
Abstract
Background:
Brachial plexus birth injuries (BPBIs) can often result in functional and cosmetic deficits including, according to a recent scoping review, elbow flexion contractures in up to 48%. A treatment algorithm that includes a custom long-arm orthosis to optimize early glenohumeral joint positioning (Sup-ER protocol) has been shown to improve shoulder range of motion. Although the protocol was not intentionally designed to affect the elbow, this study investigates the prevalence and severity of elbow flexion contractures in children treated with that protocol.
Methods:
This prospective cross-sectional cohort study examined 16 children aged 4 and older with BPBI severe enough to be treated with the Sup-ER protocol. Passive and active elbow flexion and extension range of motion (ROM) were assessed in both arms. Elbow flexion contractures were defined as > 5o from neutral.
Results:
Within the cohort of 16 patients (mean age: 7.0 years, range: 4.5-11.6 years), the mean maximal passive elbow extension was -6.2° in the affected arm and + 5.1° (hyperextension) in the unaffected arm. Zero patients had a severe elbow flexion contracture (>30o) and only 6/16 met the lowest threshold definition of elbow flexion contracture (>5o), with a mean onset at 22 months of age.
Conclusions:
This study suggests an unintended decreased prevalence and severity of elbow flexion contractures in children with more severe BPBI treated with the Sup-ER protocol, relative to published values.
Introduction
Most brachial plexus birth injuries (BPBIs) spontaneously recover to a clinically functional degree. The management of more severe cases varies with institutional preference,1,2 but outcomes associated with these will usually include some residual functional deficit or cosmetic stigmata.3-5 In the most common BPBI presentation, infants will present with initial paresis of the shoulder and elbow, but as the nerves recover, relative ongoing weakness of external rotation, and supination can lead to long-term well-defined skeletal shoulder imbalances.6,7 A similar force balance issue can occur in the elbow. An initial deficit in active elbow flexion is most common, but the natural history through nerve recovery frequently results in long-term elbow flexion contractures. Among a number of theories to explain underlying pathophysiology are included restriction or reduction of longitudinal growth of the flexor muscles, muscle fibrosis, and denervation atrophy of the flexor muscles.8-12 The incidence of elbow flexion contractures in a recent comprehensive scoping review of the subject is reported as 48%, with 21% to 36% of those contractures measuring greater than 30 degrees. 9 These more significant contractures are known to clinically impact both function and aesthetics.9,13
The literature describing elbow flexion contractures in children with BPBI is primarily focused on post-diagnostic treatments like serial casting, botulinum toxin, progressive splinting, stretching, and surgery.14-19 Even as we develop understanding of the underlying cause, there is limited evidence to support measures that prevent elbow flexion contractures.
Our clinic previously established a rehabilitative protocol implemented in early infancy which aimed to prevent secondary skeletal and joint changes in the shoulders of babies with more severe BPBI. For patients with minimal active external rotation at 6 to 8 weeks of age, the protocol introduces a custom splint that passively repositions the affected resting arm into external rotation (ER) and supination (Sup), 20 and maintains physiotherapy when not using the splint. Similar to the principles of Pavlik’s harness for hips, the goal of the Sup-ER protocol is to optimize a child’s early glenohumeral joint surface contact during shoulder girdle recovery and rebalancing; we have previously published our finding of improvements in shoulder range of motion (ROM) using this protocol. 21 Around one third of our clinic patients are prescribed this protocol and represent the more severe injuries. As part of the Sup-ER orthotic, a long arm splint is applied on the flexor surface, holding the elbow in extension. 20 This splint is worn during nights and naps for several months, following a recommended initiation period of use of 20 to 22 hours per day. Although the protocol was not intentionally designed to affect the active or passive range of the elbow, we discovered during the analysis of ROM data in a recent shoulder rotation function study, 21 a tendency toward fewer than expected elbow flexion contractures. After comparing to a number of recent BPBI elbow contracture publications we were motivated to independently analyze the potential effect the Sup-ER protocol may have in reduction or prevention of significant elbow flexion contractures. 17
The goal of this study is to specifically investigate the prevalence and severity of elbow flexion contractures in a cohort of patients being examined for the effect of the Sup-ER protocol on shoulder function.
