
Abstract
Intracystic papillary carcinoma (IPC) is a rare malignancy of the breast which is usually found in postmenopausal women. It is still rarer in males and may present with signs of a benign cystic lump. It is sub-classified into three equally prevalent groups considering treatment strategies: intracystic papillary carcinoma alone, intracystic papillary carcinoma with ductal carcinoma in-situ, and those with evidence of invasion. Even if a preoperative diagnosis is achieved, there are no specific guidelines for the treatment of IPC. Treatment modalities including the extent of surgical excision, lymph node dissection, radiation, and chemotherapy are determined by the grade and size of the lesion and sub-types. However, several reports and studies showed good prognosis with conservative surgery without axillary dissection in IPC not associated with carcinoma in situ or micro-invasion. We present a 40 years old male patient with IPC who was managed by modified radical mastectomy and adjuvant hormone therapy. A brief review of the literature and clinical characteristics, pathology, and treatment of IPC are discussed.
Introduction
Intracystic papillary carcinoma constitutes about 0.5% to 1% of all breast carcinoma, primarily affecting postmenopausal women [1]. It is sub-classified into three equally prevalent groups considering treatment strategies: intracystic papillary carcinoma alone, intracystic papillary carcinoma with ductal carcinomain-situ, and those with evidence of invasion [1]. It is a low-grade carcinoma with good prognosis as compared to invasive micropapillary carcinoma. Treatment modalities including the extent of surgical excision, lymph node dissection, radiation, and chemotherapy are determined by the grade and size of the lesion and sub-types mentioned above. We present the case of a 40 year-old male with intracystic papillary carcinoma of the breast and review the current literature on the condition.
Case report
A 40-years-old male presented to us with complaints of a lump in his left breast, associated with bloody discharge from his left nipple. On physical examination, a 3 × 4 cm, smooth, cystic mass was found in the subareolar region of his left breast which was not fixed to skin, underlying muscle or chest wall. There was no active discharge at presentation, but the nipple was found to be retracted. There were no lymph nodes palpable in the left axilla. Ultrasound of the breast revealed a cystic lesion with eccentric papillomatous mass in subareolar area of the left breast [Fig. 1]. Ultrasound examination of the axilla didn’t reveal any suspicious lymph nodes in the left axilla. USG-guided fine needle aspiration cytology (FNAC) from the solid area in the cystic lesion confirmed the diagnosis of carcinoma. A left sided modified radical mastectomy was done as the definitive surgical treatment [Fig. 2]. Histopathological examination confirmed the diagnosis of intracystic papillary carcinoma with evidence of invasion and invasive component was infiltrating ductal carcinoma with intracellular and extracellular mucin. Lymphovascular and perineural invasion was also present, but there were no metastatic lymph nodes in the axillary lymph node dissection specimen. Estrogen and progesterone receptors were present on immunohistochemistry (IHC) and there was no over-expression of HER-2. Patient was given adjuvant hormonal therapy with tamoxifen.
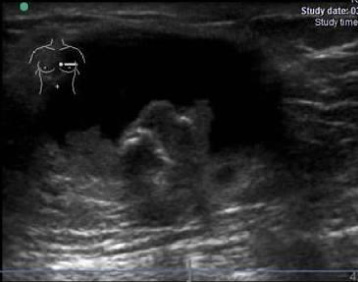
Ultrasound image of left breast showing cystic lesion with eccentric papillomatous mass.
Carcinoma in male breast accounts for about one percent of all breast carcinomas [1]. Similarly, intracystic papillary carcinoma (IPC) in itself is an uncommon entity accounting for 1–2% of all breast malignancies [2]. But, some reports suggest that it is relatively more common in men and 3.5% of IPC were found in males in a large, retrospective study of more 917 patients of IPC [3]. Although, IPC has been associated with a more favourable outcome, the diagnostic and treatment strategies have not been standardized and there are no universally accepted guidelines leading to some confusion in its management. The literature regarding IPC in males is also scant and to the best of our knowledge less than 20 cases have been reported, although in a retrospective analysis of the California Cancer Registry, 32 patients out of 917 were males [3].
