
Abstract
We present a case of surgical removal of primary amyloidosis of the breast utilizing an oncoplastic reduction pattern technique. Primary amyloidosis of the breast is a very rare benign disease characterized by accumulation of insoluble amyloid protein. Biopsy is required for definitive diagnosis, and surgical removal of the mass with clear margins is the main treatment for primary amyloidosis. Oncoplastic reduction pattern technique allows for removal of large breast lesions and correction of the resulting defect by combining the extirpative principles of surgical oncology with the aesthetic principles of breast reduction surgery.
Introduction
Amyloidosis of the breast is a rare disease characterized by extracellular deposition of abnormal fibrillar amyloid protein. Amyloidosis may be classified as primary or secondary. Primary amyloidosis is limited to a particular organ, whereas secondary amyloidosis is a manifestation of systemic amyloidosis. Primary breast amyloidosis is the result of localized production of immunoglobulin light chains due to plasma cell dyscrasia [1]. First described in 1973, breast amyloidosis has only been reported through case reports and case series [2,3].
Despite being clinically benign, a palpable mass of insoluble amyloid protein is worrisome to patients, and may mimic breast malignancy clinically and radiographically. Treatment for primary breast amyloidosis is excision of the mass with clear margins. Depending on the size of the mass, surgical deformity of the breast can result. Oncoplastic reduction technique allows for removal of a large breast mass while also achieving cosmetically satisfactory results. We present a case of a large primary amyloidosis mass that was excised successfully using oncoplastic reduction pattern technique, and review treatment recommendations.
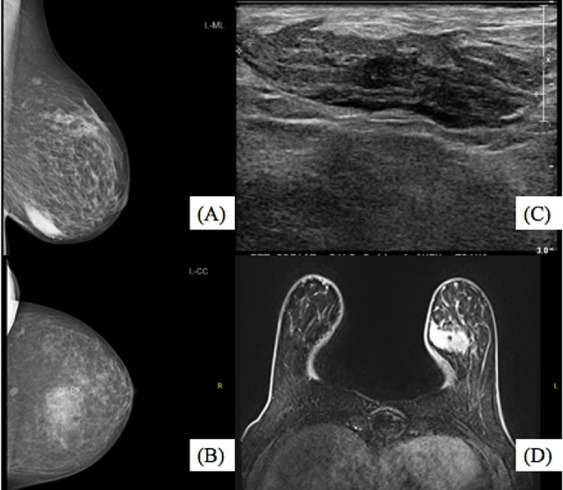
(a) Left MLO mammogram view of mass (b) Left CC mammogram view of mass (c) US of left breast at 6:00, 6CFN (d) MRI of left breast mass.

(a) Left breast with wire bracketed localization with Wise Pattern Reduction pattern markings (b) Breast tissue excised with overlying skin and clear margins (c) Oncoplastic closure.
A 66-year-old female presented with a palpable non-tender left breast lump of two weeks duration. Physical exam revealed an oblong mass measuring 4 × 2 cm in the left breast at the 6 o’clock position, occupying over twenty percent of her breast volume and close to overlying skin. No axillary lymphadenopathy was noted, and contralateral right breast exam was unremarkable. Imaging of the left breast revealed a 3.9 cm mass (Fig. 1). Ultrasound-guided biopsy revealed amyloidosis involving monoclonal plasma cells with extensive amyloid deposition, consistent with primary kappa-light chain amyloidosis. Systemic workup, including PET scan and bone marrow biopsy, was negative except for the FDG avid left breast lesion.
A Wise pattern reduction oncoplastic approach was utilized with a superior-medial pedicle for wide excision of the large breast mass allowing for removal of overlying skin as an anterior margin. The nipple-areolar-complex was subsequently repositioned, and breast tissue in the inferior pole was mobilized to close the acquired surgical defect. A contralateral breast reduction/mastopexy for symmetry was performed at the same surgery (Fig. 2).
