
Abstract
BACKGROUND:
Schwannoma is an extremely rare benign tumour of the peripheral nervous system; its association with breast cancer is sporadic, and its association with the brachial plexus is extremely rare.
CASE DESCRIPTION:
The authors report a case of a patient with breast cancer associated with nodulation in the left supraclavicular fossa, and due to the clinical and radiological features, it was considered metastatic lymph node disease. The patient underwent neoadjuvant chemotherapy, with partial response of the breast. Surgical treatment included resection of the supraclavicular nodule, which was found to be a supraclavicular fossa schwannoma. The correct diagnosis, influences the radiotherapeutic planning. The unusual presentation led to diagnostic confusion in the present case, a fact that changed the breast treatment.
CONCLUSION:
The best of our knowledge it is the third description of brachial plexus schwannoma associated with breast cancer and the first with a synchronous association. The knowledge of this pathology and its potential to alter treatment justify the reporting of the present case.
Introduction
Schwannoma or neurilemmoma is a neoplasia of the nervous sheath of the peripheral nervous system that originates in Schwann cells, which are responsible for isolating the axons of peripheral nerves. Schwannoma is often found on the neck and flexor surface of the extremities. Its primary presence in the breast is rare, and this site corresponds to 2.6% of its primary locations, but studies are typically presented in the form of case reports. It may present as a palpable nodule or detect by a mammographic screening and thus diagnostic exclusion is confirmed only after biopsy [1–5].
The association between schwannoma and breast cancer is sporadic, but it has been reported as the differential diagnosis during staging and at initial diagnosis of primarily single lesions in the following: the liver [6], axilla [7]; especially when metastatic disease is suspected in previously treated patients [8], deep supraclavicular fossa [9,10], cauda equina [11], gluteus [12], in cases of sternal intraosseous injury [17]; in association with a metastatic lesion [13,14]; and in cases where lesions mimic a vestibular schwannoma [15]. The association of schwannoma with metastatic breast cancer at diagnosis has been described, and in that case, all lesions disappeared after treatment with the persistence of a single lesion on PET/CT [16].
Brachial plexus schwannoma is rare, as this accounts for only 5% of all cases [17]. We present a third case of schwannoma associated with breast cancer [9,10], and the first case of primary schwannoma of the brachial plexus associated with a diagnosis of breast cancer (synchronous), which led to a change in treatment.
Case description
This case is a 41-year-old patient with a history of palpable nodulation in the left breast. Clinically, she had a 2-cm retroareolar hardened nodule, and the axilla exhibited N0 stage and was associated with hardened nodulation in the left supraclavicular fossa. A mammogram of the dense breast revealed a BI-RADS (Breast imaging-reporting and data system) II lesion. Ultrasound revealed a 0.8-cm juxtapapillary nodule, which corresponded to the palpable nodule. It was also associated with the axillary lymph node, which demonstrated a strongly thickened cortex (0.5 cm). Ultrasound of the supraclavicular fossa showed a 2.6-cm suspect nodule (Fig. 1a). A core biopsy revealed an invasive ductal carcinoma, which was determined to be Nottingham grade I and luminal B HER2-negative. Staging of the chest as well as upper abdomen and lower abdomen tomography and scintigraphy showed only the presence of a supraclavicular node on the left side, which was interpreted as lymph node enlargement (Fig. 1c). The patient was clinically considered T1N3M0, clinical stage IIIC, and neoadjuvant chemotherapy was proposed.
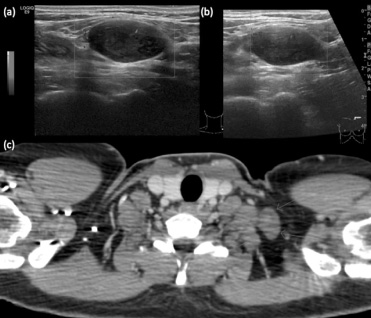
Imaging exams. (a) Pre-treatment ultrasound; (b) Post-treatment ultrasound; (c) CT scan showing left supraclavicular oval nodule.
The tumour area was demarcated on the patient (Fig. 2a) who then underwent neoadjuvant chemotherapy (12 cycles of paclitaxel followed by 4 cycles of Adriamycin plus cyclophosphamide treatment). In the evaluation of the response, a decrease of 0.8 cm was observed in the juxtapapillary image; radiologically, no lesions were detected in the armpit, and a stable supraclavicular globular nodulation was observed on the left.
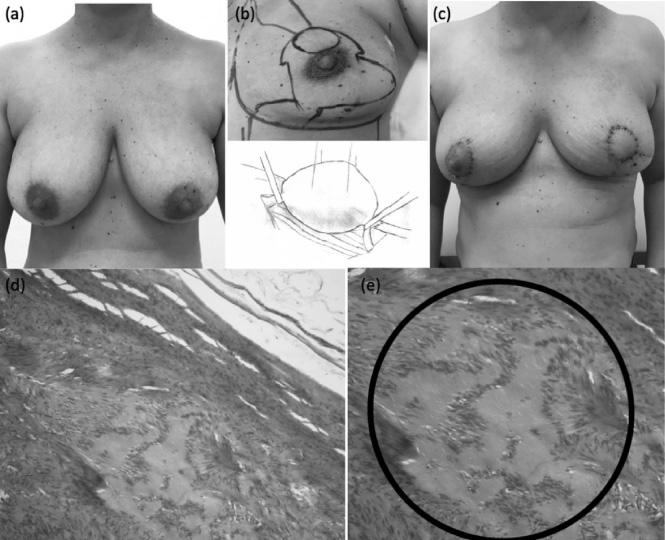
Treatment. (a) Before surgery; (b) Technique performed in the breast and supraclavicular fossa; (c) 15 days after surgery; (d) Histology, H&E 100x. Encapsulated fusocellular neoplasm with the presence of Verocay bodies but no atypia; (e) Verocy bodies in the circled area.
