isodence lesion involving right breast parenchyma and maintained fat planes with the underlying muscles (Fig. 1B). Computed tomography of chest and ultrasonography of abdomen did not reveal any lung or abdominal metastasis. We do not have bone scan facility at our centre and hence skeletal metastasis was evaluated by skeletal survey using X ray and it was negative. Since lump was occupying whole breast and frozen section biopsy is not available at our institute, patient underwent right sided modified radical mastectomy along with axillary lymph node dissection (ALND). The final histology showed an undifferentiated, high grade tumor of the small round blue morphology cells arranged in the classical tigroid pattern invading normal breast tissue suggestive of RMS (Fig. 1C). 10 out of 15 lymph nodes sampled showed metastatic deposits. Immunohistochemistry was positive for myogenin and desmin. Patient was planned for adjuvant chemotherapy and radiotherapy. However, she did not turn up for the same. She came for follow-up after six months from initial surgery and is free from the disease. She has been planned for chemotherapy and radiotherapy again.
Breast involvement with RMS is very rare, both as primary or metastatic site [3]. According to reports from Intergroup Rhabdomyosarcoma Study Group (IRS) of the United States, only 0.2% of RMS patients diagnosed were of breast origin. On the other hand, when confined to age between 10 and 21 years of age, 1.6% had breast origin RMS [2].
Due to rarity of this tumor, standard of care is not well defined. Earlier reports suggested mastectomy with excision of both underlying pectoral muscles should be performed in all cases [4]. However, recent understanding of management of soft tissue sarcomas and it’s extrapolation to breast RMS has led to less aggressive approaches such as wide local excision with negative margins. We could not perform breast conserving surgery in our patient as whole of the breast was involved. We plan to do reconstruction after completion of chemotherapy and radiotherapy.
Role of axillary lymph node (ALN) staging is also not well defined as lymph node metastasis is rare in soft tissue sarcomas [4]. We reviewed English language literature to answer this question (search strategy and brief summary available in Supplementary Document S1). We could retrieve 26 articles describing 40 cases of primary RMS of breast (Table 1). Nineteen patients (including our patient) underwent axillary staging (ALND- 16, Sentinel lymph node biopsy (SLNB)-03) out of which four had axillary lymph node metastasis. Axillary staging was performed on eight patients with clinically negative axilla and one had ALN metastasis on final histology. Thus rate of ALN metastasis is approximately 21% overall and 12.5% in clinically negative axilla. Due to heterogeneity of reported cases, outcome of axillary staging on local recurrence, overall survival or event free survival could not be analysed.
List of published case reports on primary RMS of breast and incidence of axillary lymph node metastasis (References for these articles are included in Supplementary Document S1)
List of published case reports on primary RMS of breast and incidence of axillary lymph node metastasis (References for these articles are included in Supplementary Document S1)
**References for these case reports are in Supplementary Document S1; *Data not available.
Surgery remains the only curative option as adjuvant therapies are not very affective [5]. Radiotherapy can be considered in patients with inadequate surgical margins or axillary lymph node involvement. Based on clinical studies prognostic factors includes extent of the lesion, site of primary onset, histological type and age at onset. As the majority of breast sarcoma are of alveolar type and usually presents after 10 years of age the prognosis remains poor. 5-year survival rate is 43% approximately [5].
Rhabdomyosarcoma of breast origin if identified and intervened early, satisfactory outcomes can be achieved. Rate of axillary lymph node metastasis is 21% overall and 12.5% in clinically negative axilla as per our review of literature. Some form of axillary staging should be considered in all patients with clinically positive axilla undergoing surgery for rhabdomyosarcoma. Based on current review, we are not able to make any recommendation for patients with clinically negative axilla.
Footnotes
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Taken from patient
Conflict of interest
Authors declare no conflict of interest
Funding source
No external funding
Author contributions
This is to declare that all authors have contributed to the study. No part of the manuscript has been sent for consideration elsewhere or published in any International or National journal. The authors clearly certify that there is no aspect of plagiarism. All the conflicts of interest have been clearly defined and the source of grant disclosed. Due ethical permission/consent has been obtained for carrying out the study. In case of any dispute, the authors will be held fully responsible for the statement disclosed in the cover letter. The authors are also aware of the copyright rules and also declare that they will not reproduce any published text without due permission from the journal.