
Abstract
Midfoot osteoarthritis (OA) is a degenerative condition of the foot that can be treated non-operatively by the use of orthotics. This prospective study was conducted to determine the effects of custom-made semi-rigid foot orthoses (FOs) and rigid carbon fibre (CF) footplates for the treatment of midfoot OA evaluated using specifically designed questionnaires. Fifty-seven subjects diagnosed with midfoot OA were recruited through a private clinic for inclusion in the study. Subjects were required to complete pre-treatmentquestionnaires prior to receiving orthotic treatment. All subjects received a pair of custom-made full-length semi-rigid FOs and 36 subjects also received CF footplates that were incorporated into the soles of the shoes worn on the symptomatic feet. Subjects completed post-treatment questionnaires at six weeks, three months and six months after receiving the orthotic treatment. The results demonstrated that there were no significant differences between the results of the subjects who received CF footplates and those who did not. The results of the questionnaires demonstrated that subjects experienced significant improvements in pain, activity levels, walking ability and footwear comfort at all intervals following the orthotic treatment (p <0.01). Subjects' satisfaction with the appearance of their footwear did not decrease with the orthotic treatment despite needing shoes to fit the FOs and CF footplates. The questionnaires also demonstrated that subjects were generally satisfied with the orthotic treatment for the management of their midfoot OA.
Keywords
Introduction
Midfoot osteoarthritis (OA) is a common foot condition encountered in orthopaedic practice 1 involving degenerative changes in the tarsometatarsal joints. 2 Midfoot OA causes symptoms such as pain and discomfort in the early stages with the later stages occasionally resulting in structural changes to the foot such as pes planus and abductus deformities, and the development of prominent osteophytes. 3 The pain caused by midfoot OA varies with the degenerative changes and is commonly identified clinically by focal tenderness and prominent osteophyte formation on the dorsum of the foot. 2 Unfortunately, details regarding the exact course of the degeneration is not well characterized and in need of further study. 4 Inevitably, increased disability caused by midfoot OA leads to decreased activity levels and quality of life. 3
The treatment of midfoot OA can be classified as non-operative and operative. While often effective as a definitive measure, operative intervention in the form of joint arthrodesis is associated with complications such as wound breakdown and infections 5 which can significantly increase the risk of non-union. 6,7 Even after achieving successful union of the symptomatic arthritic joints, increased stresses to surrounding joints can lead to the need for progressively larger fields of surgery. 8
Orthotic treatment is the preferred non-operative method of treatment for midfoot OA to alleviate pain and to provide a form of immobilization to the irritable arthritic joints. 2 The aim of the orthotic treatment is to improve ambulation, activity levels and overall quality of life. 9 Orthotic treatment has the advantage of minimal side effects and low levels of risk. The main disadvantages for the patient are the financial costs (where funding would not be provided by the healthcare system), as well as the necessary compromise on footwear. However, these disadvantages could be overlooked if the orthotic treatment avoided the need for more costly and risky surgery.
Orthotic treatment for midfoot OA usually involves the use of foot orthoses (FOs), supportive accommodative footwear with or without rocker soles, and the addition of full-length carbon fibre (CF) footplates to stiffen the soles of shoes (Figure 1). 3 These treatments work in combination to support and immobilize the arthritic midfoot joints, decrease joint aggravation, decrease inflammation and therefore, decrease pain, ultimately leading to an increase in activity.
There are numerous designs of FOs for the treatment of midfoot OA. The two main designs are the three-quarter-length (3/4) rigid FO and the full-length semi-rigid FO (Figure 2). There is no published literature to demonstrate the most effective design for the mid-to long-term treatment of midfoot OA. There is also limited evidence regarding the use of CF footplates for the treatment of midfoot OA; specifically addressing effects of the footplates when used within the shoe compared to being imbedded into the sole of the shoe (Figure 3). Rao et al. 2 recently conducted a study on the effect of 3/4 rigid FOs compared with CF footplates on midfoot OA and found improvements in pain and activity levels as well as reduced magnitude and duration of loading under the midfoot region with the CF footplates. This study provided evidence that orthotic treatment may be useful for midfoot OA over a four-week period; however, long-term effects remain unknown.

A carbon fibre footplate.

A custom-made full-length semi-rigid foot orthosis.

Cross section of a shoe with a carbon fibre footplate (indicated with an arrow) incorporated into the sole.