The patient underwent central quadrantectomy and remodelling using the geometric compensation technique [18] (Fig. 2b, 2c), which was associated with left axillary sentinel lymph node screening. Symmetrisation using the superior pedicle technique was performed on the right side. Resection of the nodular lesion was performed in the supraclavicular fossa, and the presence of a proximal and distal hardened cord was observed (Fig. 2b).
The anatomical-pathological examination revealed the presence of a 3.3-mm residual breast lesion, with two disease-free axillary lymph nodes. Left supraclavicular nodulation was determined to be a schwannoma (Fig. 2d, 2e). Postoperative motor or sensory deficits in the upper left limb were not observed. The patient underwent radiotherapy of the breast wall (4256 cGy) and is currently being treated with tamoxifen.
Schwannomas are benign entities with low malignant potential. They can develop in the dermis, in subcutaneous tissue or in nerves [17]. Typically, a slow-growing mass, which is asymptomatic or elicits symptoms associated with nerve compression, is formed. The mass is firm and not soft, with symptoms of pain or paraesthesia along the involved nerve [11]. Based on the clinical history, familial neurofibromatosis type II and schwannomatosis should be considered, but they can be ruled out by the clinical history and the absence of peripheral neurofibromas or café-au-lait spots, which are associated with neurofibromatosis type I [17].
In the brachial plexus, the presence of a palpable lesion constitutes the primary clinical presentation, but the majority of these tumours are benign. Of the benign lesions, schwannoma is the most common histological type. Ultrasound and tomography are performed routinely during the pre-operative evaluation, and resection is effective for benign lesions [19]. The tumour can occur in the root, trunk, cord or terminal branches [20]. The radiological finding is a well-defined broad nodule in a brachial plexus root. Imaging modalities that provide a high degree of soft tissue contrast and spatial resolution, such as ultrasound and magnetic resonance imaging, are adequate preoperative methods [21]. Many of these lesions have been diagnosed by PET/CT [6,9,12,22,23], especially in follow-up studies. In the present case, the clinical diagnosis of a palpable nodule in the supraclavicular fossa ipsilateral to the breast tumour, together with the ultrasound finding of hypoechoic nodulation [24], which is a frequent feature of malignant lymphadenopathy, led to diagnostic confusion.
Evaluating breast cancer, the ultrasound in an important complementary exam used in the evaluation of the axilla and suspicious supraclavicular fossa. The fine need aspiration is practical but it is associated with inferior sensibility to the ultrasound-guide core needle biopsy for lymph node evaluation. Morphological change of the cortical lymph node thickening is associated to lymph node envolvment [25,26], and besides in this case the axillary lymph node showed a strongly thickened cortex (0.5 cm) and the supraclavicular node was homogeneous, all were considered metastatic from breast cancer. Breast cancer is a regional disease. The main lymphatic metastatic local is the axilla, the second is internal mammary lymph node and the third supraclavicular. Skipping metastasis to the supraclavicular fossa represents 3.8% of the cases [27], and as it occurs no additional biopsy was performed. This erroneous interpretation represented the main limitation on the clinical conduction of this patient as biopsy was not performed in supraclavicular fossa previously to the beginning of the chemotherapy. Primary malignant, metastatic diseases or non-malignant may presented as a mass in the supraclavicular fossa [28] and Schwannoma is also infrequent. The rarity of these conditions justified the treatment performed, as a synchronous schwannoma associated to a breast cancer has not been described yet in the literature.
The diagnosis of Schwannoma can be made by core biopsy or by complete resection of the lesion. A benign neoplasm of spindle cells in nerve fascicles with hypocellular (Antoni A) and hypercellular (Antoni B) areas is observed. Immunohistochemistry shows strong and diffuse positivity for S-100, laminin and collagen IV [22]. In the present case, no core biopsy was performed before neoadjuvant treatment, and the schwannoma was diagnosed only during the surgical treatment.
The absence of neurological symptoms prior to surgery did not result in clinical suspicion. In cases of schwannoma, surgery is indicated in the presence of neurological deficit, rapidly growing lesions, suspected malignancy or to prevent or minimize neurological symptoms. Complete resection of these tumours with the preservation of the surrounding nerves should be the goal and may be combined with nerve reconstruction. The nerve fascicles surrounding the tumour are usually separable, with enucleation almost always possible [22]. In this patient, the nerve was sectioned, and no neurological complications were observed. When schwannoma occurs in major peripheral nerves, resection may cause worrisome neurological or sensory complications after surgery. Such neurological complications may be major or minor and may progress favourably during follow-up, with low tumour recurrence [29,30].
Conclusion
Schwannoma of the brachial plexus is an extremely rare entity, and its association with breast cancer is sporadic, which led to diagnostic confusion in the present case. In breast tumours with a single distant lesion, in which the histological diagnosis can alter the therapeutic approach, schwannoma must be considered in the differential diagnosis of nodules of the supraclavicular fossa, and the oncologist should consider the indication for histopathological study in the initial evaluation.
Conflict of interest
The authors declare no conflicts of interest.