Methods
This study used secondary data previously collected but not reported in a prospective cross-sectional cohort study of shoulder function, undertaken with the approval of the University of British Columbia Children’s and Women’s Health Center of British Columbia Research Ethics Board (H18-01006). Parents signed informed consent, and children over 7 years of age provided their informed assent.
Study Participants
All BC Children’s Hospital BPBI patients who had been prescribed the Sup-ER protocol, with or without any other procedures, and who were 4 years or older at the time of the study had been invited to a comprehensive evaluation of shoulder rotation function. 21 Global upper extremity measurements, including elbow range of motion, were collected at the same visit. The study excluded patients lost to follow-up, who had moved residence from BC, or with cooperation issues rendering them unable to complete the study assessment.
Data Collection
Physical data were collected during a single 1-hour study visit. Medical and procedural history and Sup-ER protocol details were documented from patient records. While assessing passive and active elbow flexion and extension during the global upper extremity examination, the unaffected arm was always measured first. Both a physiotherapist and a trained clinical evaluator measured all participants consistently.
Range of Motion
Elbow flexion and elbow extension ROM were measured in standing with the upper arm in adducted resting position. The trunk was stabilized by a parent or clinical evaluator to minimize compensatory movements. An analog goniometer centered on the lateral epicondyle was used to measure both flexion and extension. Angles were recorded through a 0° to 180° range with 0° representing a neutrally straight elbow (Figures 1 and 2). For clarity, elbow extension deficits are reported as negative values, and hyperextension beyond neutral as positive.
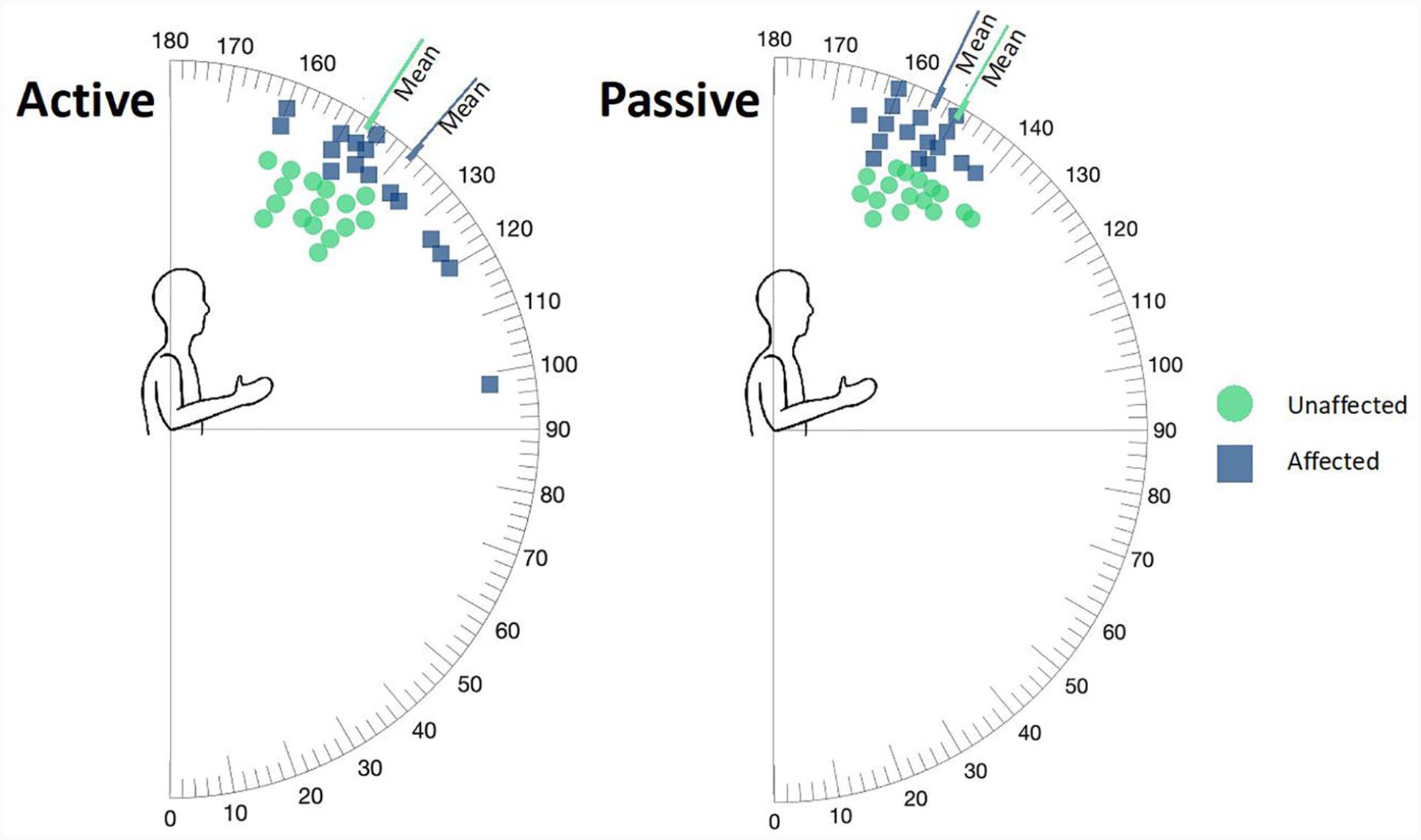
Elbow flexion active and passive range of motion in children with brachial plexus birth injuries treated with the Sup-ER protocol.