Our clinical experience favours the use of custom-made full-length semi-rigid FOs (Figure 2) used in conjunction with CF footplates imbedded into the soles of shoes (Figure 3). Anecdotally, patients tend to find semi-rigid FOs more tolerable and comfortable than rigid FOs due to their increased cushioning and shock absorption capabilities. 10 CF footplates imbedded into the soles of shoes appear to be a more effective method of use, as this does not decrease the amount of room within the shoe (especially if room is required to accommodate the FO). This method also ensures that there is minimal movement between the footplate, shoe and FO, which is important if the aim is to achieve immobilization.
Evidence to support the effects of orthotics for the treatment of midfoot OA is lacking. Literature does not provide clear guidelines regarding orthotic prescription, and the duration of improvement following orthotic treatment is unknown. There has been a considerable amount of research conducted to demonstrate the effectiveness of orthotic treatment for rheumatoid arthritis of the feet, 11–14 but whether these results can be generalized to midfoot OA is uncertain.
The aims of this study were:
To assess the effects of orthotic treatment for midfoot OA through specifically designed patient evaluation questionnaires;
To assess subjects' satisfaction with the orthotic treatment (including service provided and cost to the patient);
To determine if subjects who had previously received orthotic treatment would experience greater relief of their symptoms and improvement with their function following the new orthotic treatment; and
To determine if the radiographic severity of midfoot OA had an effect on the outcome of the orthotic treatment.
Methods
Subjects
Subjects were recruited through a private orthopaedic foot and ankle clinic. All subjects were assessed by a fellowship-trained foot and ankle orthopaedic surgeon. Subjects who were diagnosed with midfoot OA based on clinical and radiographic findings and who satisfied the inclusion criteria were invited to participate in the study. The inclusion criteria were as follows:
Diagnosis of midfoot OA (unilateral or bilateral) and confirmed with radiographic evidence;
Presence of pain in the midfoot region;
A rating of one or greater than one on a midfoot severity scale (Table 1);
Consented to orthotic treatment of the midfoot OA;
Comprehension of English sufficient to understand and complete the evaluation questionnaires; and
Able to give informed consent.
Subjects were excluded if they had any other symptomatic conditions of their feet or ankles unrelated to midfoot OA. Subjects were also excluded if they had previously received the same orthotic treatment as that prescribed in this study - full-length semi-rigid FOs and CF footplates modified into the soles of their footwear.
Evaluation questionnaire
To our knowledge, there is only one midfoot specific evaluation questionnaire detailed in literature known as the AOFAS midfoot score. 15 The AOFAS midfoot score was developed by orthopaedic surgeons for the evaluation of surgical outcomes. As a result, it is not entirely suitable for the evaluation of orthotic treatments as it has low sensitivity to detect change, does not provide sufficient detail regarding variables such as pain and function, and it lacks specificity. Due to these limitations, patient evaluation questionnaires were developed based on the AOFAS midfoot score to provide a means for evaluating the success of orthotic treatment for midfoot OA.
Two questionnaires were developed, one that was used prior to orthotic treatment (Appendix 1, available online at www.informahealthcare.com/doi/suppl/10.3109/03093646.2010.503672) and one that was used after commencing the orthotic treatment (Appendix 2, also available online at www.informahealthcare.com/doi/suppl/10.3109/03093646.2010.503672). The questionnaires were separated into five sections and consisted of 0–10 rating scales, 5-point categorical scales and questions with tick box answers. The first section evaluated pain levels, the second section evaluated activity levels, the third section evaluated perception of footwear and the fourth section evaluated subjects' expectations. The final section detailed any previous orthotic treatment the subject may have received for their midfoot OA apart from full-length semi-rigid FOs and/or CF footplates, which excluded them from the study.
Four-point diagnostic midfoot severity score.

The pre- and post-treatment questionnaires were identical except for the fifth section. The questions regarding previous orthotic treatment were eliminated from the post-treatment questionnaire as it was unnecessary to repeat this information. The post-treatment questionnaire included the addition of two questions regarding subject satisfaction. The questionnaires were designed to be easily comprehensible so that subjects could complete them with minimal assistance.
