
Abstract
Background:
Floor reaction ankle–foot orthoses are commonly prescribed to improve knee extension of children with cerebral palsy having crouch gait. Their effectiveness is debated. Therefore, the objective of this study is to optimize current prescription criteria for the improvement of crouch gait.
Study design:
Cross-sectional interventional study.
Methods:
A total of 22 patients with bilateral spastic cerebral palsy, between 6 and 17 years, Gross Motor Function Classification System II–IV participated in this study. Instrumented gait analysis was done under three conditions: barefoot, shoed, and with orthotics. Patients were divided into two groups: good and non-responders with more and less than 8.8° improvement of knee extension during walking, respectively. A multiple predictor analysis was done on parameters that were different between groups.
Results:
In total, 12 of 22 patients showed good response in knee extension with a mean change of 17° (standard deviation = 5°). Good responders showed a significantly smaller walking velocity, knee extension strength, ankle plantarflexion strength, and greater external foot progression angle compared to non-responders. Foot progression angle together with ankle plantarflexion strength explained 37% of the variance in improvement of knee extension.
Conclusion:
With appropriate patient selection, an improvement of crouch gait by ankle–foot orthoses of 17° (standard deviation = 5°) can be expected. Patients with slow velocity, weak plantarflexors, and external foot progression benefit most. Joint contractures were no contraindications.
Clinical relevance
This study showed that gait in patients with low functional level benefit most from ankle–foot orthoses. Unlike in patients with higher functional status, contractures of hip, knee, and ankle did not reduce the positive effects on gait. The suggested prescription criteria may help to better select appropriate patients for orthotics.
Background
Crouch gait with excessive knee flexion during the stance phase of walking is one of the most common gait pathologies in children and adolescents with cerebral palsy (CP). 1 Crouch gait increases quadriceps forces that contribute to larger tibiofemoral and patellofemoral loading 2 which may lead to overuse and knee pain. In addition, crouch gait was shown to increase energy consumption. 3 Both pain and increased energy consumption may significantly contribute to activity limitations. 4
Floor reaction ankle–foot orthoses (FRAFOs) with a ventral shell are commonly prescribed to improve crouch gait. They were shown to be effective in controlling tibial advancement over the foot during the second rocker of stance phase, to improve knee extension during walking5–8 and standing. 9 Mechanically, this is achieved by increasing and advancing the floor reaction force vector under the foot. This generates an extension moment at the knee and that has been described as the plantarflexion–knee extension couple. 10
Besides the function to improve crouch gait in stance phase by increased resistance to dorsiflexion, the FRAFO may control the equinus in swing phase by providing increased resistance to plantarflexion. In fact, it has been shown that most patients with CP use FRAFOs successfully for both correcting crouch gait and treat equinus contractures. 11 Limiting plantarflexion in orthotics may reduce plantarflexion work and may affect walking speed and efficiency. 12 However, it was shown in patients with CP that the reduction in plantarflexion of an articulated orthosis did not reduce either walking speed or increased energy consumption. 7 Therefore, indication of FRAFOs to correct crouch gait might be limited not only to patients showing excessive ankle dorsiflexion during walking but also to patients showing equinus pathologies in addition to crouch gait. 11
Reported contraindications for the use of FRAFOs in patients with CP were hip and knee contractures greater than 15°, thigh-foot angles greater than 15° external rotation, and equinoplanovalgus deformities. 6 It was recommended to surgically correct these contractures, segmental malalignments, and deformities before successful application of the orthosis. In particular, CP patients with lower levels of gross motor function are prone to contractures at the hip and knee; 13 however, the use of FRAFOs in these patients group is most frequent. 11 Therefore, the contraindications reported in the literature were not reflected in routine clinical prescriptions. In addition, the reported effects of FRAFOs on peak knee extension during stance phase vary considerably between 3°, 14 5°,7,8 and 11°. 6 These variations suggest that current FRAFO prescription criteria may not be goal directed for the improvement of gait. Hence, the need to develop more effective FRAFO prescription algorithms was emphasized. 15
Therefore, the purpose of the study is to find best predictors from clinical and gait measures for improving crouch gait by FRAFOs. Following a review of the current literature, we hypothesized that patients with lower levels of motor function, excessive dorsiflexion, and weak plantar flexor strength may profit most from the orthoses, whereas excessive rotational leg malalignment, hip and knee contractures may be contraindications.