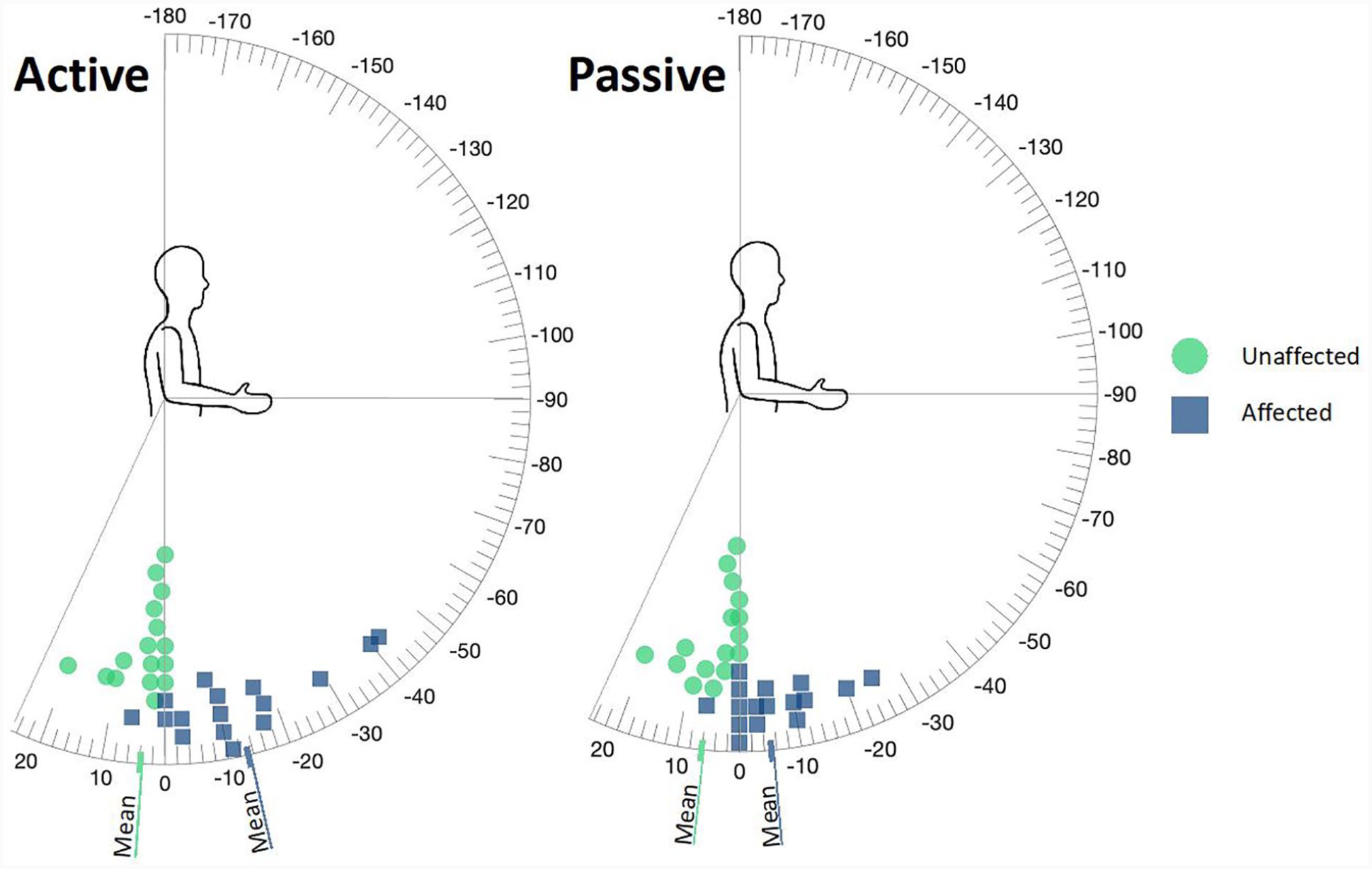
Elbow extension active and passive range of motion in children with brachial plexus birth injuries treated with the Sup-ER protocol.