Procedures
Ethical approval by an ethics committee was not required for this study, however, all subjects were required to give informed consent to be included in the study. Initial consultation by the treating orthopaedic surgeon included both clinical and radiographic assessments. Based on the imaging, a diagnostic midfoot severity score was developed to grade the radiographic severity of the midfoot OA (Table 1). Subjects who were subsequently diagnosed with midfoot OA with a grade greater than or equal to one were presented with the option of managing their condition non-operatively. Subjects were then referred to an orthotist who had a particular expertise in orthotic management of foot and ankle conditions. All subjects were referred for a pair of custom-made full-length semi-rigid FOs and CF footplates for the symptomatic foot/feet.
During the consultation, subjects were fully educated regarding the nature of midfoot OA and the orthotic treatment. Subjects were also educated regarding the appropriate footwear requirements for treatment, which involved extra depth supportive footwear to accommodate the FOs with soles thick enough to accommodate the CF footplates. Once subjects had agreed to try orthotic treatment, they were invited to participate in the research project. After consenting to participate in the study, subjects completed the pre-treatment questionnaire.
Subjects then underwent an assessment of their feet and had impressions taken with compressible foam impression boxes (Gotz Service, Goppingen, 73037, Germany). The impressions were filled with plaster to produce positive moulds that were then modified. A pair of FOs was produced by heat moulding two sheets of high density foam (EVA 220 kg/m 3 first layer and 270 kg/m 3 second layer) over the casts which were then shaped. One week after the consultation, subjects returned to have their FOs custom fitted into their own pre-existing footwear (if appropriate) or footwear recommended by the orthotist.
Subjects who agreed to try the CF footplates had the shoe of their symptomatic foot/feet modified. CF footplate modification involved splitting the sole of the shoe with a sharp knife and grinding a cavity out of the sole that was the shape and depth of the CF footplate. The CF footplate was then glued into the cavity and the base of the sole glued back onto the shoe. This method ensured no movement between the CF footplate and the shoe. The height of the shoe was not affected as a cavity was created within the sole to accommodate the CF footplate. Subjects who did not agree to try the CF footplates were advised to wear their FOs in supportive firm soled shoes.
After receiving the orthotic treatment, subjects attended at least one review consultation with the orthotist and a separate review consultation with the orthopaedic surgeon. Subjects who required further adjustments to their orthotic devices were able to make review consultations with the orthotist as required. Post-treatment evaluation questionnaires were mailed out to subjects at six weeks, three months and six months following the treatment. Subjects were requested to complete the questionnaires and mail them back to the orthotist in reply paid envelopes.
Data analysis
Research data were entered into MD Analyze, a medical outcome patient database (Medtech, Global Ltd, South Melbourne, 3205, Australia) and analysed using SPSS (SPSS Inc, Chicago, IL, USA). Differences across the four time intervals were analysed using a one-way repeated measures analysis of variance (ANOVA). Mauchly's test of sphericity was used to determine whether distributions were normal, and if they were not, a Greenhouse-Geiser adjustment was used. Where the ANOVA were found to be statistically significant, post hoc tests with Bonferroni adjustments were conducted to determine which pair-wise comparisons were different.
Two-way repeated measures ANOVA was used to determine if there were any significant differences between subjects who received the CF footplates compared to those who did not. Group effects were also analysed for subjects with a midfoot severity score of one compared to those with a score of two or three. Data were further analysed to determine if subjects who had previously received orthotic treatment for their midfoot OA differed in their expectation levels and satisfaction levels from subjects who had not received prior treatment.
Differences between pre-treatment and 6 month post-treatment questionnaires for the non-parametric data were analysed using McNemar's test. Statistical significance for all tests was set at α = 0.01.
Results
Seventy-three subjects diagnosed with midfoot OA were recruited over a period of 24 months. Sixteen subjects were excluded from the study as 12 subjects failed to return post-treatment questionnaires and four subjects requested to be withdrawn for personal reasons. Therefore, the data for 57 subjects were included for analysis. The means and standard deviations for the scores on the 0–10 rating scales between the four intervals were used to calculate the power. The standard deviations were quite consistent around 2.2. It was estimated that the sample size of 57 subjects would provide 100% power to be able to detect a change from baseline of at least 2 units on the 0–10 rating scales. As this study was exploratory in nature, no pilot trial was conducted to estimate effect sizes for the calculation of power prior to the commencement of the study.
The subjects consisted of 16 men and 41 women aged between 37 and 81 years (mean age 63.95 years). Fifteen subjects had midfoot OA diagnosed in both feet, 14 had only the right foot affected and 28 had only the left foot affected. The mean midfoot OA severity score was 1.63 (Table 2). All of the subjects were fitted with custom-made FOs and 36 subjects (63%) also had CF footplates modified into their footwear.