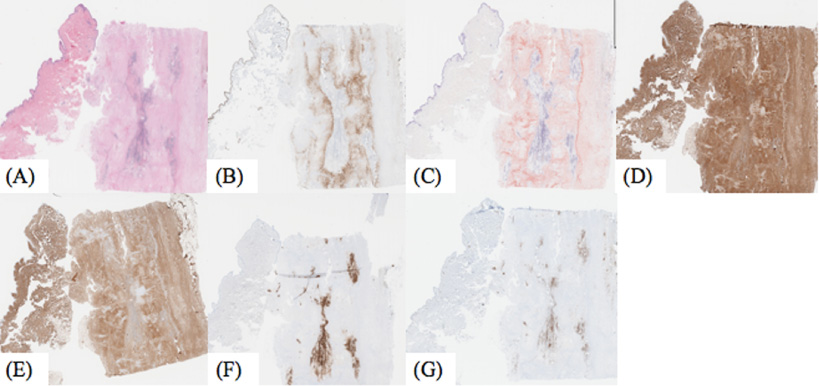
Pathology of final specimen (a) H&E (b) CD138 indicating plasma cells (c) Congo red positive staining for amyloid (d) Kappa light chain positive (e) Lambda negative (f) CD20 positive for B-Cells (g) CD3 positive for T cells.
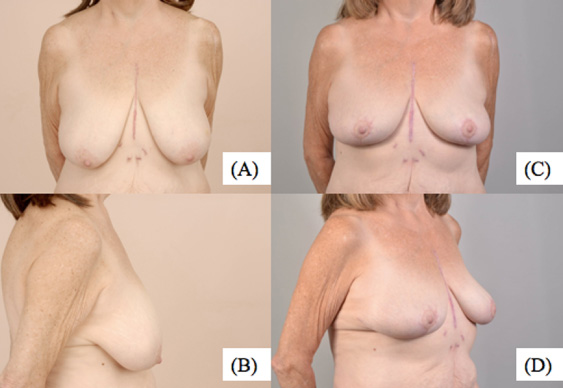
(a)–(b) Pre-operative (c)–(d) 4 months post-operative bilateral oncoplastic reduction photos of patient.
Final surgical pathology immunohistochemical staining with CD138 showed the specimen was positive for plasma cells. A Congo red stain was positive for amyloid deposition and kappa light chain, but negative for lambda. CD20 and CD3 were positive, all confirming the diagnosis of amyloidosis (Fig. 3). All resection margins were clear, and the patient was very satisfied with her cosmetic result (Fig. 4).
Primary breast amyloidosis is a rare condition not well characterized in the literature. Breast amyloidosis most often presents as a palpable, painless mass, but has also been reported as a mass with or without associated microcalcifications, skin thickening, or an asymmetry on imaging, mimicking cancer [2]. Definitive diagnosis of breast amyloidosis is made with tissue biopsy. Histologically, amyloidosis may also be distinguished from other conditions by Congo red stain, which identifies amyloid deposits through apple-green birefringence under polarized light [4]. Diagnosis of breast amyloidosis necessitates staging work-up to rule out systemic disease and distinguish between primary and secondary subtypes. Some reports have shown amyloidosis to coexist with breast cancer, which must be ruled out [5,6]. Other reports show that breast amyloidosis has a 50% incidence of associated systemic disease. Localized, primary breast amyloidosis, uncomplicated by systemic amyloidosis, has a benign clinical course and good prognosis [1].
Once confirmed to be primary amyloidosis, treatment is excision of the benign amyloid mass with clear margins. Traditionally, oncoplastic reduction lumpectomy has been utilized for correction of defects resulting from breast cancer excision, as well as large benign breast lesions [7]. Our patient had a large mass, approximately 4 cm, for which overlying skin resection was necessary to achieve a clear anterior margin. The volume removed would leave a large cosmetic defect at her inferior pole, which is known to be high-risk for resultant breast deformity. Surgical excision using an oncoplastic reduction approach allowed for appropriate oncologic excision with clear margins while optimizing cosmesis and symmetry.
In the absence of malignancy, radiation therapy and chemotherapy are unnecessary following excision for primary amyloidosis. Prior case reports suggest patients to undergo a mammogram of the affected breast at 6 months postoperatively, which will serve as the new baseline for future mammograms, although the benefit of this has not been validated. If no areas of concern are noted, the patient may resume annual screening mammograms.
Conclusion
Primary amyloidosis of the breast is a rare condition in which insoluble amyloid protein deposits extracellularly, most commonly resulting in a painless, palpable mass. To confirm this benign etiology, thorough workup is necessary to rule out malignancy and distinguish between localized and systemic amyloidosis. Excision is the definitive treatment. For large masses, an oncoplastic reduction pattern technique may be used to correct the resulting defect in a cosmetically preferable fashion.