In current literature an “elbow flexion contracture” is deemed to be present when the patient can extend maximally to no straighter than 10° from neutral, or in other words flexion contracture is defined as 10° or greater.17,19 Previous literature has also described contractures as deformities >5°, ≥10°, or >10° from zero. 22 - 24 For our documentation and analysis, we chose to define elbow flexion contractures with the lowest threshold published definition: > 5° from neutral.
Controls
The unaffected arm in each child acted as internal control for all measurements. We had not prospectively collected elbow flexion deformity measurements consistently or formally in our clinic database prior to this, so for this work we looked for controls in published studies measuring elbow extension range with similar enough technique to allow comparison.
Results
Of 32 invited children with BPBI severe enough to be treated with the Sup-ER protocol, 17 consented to participate in the study. One child on the autism spectrum was withdrawn when they demonstrated inability to cooperate with acquisition of study measurements. Ultimately, we report here on a cohort of 16, with 13 females and 3 males examined at a mean age of 7.0 years (range: 4.5-11.6 years) (Table 1).
Patients with BPBI Treated with the Sup-ER Protocol: Case Series Demographics.
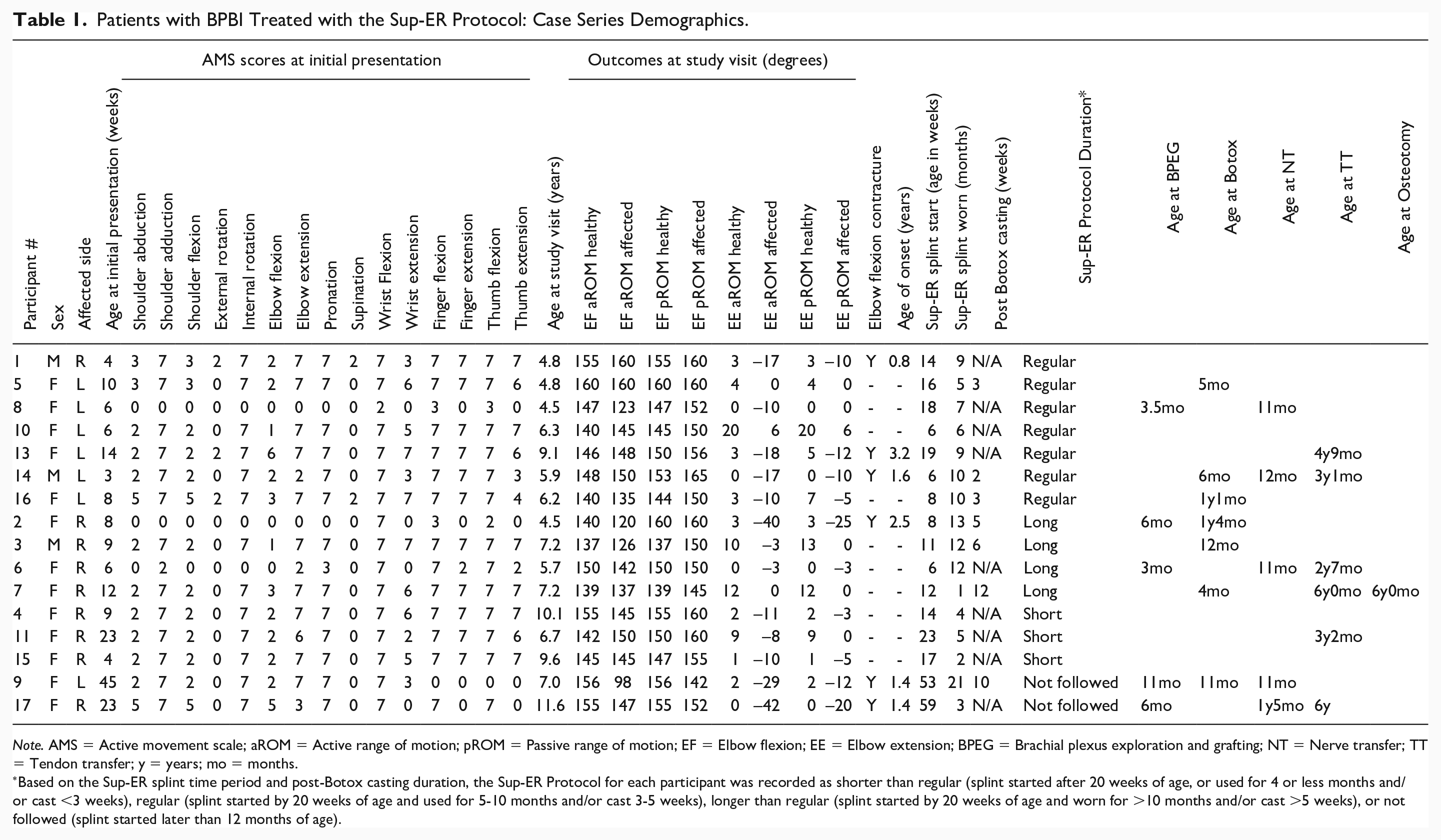
Note. AMS = Active movement scale; aROM = Active range of motion; pROM = Passive range of motion; EF = Elbow flexion; EE = Elbow extension; BPEG = Brachial plexus exploration and grafting; NT = Nerve transfer; TT = Tendon transfer; y = years; mo = months.