Methods
Patients
In total, 22 patients with CP volunteered to participate in this cross-sectional interventional study. Patients were children and adolescents presented to the hospital-based outpatient clinics in 2014 and 2015. The children, adolescents, and parents were informed about the study, and the parents provided written consent as approved by the local ethic committee.
Inclusion criteria were as follows: diagnoses of bilateral CP, between 6 and 17 years, Gross Motor Function Classification System (GMFCS) II–IV, and no surgeries in the last 2 years. Patients must have crouch gait without orthotics and were provided bilaterally with customized hinged FRAFOs with a rigid ventral shaft to improve crouch gait. Patients must have used their orthotics for a minimum of 3 months. A total of 22 age- and gender-matched typically developed children and adolescents were used as reference group.
Orthotics
Participants were prescribed with a custom-fabricated FRAFO which was manufactured by Pohlig GmbH, Traunstein, Germany.
The shape of the orthosis was gathered by a three-dimensional (3D) scan (EVA, Artec 3D, Luxembourg City, Luxembourg) with the subtalar joint and ankle joint held in neutral position. The 3D scan was then filled, smoothed, and edited using a computer-aided design (CAD) program. The resulting design data were transferred to the manufacturing center where the positive model was carved from a block of hard foam using the computer-aided manufacturing (CAM) method. The foam liner was build first and then a carbon fiber composite was vacuum laminated. The number of layers, in particular for the stiff footplate, was adapted to the patient’s weight. An ankle joint (F1734; Otto Bock Holding, Duderstadt, Germany) was fixed, and then upper and lower parts were separated, so that the shank was supported by a rigid ventral shaft, and the foot was held by a circular hindfoot fixation with a rear opening shown in Figure 1.

FRAFOs used in this study frontal, lateral, and medial view.
In the final adjustment, the range of motion in the ankle joint was decided depending on the foot and ankle pathology. In case of spastic equinus, the plantarflexion was locked and the dorsal-extension was released to 5°. In case of talipes calcaneovalgus, the dorsiflexion was locked and the plantarflexion was released to maximally 10°. In combination with the orthotic shoe, the heel height was then adjusted to obtain a heel toe gait with a plantar foot contact during midstance phase of walking. In addition, it was aimed for a 12° inclined shank angle with the floor that was shown to result in a stable physiological walking pattern. 16
The specification, 3D scan, and final fitting were completed by two experienced certified orthotists in the outpatient department.
Data collection
Kinematic data were collected using the Vicon Plug-in-Gait marker set on an 8-cameraVicon system (Vicon, Oxford, UK). In addition, medial ankle and knee markers were used during the standing trial to improve the accuracy of the joint rotations in the transverse plane. 17 Wearing orthotics, the ankle markers were palpated on the hinge axes of the orthoses. Patients walked under three conditions: barefoot, shoed, and FRAFOs with orthotic shoes at preferred walking speeds in randomized order. If necessary, patients used their walking aid that they most frequently used for ambulation for all three conditions. Subsequent to gait analysis, participants underwent a standardized manual clinical examination including goniometric measurement of passive hip, knee, and ankle range of motion as well as manual muscle strength testing of the lower leg muscles. The detailed clinical test protocol with subjects and goniometric positioning was previously published. 18
Data evaluation and statistics
A prior definition of good responders (GR)/non-responders (NR) was established: For the orthotic intervention, an improvement of 8.8° in peak knee extension during stance phase of walking, compared to the shoed condition was considered a GR. This threshold of 8.8° represents two standard deviations (SDs) of the peak knee extension angles of the typically developed controls. This was chosen because crouch gait is defined as knee extension angles greater than 2 SDs above the average control value. 19 Therefore, this value provides a considerable improvement of knee extension from being classified as mild crouch gait to natural knee gait of typically developed controls.