Twenty-seven (47%) subjects had previously been managed with FOs for their midfoot OA before attending the orthopaedic surgeon's clinic. Twenty (74%) of those subjects had received their FOs from a podiatrist, five (19%) from an orthotist and two (7%) from other healthcare professionals. Sixteen (59%) of those subjects had been previously treated with 3/4 rigid FOs of which six had the addition of full length soft covers. Fifteen of those 3/4 rigid FOs had been custom-made and two had been prefabricated. Five subjects (19%) had previously had 3/4 semi-rigid EVA FOs, another five (19%) with full-length semi-rigid EVA FOs and one subject had a UCBL FO.
Of the 27 subjects who had previously tried orthotic treatment for their midfoot OA, 25 (93%) indicated that they achieved better results with the new orthotic treatment in their six-month post-treatment questionnaires. Of the 16 subjects who had previously tried 3/4 rigid FOs, 14 subjects (88%) stated that they received better results with the new orthotic treatment.
The ANOVA revealed significant differences between the four questionnaires for worst pain (F = 44.474, df = 3, p = 0.000), average pain (F = 22.491, df = 3, p = 0.000), walking on uneven ground (F = 29.895, df = 2.2, p = 0.000), walking up and down stairs (F = 9.170 df = 2.520, p = 0.000) and footwear comfort (F = 5.170, df = 1.506, p = 0.000) (Table 3). Post hoc tests revealed that the six-week, three-month and six-month questionnaires were all significantly different from the pre-treatment questionnaires (p < 0.01). There were no significant differences between the pre- and post-treatment questionnaires regarding footwear appearance (F = 1.015, df = 1.955, p = 0.364) (Table 3).
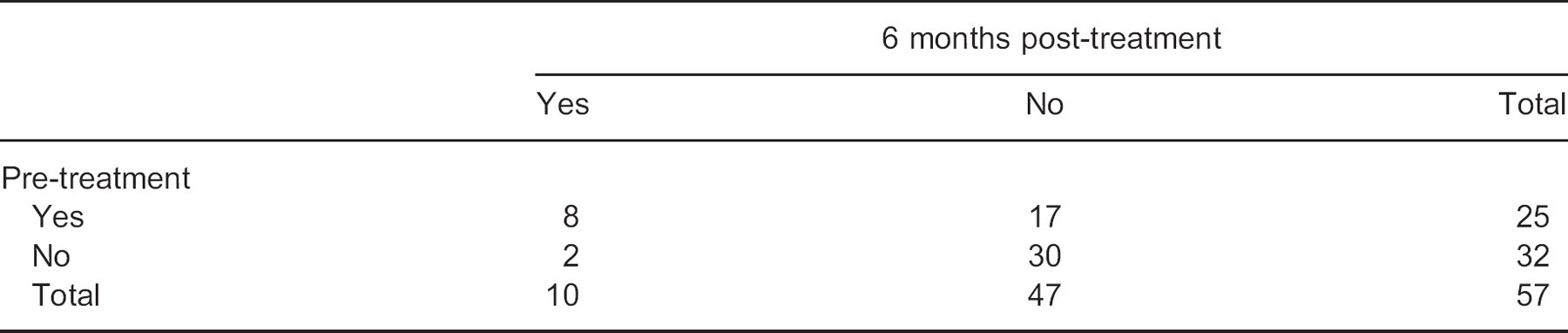
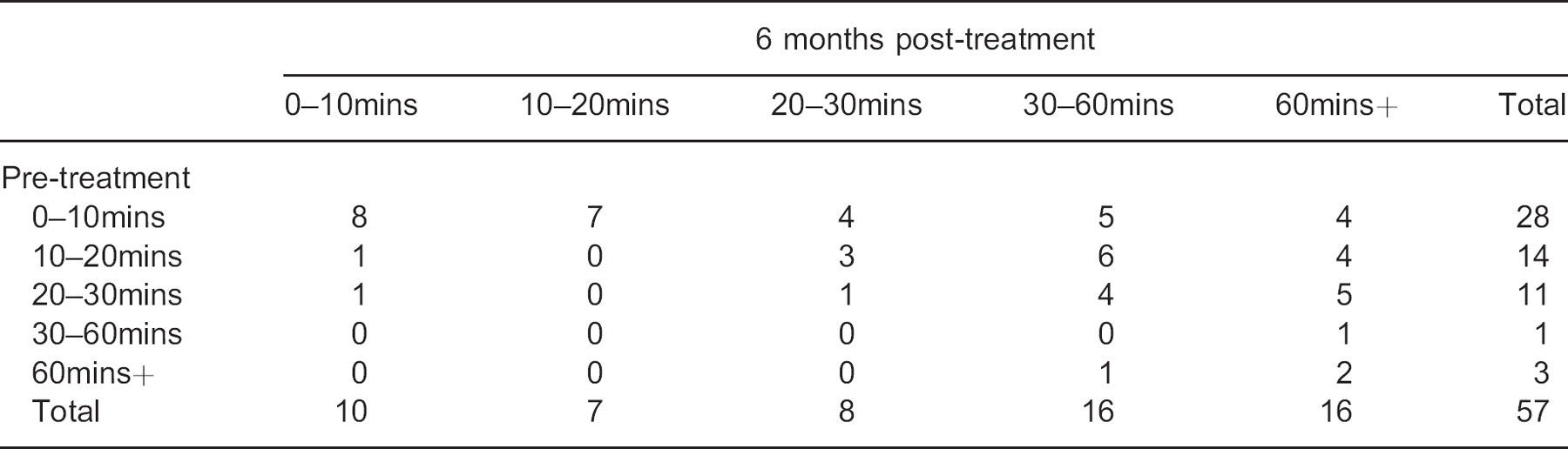
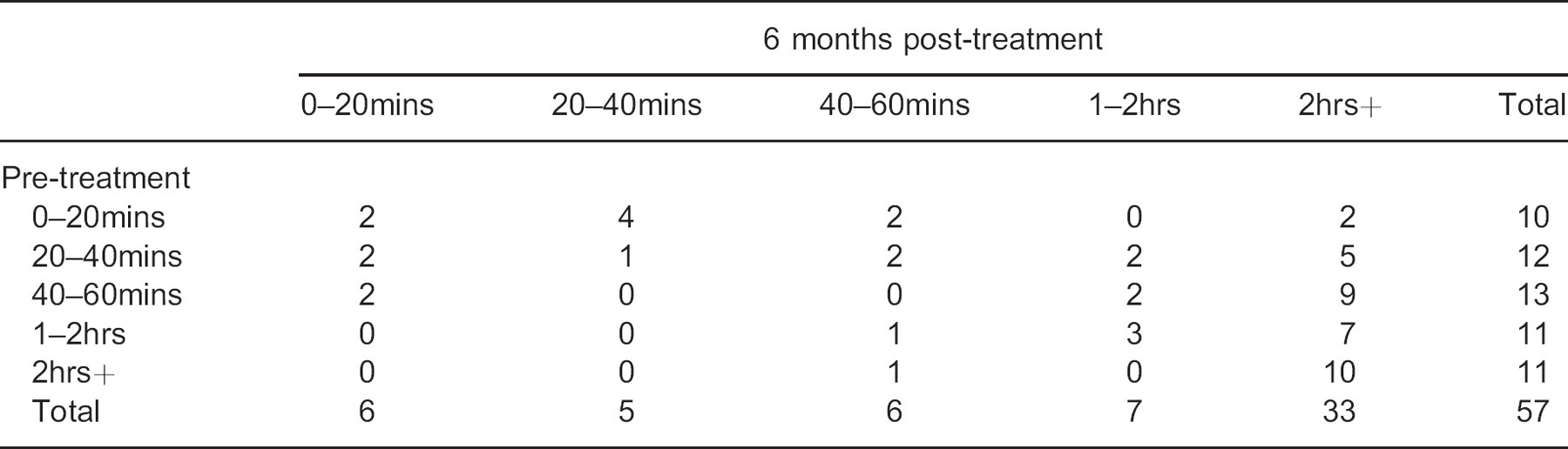
There were significant differences (p = 0.001) between the pre-treatment questionnaires and the six-month post-treatment questionnaires regarding whether subjects reported being woken up by their pain at night (Table 4). There were also significant differences between the pre-treatment questionnaires and the six-month post-treatment questionnaires for the questions regarding how long subjects could walk before their pain began (p = 0.000) (Table 5), and how long subjects could walk before their pain was so severe that they needed to stop walking (p = 0.001) (Table 6).