Based on the Sup-ER splint time period and post-Botox casting duration, the Sup-ER Protocol for each participant was recorded as shorter than regular (splint started after 20 weeks of age, or used for 4 or less months and/or cast <3 weeks), regular (splint started by 20 weeks of age and used for 5-10 months and/or cast 3-5 weeks), longer than regular (splint started by 20 weeks of age and worn for >10 months and/or cast >5 weeks), or not followed (splint started later than 12 months of age).
Elbow Flexion
The mean maximal
Elbow Extension
The mean maximal
Almost 63% of participants (10/16) had affected-arm elbow passive extension straighter than the >5° deficit required to meet even the lowest threshold definition of elbow flexion deformity. Six of those achieved between 0° and 6° of hyperextension, though the participant with the 6° of hyperextension was hyperextensible to 20° on the unaffected side (Figure 2).
Defined elbow flexion contractures >5° were found in 6/16 (37.5%) children, with mean onset of 22 months (Table 1, Figure 3). The mean elbow flexion contracture was 15°, the median was 12°, and the maximum was 25°. Although all participants started the Sup-ER protocol, of the children that had elbow flexion contractures, there was no relationship observed between the degree of elbow flexion contracture and the length or degree of compliance with the Sup-ER protocol, or the undertaking of other surgical or medical procedures. Of note, both participants who started the protocol after age 1 had elbow flexion contractures (12° and 20°). Also of note, a participant who started the protocol at 8 weeks of age, presented our maximum elbow flexion contracture, but their course was complicated by significant surgical and clinic-visit delays, and difficulties with splinting and physiotherapy compliance due to participant’s severe chronic respiratory illness (Table 1).
