
Abstract
We report a case of intracystic papillary carcinoma of the right breast in a 59-year old man presenting with bloody nipple discharge for 1 week prior to presentation. Mammography, ultrasonography, and core needle aspiration were consistent with intracystic papillary carcinoma. The patient underwent right simple mastectomy. Pathology was also consistent with low grade intracystic papillary carcinoma. The 21-gene assay revealed a recurrence score of 0, corresponding to a 3% risk of distant recurrence at 10 years. A patient did not receive chemotherapy or post-mastectomy radiotherapy. The patient was placed on tamoxifen and has been free of disease to date.
Introduction
Male breast cancer is a rare entity, accounting for about 1% of all breast cancers diagnosed each year in the US and UK.1,2 The exact etiology of male breast cancer is unknown. However, gynecomastia, radiation exposure, imbalance in estrogen-testosterone ratio, obesity, BRCA2 mutations have all been implicated as risk factors.3–6 There has been some speculation that intracystic papillary carcinoma (IPC) in particular may present more often in men with gynecomastia.7,8 Intracystic papillary carcinoma is rare in male breast cancer, reported to comprise 2.6-5% of male breast cancers.9,10 Here, we report a case of intracystic papillary carcinoma of the breast in a male patient.
Case Report
A 59-year old man presented with a right breast mass that had been palpable for over a year. He noticed a bloody nipple discharge one week prior that prompted him to have the mass examined. Mammogram revealed a 3.4 cm round nodular density in the right breast 3 cm from the nipple and mild gynecomastia in both breasts (Figure 1A). Ultrasound showed a complex cystic and solid mass with debris and nodular lobulated solid echogenic components (Figure 1B). Core needle biopsy showed fragments of papillary carcinoma.
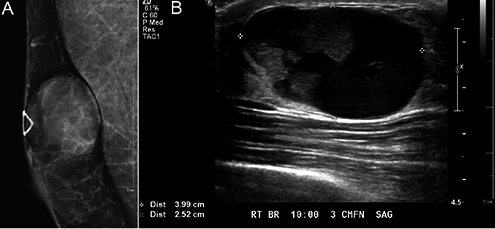
Imaging of intracystic papillary carcinoma. A) Mammogram shows a 3.4 cm round nodular density in the right breast. B) Ultrasound shows a complex cystic and solid mass.
The patient smoked in the distant past and drinks socially. Family history was significant for a father who died of stomach cancer in his 30s and a maternal cousin with prostate and colon cancer. The patient underwent genetic testing for BRCA1 and BRCA2 and no mutations were found. Radiological exam of head, chest, and abdomen revealed no metastatic disease.
The patient underwent right simple mastectomy with sentinel lymph node biopsy. Pathology of specimen showed a 3.5 cm IPC with an overall histologic grade of 1, with no lymphovascular infiltration (Figure 2). Immunostains for myoepithelial cells with p63 and smooth muscle myosin heavy chain antibodies were negative, supporting the presence of invasive carcinoma. Surgical margins were negative for in situ and invasive carcinoma. 5 sentinel lymph nodes were examined and negative for disease. The pathologic staging was pT2, psnN0. Immunohistochemistry showed that the tumor was positive for estrogen and progesterone receptors, negative for HER-2/neu amplification, and had a Ki-67 score of 10%. The patient did not receive radiation therapy or chemotherapy. He was placed on tamoxifen and is tolerating it well without side effects. The 21-gene assay (Oncotype DX, Genomic Health Inc., Redwood City, CA, USA) was sent out to predict the recurrence risk. The recurrence score was 0, corresponding to a 3% risk of distant recurrence at 10 years.