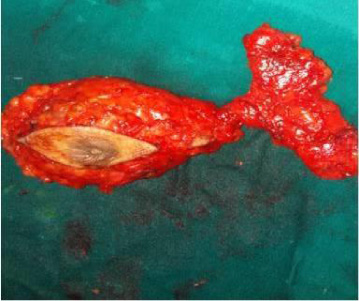
MRM specimen.
The nomenclature and classification of IPC is also confusing. It is classified as papillary carcinomas into the invasive and non-invasive forms. The non-invasive form is then further subdivided into the diffuse form, the papillary variant of DCIS, and the localized form, termed “intracystic” or “encysted” papillary carcinoma This localized form, IPC, describes a solitary tumor in an encysted or dilated duct [4]. The presence of a layer of myoepithelial cells (MECs) at the periphery of areas of papillary carcinoma have historically been used to define a lesion as in-situ rather than invasive. Recent studies have shown that, in contrast to papillary DCIS, IPC does not appear to have an MEC layer surrounding the tumour nodules [5]. This observation has lead to the idea that, in some cases, IPC may not actually be an in-situ carcinoma but may actually be an encapsulated nodule of low-grade invasive carcinoma or may be part of a spectrum of progression intermediate between in situ and invasive disease [5].
The diagnostic evaluation of lump in a male breast usually involves an ultrasonographic (USG) evaluation. On USG, the IPC has variable picture, ranging from the presence of an intraductal lesion to a completely solid mass almost completely filling the cyst or duct. Color doppler can be of some value as well, because some authors believe that it is more vascular [6]. Mammography is believed to be less valuable because it can miss small lesions and when a lesion is found, it may appear as having features of a benign lump [7].
To distinguish between benign from malignant and in situ from invasive papillary lesions of the breast, identification of a myoepithelial cell layers is essential and is done by immunohistochemical analysis [5]. Complete lack of myoepithelial cell layers both in the proliferating intraluminal component of the lesion and in the basal layer at the periphery with surrounding fibrous capsule is the classical picture of IPC. IPC is considered as an encapsulated low-grade invasive carcinoma and placed between progression of lesion from in situ to invasive carcinoma [3,8]. In a review of 19 cases of male IPC, only 2 of the 10 cases where FNAC was performed were reported as positive with a preoperative diagnosis of papillary neoplasm, while 3 cases had core needle biopsy showing papillary neoplasm [6]. Hence, excision biopsy is recommended in all cystic lesions in the male breast if the results are inconclusive.
These patients are assumed to have a favourable prognosis (relative survival rate more than 95% at 10 years) and surgery in the form of BCS or mastectomy with or without axillary staging have yielded equivalent results [3]. They are at very low risk of local recurrence and axillary or distant metastasis and hence the role of adjuvant therapies is also not well defined [3]. Fayanju et al. reviewed the management of 45 patients with IPC and concluded that associated pathology (DCIS or micro-invasion) is the most important factor determining the use of radiation and endocrine adjuvant therapy. These therapies were not of much value in patients with pure IPC. If the treatment of IPC is tailored according to associated pathology (breast DCIS or invasion), its prognosis is still excellent [9].
Intracystic papillary carcinoma of male breast is an extremely uncommon entity and a high index of suspicion is required to arrive at a correct diagnosis All cases of cystic lump in males should be excised if malignancy cannot be ruled out conclusively Breast conservation or mastectomy, both provide adequate oncological outcome Role of adjuvant therapies is questionable, but in absence of any specific guidelines it should be guided by the associated in-situ or microinvasive disease.
Footnotes
Conflict of interest
None of the authors declare any conflict of interest, financial or otherwise.