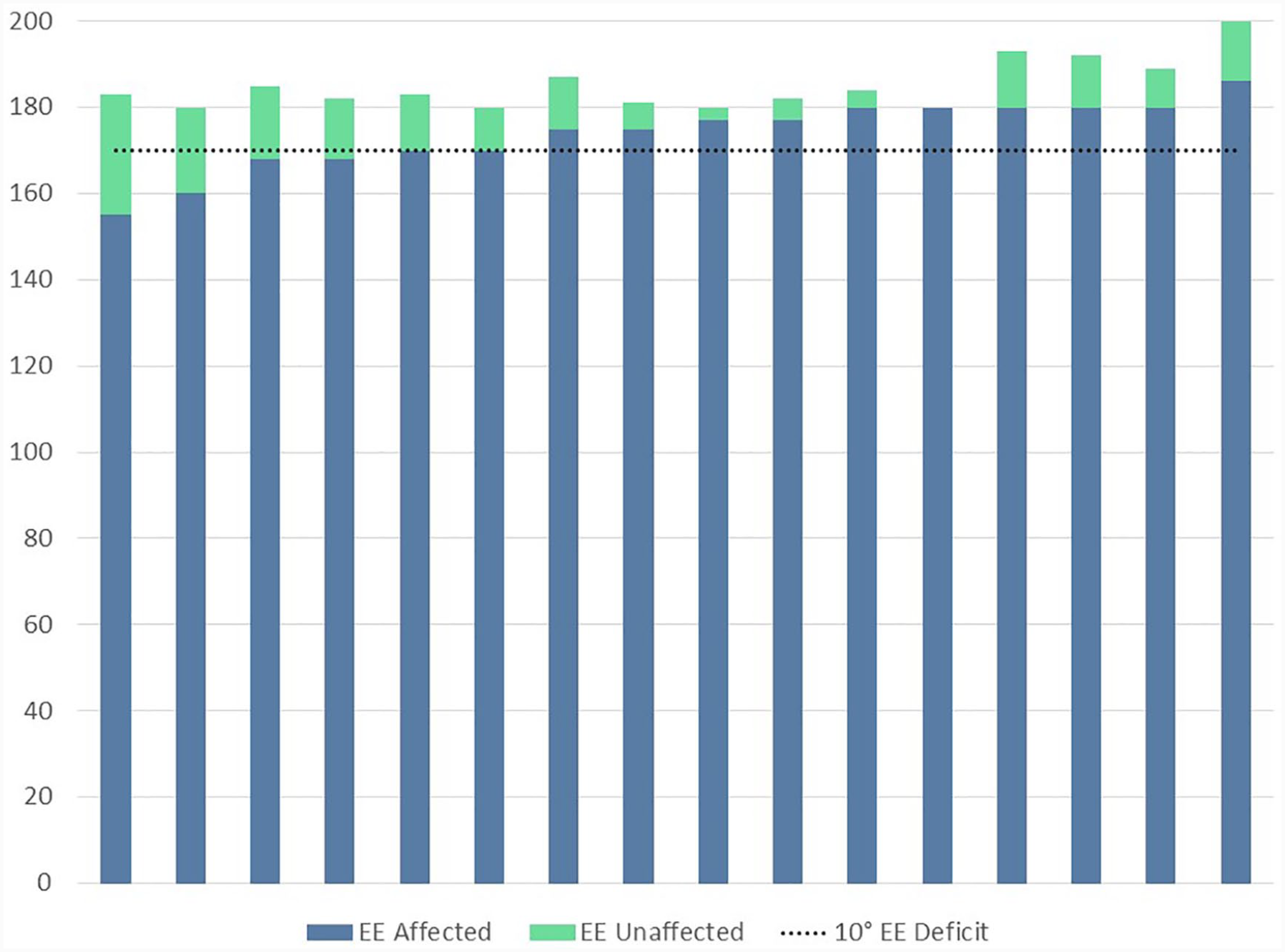
Passive elbow extension range of motion in the unaffected and affected arms of children with brachial plexus birth injuries treated with the Sup-ER protocol.
To take into account natural hyper-extensibility, the deficit in maximal passive elbow extension between affected and unaffected side of each child ranged from 0 to 28°, with a mean difference of 11°. This pattern is similar to the differences we found measuring from 0° (Figure 3).