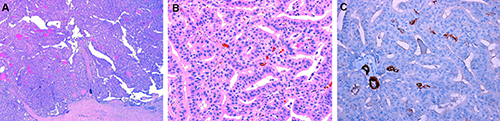
Immunohistochemistry of intracystic papillary carcinoma. A) A thick fibrous capsule is evident on low-power examination. The capsule surrounds a nodule composed of complex epithelial fronds with fibrous vascular cores (Hematoxylin & Eosin stain, 40×). B) Fibrovascular cores are covered by monomorphic neoplastic cells with low grade nuclei and amphophilic cytoplasm. Myoepithelial cells are absent (Hematoxylin & Eosin stain, 200×) C) Immunohistochemical stain using smooth muscle myosin heavy chain demonstrates lack of myoepithelial cells (DAB and Hematoxylin, 200×).
Discussion
Intracystic papillary carcinoma, also known as encapsulated papillary carcinoma, is an encysted, localized variant of papillary ductal carcinoma surrounded by a fibrous capsule found within a dilated duct. It has an estimated incidence of 0.5-2% among all breast cancers and is usually found in postmenopausal Caucasian women, with a median age of 69.5 years.11,12 IPCs in male patients are rare, comprising only 3.5% of 927 IPC cases. 13 A study of breast cancer in men using the National Cancer Institute Surveillance, Epidemiology, and End Results data from 1973-1998 found 2.6% of male breast cancers with papillary histology. 10 The majority of reported cases of IPCs in men are case reports, with a significant proportion of the cases involving Japanese male patients.14–16 Male patients are usually diagnosed in their 70s and 80s. 17
IPCs can be asymptomatic or present with a palpable breast lump or bloody nipple discharge. Preoperative diagnosis of IPC can be difficult and definitive diagnosis is usually made after excisional biopsy. 18 A mammogram will usually show a well-circumscribed, round, oval or lobulated mass. On ultrasound, IPCs will commonly reveal a complex, predominantly hypo-echoic cystic mass with more than one mural nodule. Macroscopically, the cyst is surrounded by a thick fibrous wall and blood clots are found within the lumen and on the cyst wall. 11 Histologically, IPCs are malignant ductal cells that form arborizing fibrovascular stalks lined by epithelial cells. Unlike papillary DCIS, however, IPCs do not appear to have a basal myoepithelial cell (MEC) layer, and MEC markers, such as p63, actin, and calponin can be useful in differentiating between IPCs from papillomas.19,20 Therefore, it has been suggested that IPC be considered as an encapsulated nodule of low-grade invasive carcinoma.
No clearly defined guidelines have been established for treating IPC, largely due to its low incidence and wide spectrum of morphological features. Surgical excision with negative margins is considered the mainstay of treatment. 21 Solorazano et al. noted that, given the rarity of axillary node metastases in their study of 40 IPCs, that axillary lymph node dissection was not justified. 18 They recommended sentinel node biopsy as an alternative.
Adjuvant therapy with hormonal and radiotherapy have been reported, but their benefit have been largely inconclusive. 30% of the patients in Solorazano's IPC series received adjuvant radiotherapy. 18 The authors reported that the use of radiation did not influence recurrence or survival. In their review of 40 IPC cases, Wynveen et al. reported all cases as estrogen receptor positive, most as progesterone positive, and all negative for HER2. 22 Half of the patients received hormonal therapy with either tamoxifen or aromatase inhibitors. The authors noted that it was difficult to interpret the benefits of radiotherapy and hormonal therapy, given the limited number of cases, that adjuvant treatments were frequently administered together, and that the original diagnosis of IPC introduced a bias for more aggressive treatment.
Patients with IPCs have excellent prognoses. IPCs are relatively slow growing, with reported survival rates of 100% at 10 years and a disease-free survival rate of 91%. 23 The consensus from several studies are that, irrespective of treatment modality, recurrence rate is low and survival is excellent.18,24,25
Conclusions
Intracystic papillary carcinomas in males remain an uncommon disease. First-line treatment is surgical excision with negative margins. The use of adjuvant therapy with hormonal therapy and radiotherapy remains unclear. Prognosis is excellent, with a low recurrence rate and high survival rate.