The investigated parameters of clinical examination and gait analysis are listed in Tables 1 and 2, respectively. The differences for clinical parameters between both groups GR and NR were tested using independent t-tests with a significance level of p < 0.05. Differences between gait parameters were tested with a two-factor mixed-model analysis of variance (ANOVA) with group (GR and NR) and repeated measures in intervention (barefoot, shoes, and orthoses). To account for multiple parameters (12) tested on the same gait data set, the significance level was Bonferroni corrected to p < 0.004. Post hoc t-tests were performed to locate significant differences.
Anthropometrics, previous surgeries, clinical strength, and passive range of motion measures of good and non-responders to orthosis compared to typically developed (TD) controls.
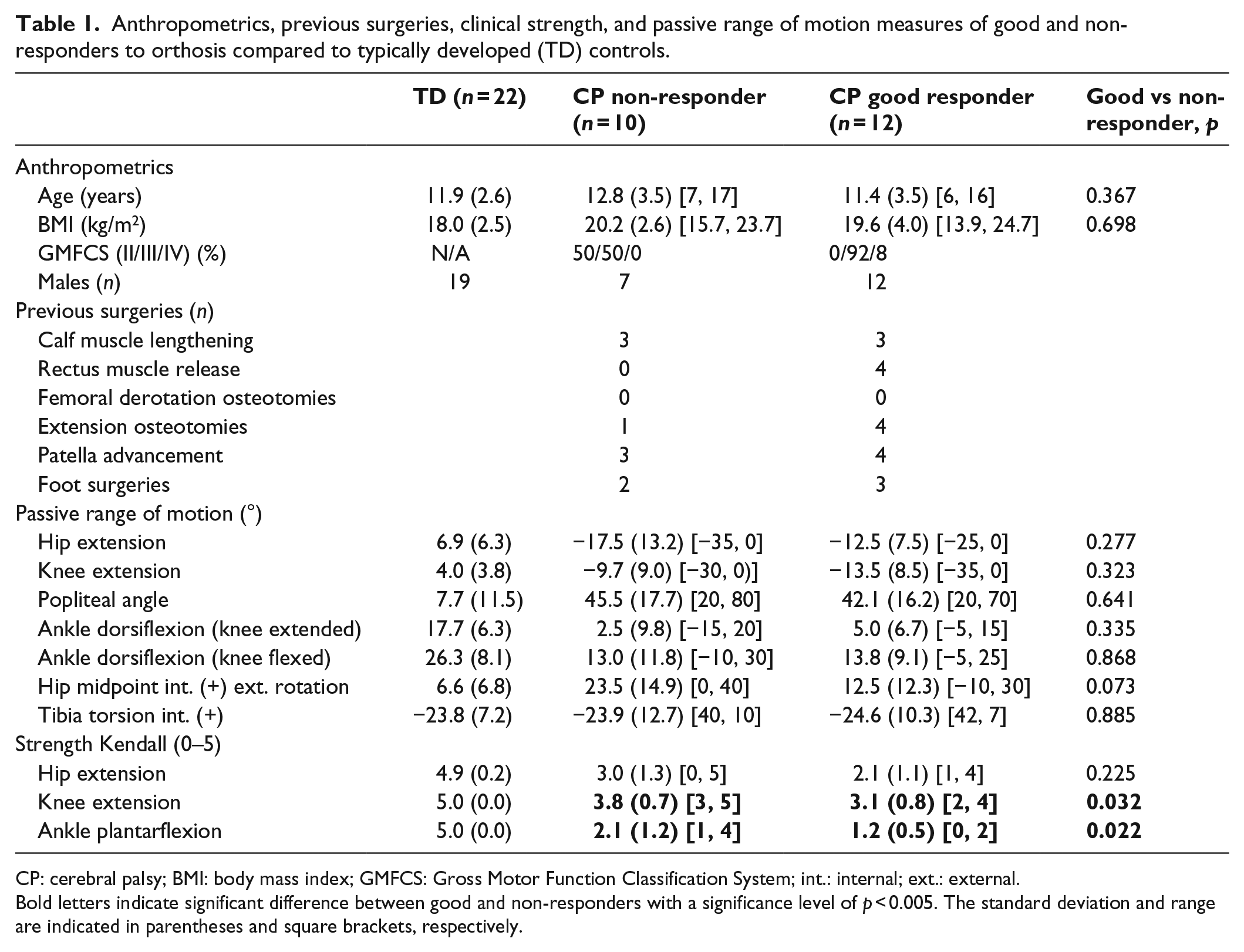
CP: cerebral palsy; BMI: body mass index; GMFCS: Gross Motor Function Classification System; int.: internal; ext.: external.