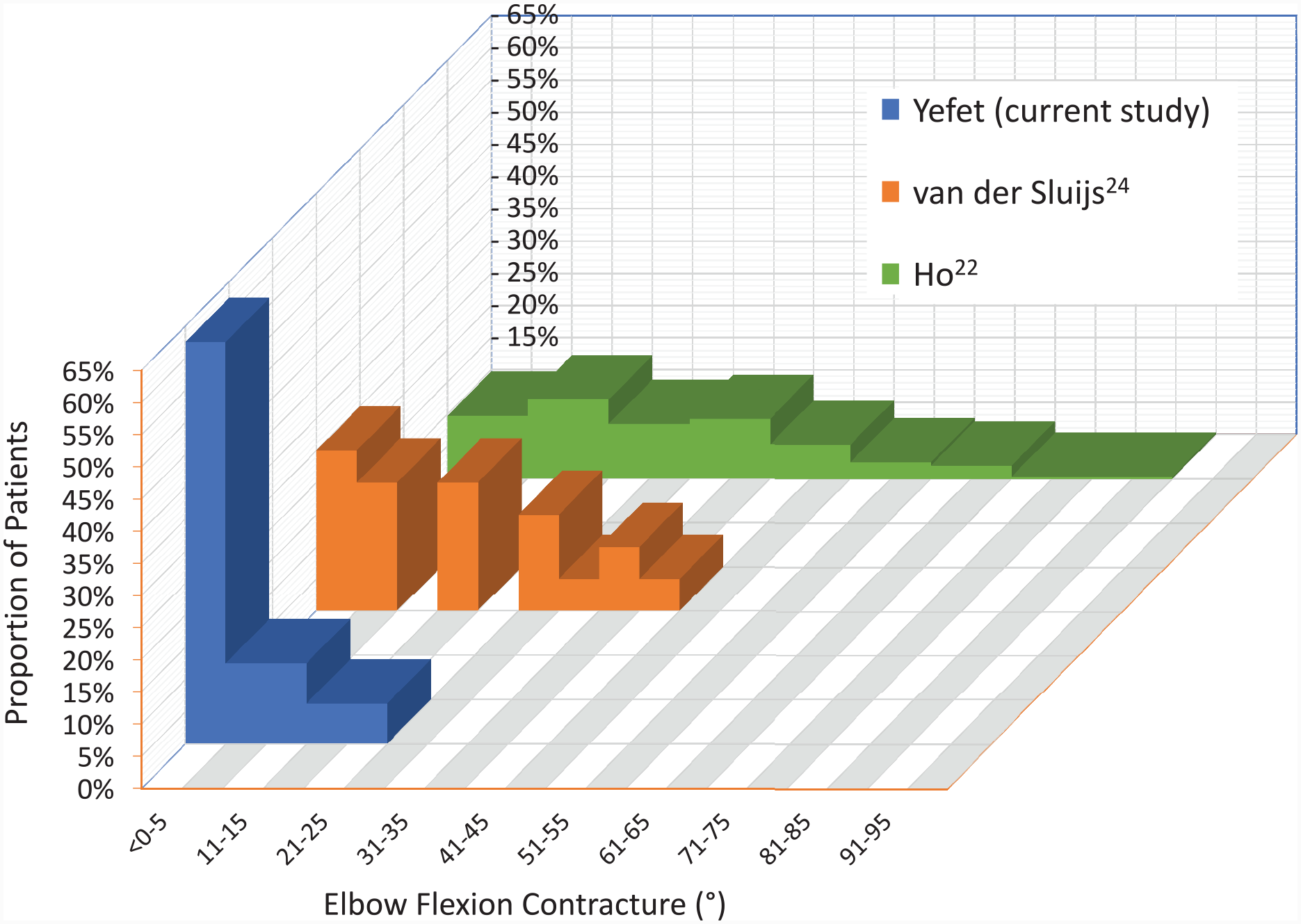
With more than 60% of our participant group showing no elbow flexion contractures at all, and the rest distributed between 10° and 25°, this cohort displays a favorable pattern relative to the distribution found in comparable literature (Figure 4).
Discussion
The primary goal of the Sup-ER protocol was to maintain anatomic congruency of the glenohumeral joint as the nerve injuries healed, by resting the arm in external rotation and the forearm in supination. During the early evolution of our splint design, recognizing the inherent tendency in the BPBI population toward elbow flexion contractures, we moved from an elbow-flexed splint to an elbow-extended position. In this study group, we see fewer and less severe elbow flexion contractures than the literature would suggest might be present.