The results of the two-way ANOVA demonstrated that there were no significant differences in expectation levels, willingness to try orthotic treatment or satisfaction levels with the orthotic treatment between subjects who had previously received orthotic treatment and those who had not. There were also no significant group effects for subjects who were treated with FOs alone and subjects who received the addition of CF footplates. Likewise, there were no significant differences between subjects with a midfoot severity score of one compared with those with scores of two or three.
Distribution of midfoot severity scores.

Average scores for questions with responses rated on a 0–10 rating scales (Mean ± SD).
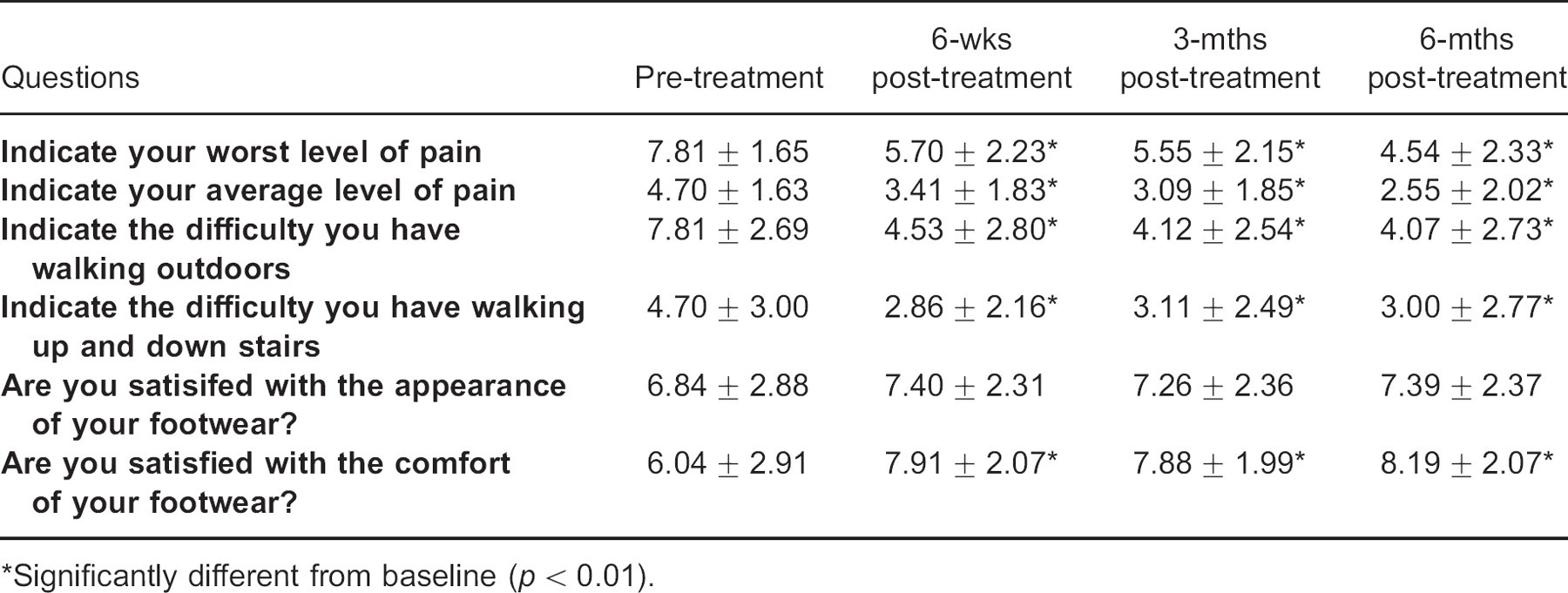
Significantly different from baseline (p < 0.01).
2 × 2 cross table for the responses to the question: ‘Does the pain wake you at night?’.
5 × 5 contingency table for the responses to the question: ‘How long can you walk before the pain begins?’.
5 × 5 contingency table for the responses to the question: ‘How long can you walk before the pain is so severe that you need to stop walking?’.
At six-months post-treatment, the mean score for subjects' satisfaction of the overall treatment process was 8.4 ± 2.0 on the 0–10 rating scale, with 0 being not satisfied and 10 being very satisfied. The mean score for subjects' satisfaction with quality of service received and amount paid was 7.9 ± 2.2 on the same scale. When subjects were asked if they would recommend the treatment to others with their condition, their mean score was 8.5 ± 2.3, with 0 being would not recommend and 10 being would highly recommend.