Bold letters indicate significant difference between good and non-responders with a significance level of p < 0.005. The standard deviation and range are indicated in parentheses and square brackets, respectively.
Gait analysis data of good responders (GR) and non-responders (NR) of walking barefoot, shoes, and with orthoses compared to TD children and adolescents walking barefoot.
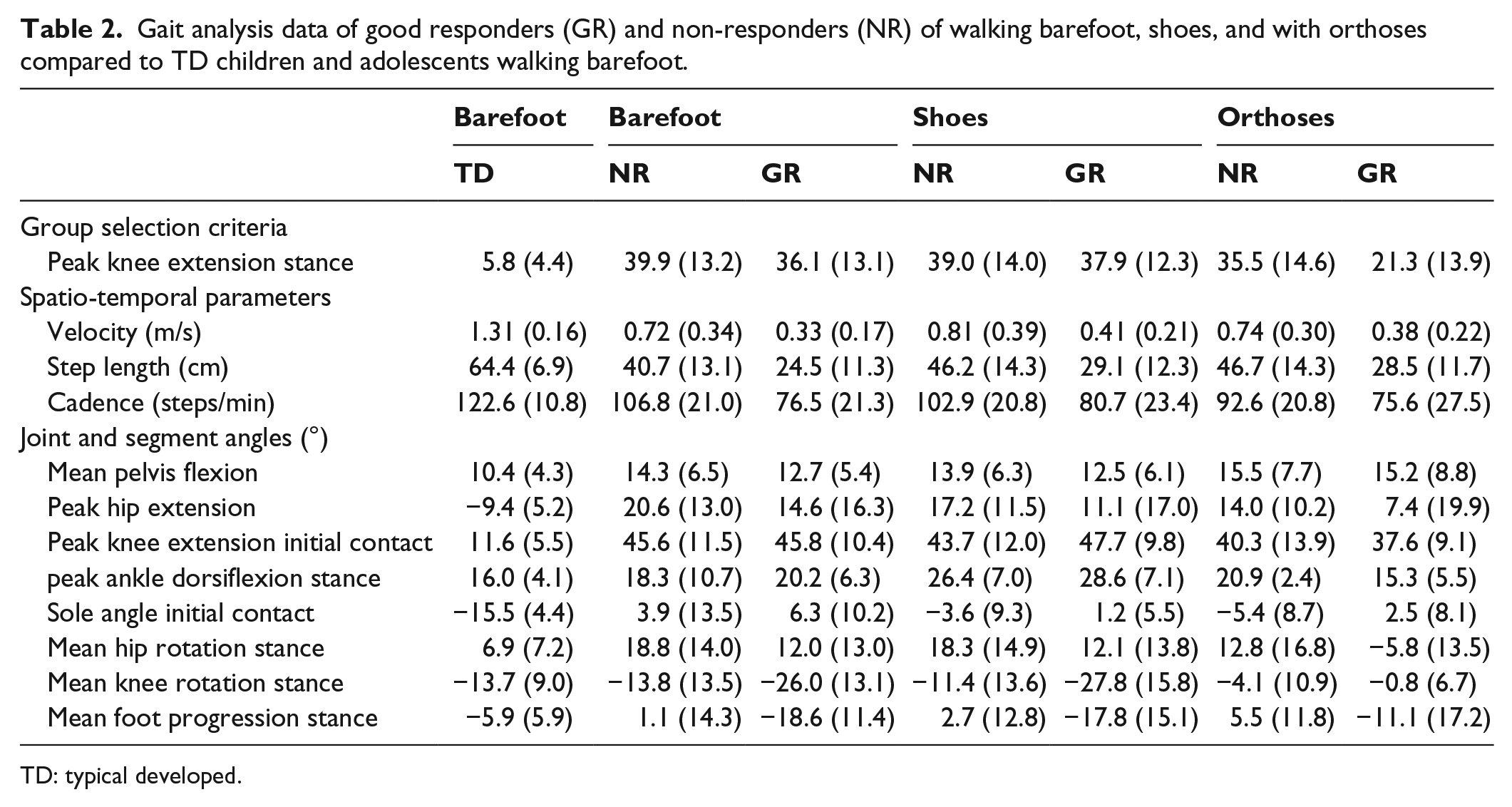
TD: typical developed.
For parameters that were significantly different between groups GR and NR in the clinical tests and barefoot walking conditions, a stepwise multilinear regression of the response value (improvement in knee extension during walking) was performed. Intercorrelations and Henze–Zirkler’s multivariate normality test were used to assess the requirements for the multiple regression analysis. 20 The calculation was carried out using the function “stepwisefit” of the MATLAB 6.2 statistics toolbox (The Mathworks, Inc., Natick, MA, USA). The maximum p value for a term to be added was p = 0.05. The minimum p value for a term to be removed was p = 0.10.
Most children with bilateral involvement display asymmetric neurological involvement, gait and musculoskeletal pathology. This results in complex interactions between both limbs so that they cannot be evaluated independently. 21 We assume that the leg with the larger crouch gait (peak knee extension in stance) is mainly responsible for the crouched gait and will be analyzed and presented in detail. In addition, the predictor analysis was presented for both legs to support the previous assumption.
Results
In total, 12 of 22 patients (55%) showed good response, greater than 8.8° in knee extension with ankle–foot orthosis (AFO) compared to the shoed condition. The improvement varied between 10° and 28° with a mean of 17° (SD = 5°). The 10 of 22 non-responders showed between −4° and 8° changes in knee extension with a mean of 4° (SD = 5°). Anthropometries, previous surgeries, clinical tested strength, and passive range of motion of GR and NR groups are shown in Table 1. The five patients with higher functional level GMFCS II were all located in the NR group. Previous surgeries were not considerably different between both groups. Significant differences between NR and GR were observed for knee extension strength (p = 0.032) and ankle plantarflexion strength (p = 0.022). Results of the gait analysis are shown in Figure 2, Table 2, and the associated statistics in Table 3. Significant differences were found for walking speed (p = 0.002) and foot progression angle (p = 0.002). The barefoot walking speed of GR was on average reduced about 0.4 m/s, and the foot progression angles on average more outward rotated about 17° compared to the NR group. Four parameters were significantly different between NR and GR groups in the clinical test and barefoot walking condition: (1) knee extension strength, (2) ankle plantarflexion strength, (3) walking velocity, and (4) foot progression angle.