A recent scoping review determined the prevalence of elbow flexion contractures to be 48% in children with BPBI. 9 Between 10% and 17% had contractures greater than 30°, with a range in contractures between 5 and 90°. The prevalence of all elbow flexion contractures in our cohort (at a mean age of 6.4 years) compares favorably (37.5% vs. 48%) to the literature. More notably, our mean elbow flexion contracture was 12°, less than mean measurements previously described in comparable case series.22-24 This study included ONLY patients with our clinic’s most severe BPBI, so this group should over-represent elbow flexion contractures within our population. Furthermore, despite the severity of their BPBI, we found zero participants (0% vs. 10% to 17%) with severe (>30°) contractures; those usually associated with functional and aesthetic sequelae. 13 Three of the children with defined contractures followed a regular Sup-ER protocol, one followed a longer than normal protocol, and 2 children did not follow the Sup-ER protocol as per our recommended criteria. This makes definitive conclusions and associations difficult, however, an overall pattern of elbow flexion contracture reduction suggests an unintended positive effect of the Sup-ER protocol that may warrant further consideration in prevention efforts.
The etiology of elbow flexion contractures in BPBI is incompletely understood, but in large part may be due to reduced longitudinal growth of the flexor muscles with or without the presence of biceps brachii overactivity.8,11,25 Although not an intended primary goal, we wonder if the en-passant early elbow extension positioning in the Sup-ER splint may have helped to maintain some of the absolute length of elbow flexors during a time of known reduction of rapid growth. Otherwise, perhaps simply improving shoulder positioning early reduces secondary elbow forward compensatory movements. We have wondered if the elbow forward position in function and functional rest combined with gravity, emphasizes constant elbow flexion, without frequent rests into extension.21,26
Efforts to achieve good shoulder balance can be either preventive or corrective surgically. These data support a possibility that choosing an early preventive strategy involving a long arm splint may offer an additional advantage to elbow passive range that would not likely be achieved with corrective shoulder surgery alone.
Splint-positioning the shoulder in passive external rotation is logically more efficient with a bent elbow, as per our prototype design. We were reassured through clinical ultrasound that the long arm extension format achieves adequate ER to improve or normalize the glenohumeral alpha angle. But our findings here have reinforced that a long arm extension splint may also provide an advantage to recovery more distally at the elbow.
This study is limited by the small sample size which hinders statistically significant conclusions. About half of invited children agreed to participate; there may be selection bias given the nature of voluntary participation. Anecdotally, we do feel this participant cohort is a fair representation of our intended clinic population. The goniometer type used in this study has been shown to have fair to excellent interrater reliability and maximal errors of up to 10.3°.27,28 Many of our measured ranges were between 0 and 10° from neutral. Repeating measurements and limiting their acquisition to a single pair of experienced evaluators were intended to reduce potential errors. Comparing to published literature is less desirable than comparing data prospectively collected in the same study or database. We regret not previously formally collecting accurate elbow flexion range in our larger database. It would be interesting to see in our recent and historical non-Sup-ER population what the elbow flexion deformity details were.
In conclusion, this study demonstrates an unintended decreased prevalence and severity of elbow flexion contractures in children with severe BPBI treated with the Sup-ER protocol, relative to published values. The etiology of elbow flexion contractures is multifactorial. We hypothesize that the observed improvement may be due to early consistent elbow extension positioning, with consideration that muscle fibers may more readily maintain their length during a critical growth phase. We are interested in studies further evaluating muscle length, growth patterns, and flexor tendon/muscle length ratio of patients treated this way.
Footnotes
Acknowledgements
We wish to thank Ms. Norine Mayede for helping our team coordinate the study visits.
Ethics Approval
This study was approved by The University of British Columbia Children’s and Women’s Health Center of British Columbia Research Ethics Board (H18-01006). Parents signed informed consent and children over 7 years of age provided their informed assent.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study. Parents signed informed consent and children over 7 years of age provided their informed assent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Leoor Yefet was awarded a UBC Summer Student Research Program grant for this study. This study was also awarded a UBC Plastic Surgery academic grant that helped pay for a digital goniometer, as well as parking and study incentives for participants.