Discussion
The results of this study demonstrated that orthotic treatment for midfoot OA significantly decreased pain levels, increased activity levels and increased footwear comfort as evaluated with specifically designed questionnaires. Subjects were able to walk longer and with less pain with the use of FOs and for some the addition of CF footplates. Often, there is a compromise in footwear appearance with the use of orthotic treatment; however, subjects' satisfaction with their footwear appearance was not significantly affected after receiving the treatment.
The results also demonstrated that prior orthotic treatment for midfoot OA did not deter subjects from trying another orthotic approach after all subjects received a thorough explanation of the rationale behind the treatment strategy. Furthermore, previous treatment did not have a significant effect on satisfaction outcomes, suggesting that subjects who had previously tried orthotic treatment were not more critical of the treatment process than those who had not received prior treatment.
The results also demonstrated that the majority of subjects who had previously received orthotic treatment for their midfoot OA experienced greater relief with the treatment used in the present study. The type of orthosis subjects had previously received was documented. However, the fit and function of any previous orthoses were not assessed. No subject had previously tried CF footplates.
The subjects who received CF footplates in addition to the FOs did not experience greater relief than those who only received the FOs. This suggests one of two things. Firstly, that the addition of CF footplates was unnecessary and simply wearing appropriate footwear with firm soles was sufficient to experience relief of symptoms, or secondly, that those subjects who received CF footplates were clinically worse and required the added support and immobilization of the CF footplates. However, this is unlikely as the results of the two-way ANOVA revealed no significant differences in outcome between subjects who received CF footplates and those who did not. A randomized controlled trial would be necessary to determine if the use of CF footplates has any additional benefits to firm soled shoes alone.
To our knowledge, Rao et al. 2 are the only other researchers who have assessed the effects of FOs and CF footplates for the treatment of midfoot OA. They reported improvements in the Foot Function Index- Revised scores and reductions in the magnitude and duration of medial midfoot loading with CF footplates compared to 3/4 FOs in subjects with midfoot OA. The authors suggested that CF footplates may be more effective in the treatment of midfoot OA than 3/4 FOs. However, their results seemed biased as the authors noted that subjects reported persistent midfoot complaints with their 3/4 FOs. The subjects were tested using their existing 3/4 FOs that were apparently ineffective and no mention was made of assessing the fit and function of the FOs. The results of the present study demonstrated that the majority of subjects who had previously been provided with 3/4 rigid FOs achieved greater relief with full-length semi-rigid EVA FOs, and it is believed that this was due to the increased cushioning and comfort of the semi-rigid FOs.
Although all subjects were referred for CF footplates, 37% chose not to have them. The main reason for this was that subjects did not want to have the soles of their shoes modified, and fitting the CF footplates inside the shoes was not an option given to subjects for the purposes of this study. Another reason for subjects not wanting the CF footplates was the associated footwear limitation which was a significant factor since the majority of subjects were female. All subjects who did not receive CF footplates were advised to wear their FOs in supportive firm soled shoes.
The additional cost of the CF footplates was also a factor for some subjects deciding not to have them. All subjects were required to fund the full cost of the orthotic treatment themselves. Some subjects were able to claim a reimbursement for a percentage of their costs through external sources such as private health insurance. It was possible that the out-of-pocket cost of the orthotic treatment influenced the results of how satisfied subjects were with the orthotic treatment. It is also possible that subjects' perception of a successful outcome may have been different if the treatments had been provided free of charge.
The primary limitation of this study was that the reliability and validity of the questionnaires was not assessed and this warrants further investigation. The lack of a control group was also a limitation of this study; however, as all subjects had been referred for management by an orthopaedic surgeon in a private clinic, it was deemed unethical to withhold treatment or to use a placebo treatment for any of the subjects. Further investigations into the effects of orthotic treatment for midfoot OA should involve randomized controlled trials to produce higher levels of evidence.
Conclusion
This study has demonstrated that custom-made semi-rigid FOs with and without the addition of CF footplates were effective in decreasing pain and improving activity levels in subjects with midfoot OA over a period of six months. It was also demonstrated that subjects were satisfied with the orthotic treatment of their midfoot OA and would recommend the same treatment to others with their condition. Subjects' satisfaction with the appearance of their footwear did not change significantly following implementation of the treatment indicating that the appearance of shoes required to accommodate orthotic treatment was not a concern for subjects.
Acknowledgements
We would like to acknowledge the Medical Research Foundation for Women and Babies (East Melbourne, Victoria, Australia) for their financial support of this study.
Footnotes
Supplementary material available online