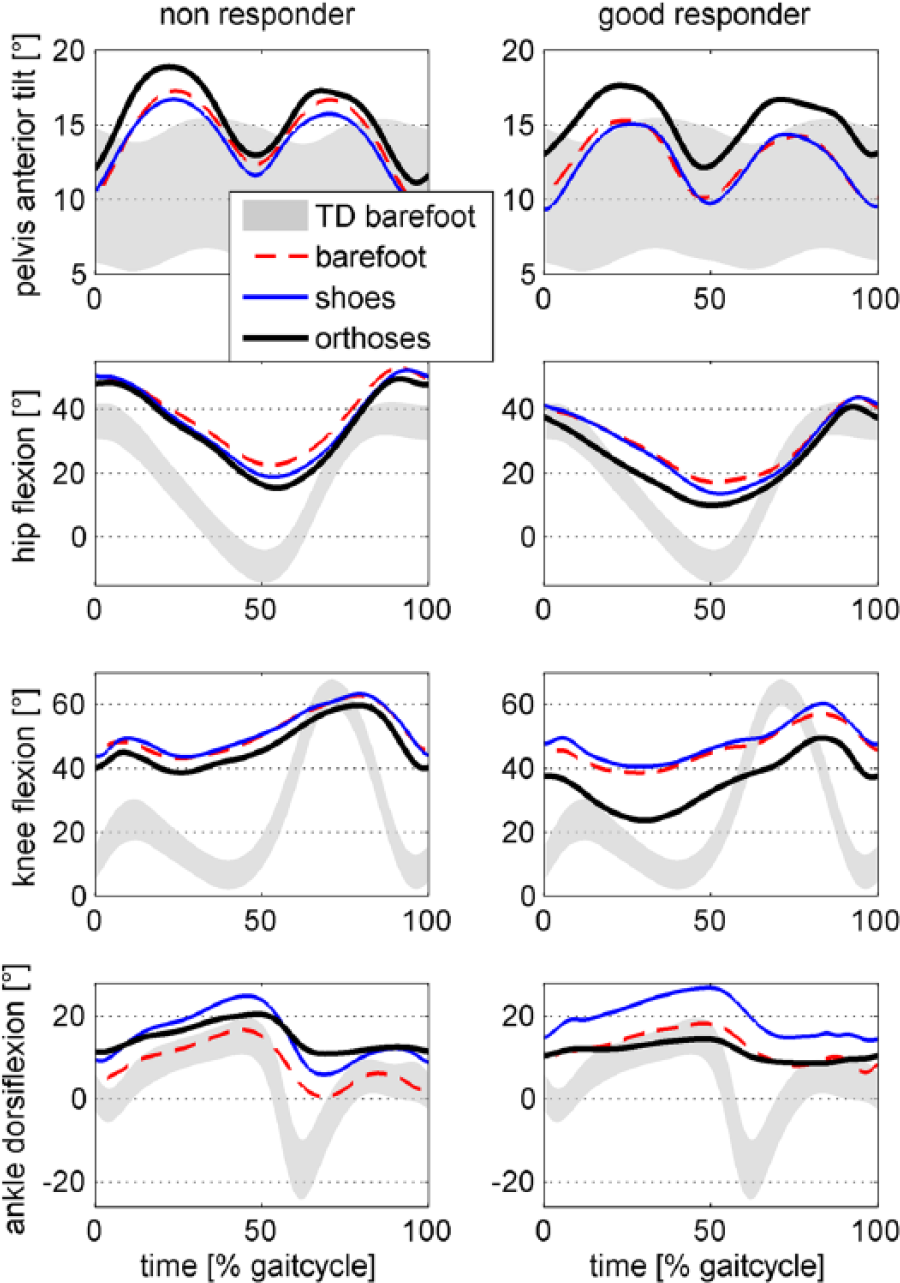
Joint and segment angles of patients in the sagittal plane under three conditions: barefoot, shoes, and shoes with orthoses in comparison to typical developed participants.
Gait analysis ANOVA table between groups of good responders (GR) and non-responders (NR) walking under three conditions (barefoot, shoed, and with orthoses).
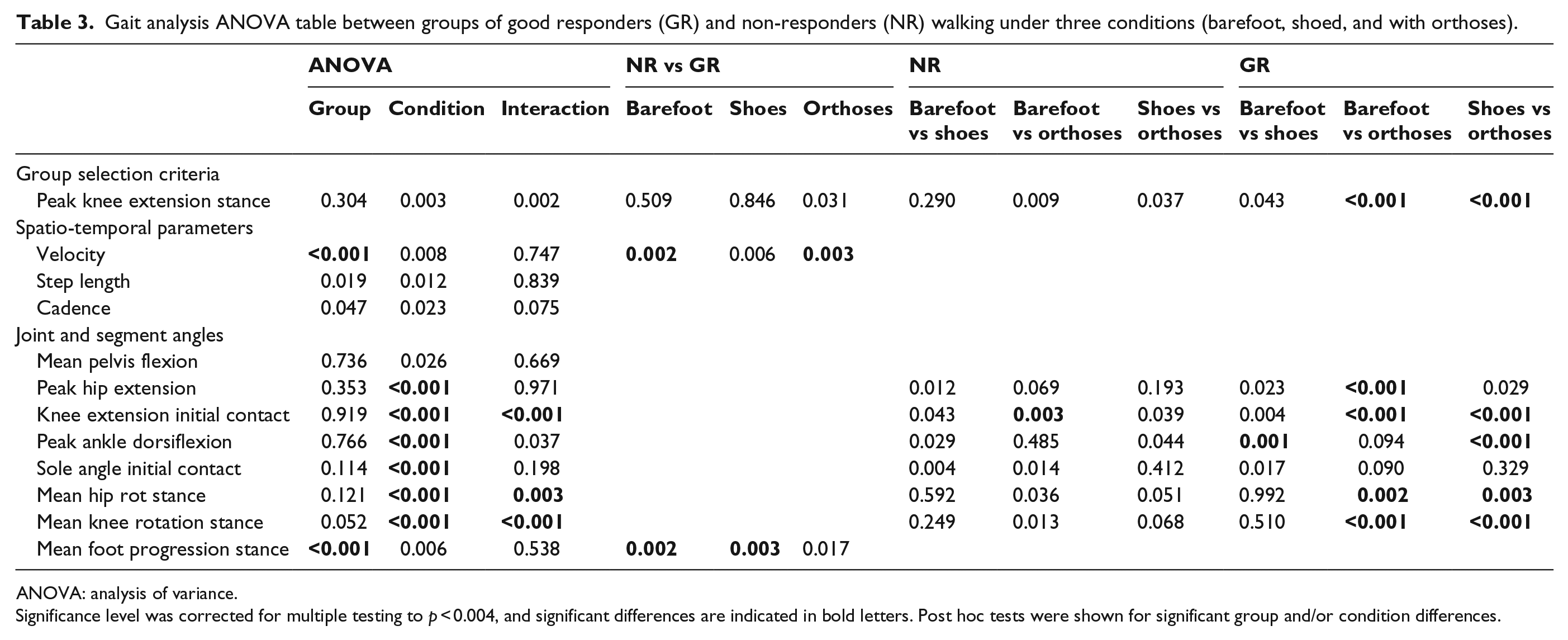
ANOVA: analysis of variance.
Significance level was corrected for multiple testing to p < 0.004, and significant differences are indicated in bold letters. Post hoc tests were shown for significant group and/or condition differences.
Predictor analysis
The individual correlation with the improvement in knee extension, of the four parameters mentioned above, was for knee extension strength (R = −0.28, p = 0.20), ankle plantarflexion strength (R = −0.4, p = 0.049), walking velocity (R = −0.60, p = 0.003), and foot progression angle (R = 0.54, p = 0.012). All four parameters may be used as potential predictors. However, significant intercorrelations (p < 0.05, R > 0.50) between the four parameters were found: knee extension strength correlates with ankle plantarflexion strength and the velocity correlates with foot progression and knee extension and ankle plantarflexion strength. For the multiple predictor analysis, foot progression and ankle plantarflexion strength were selected as independent predictors, as they were found to be related to the correction mechanism of the orthoses. Stepwise multiple predictor analysis revealed foot progression as the best predictor explaining 29% of the variation of improvement in knee extension; both parameters together explained 37% of the variation.
Contralateral side
The same 12 of 22 patients showed good response in knee extension also on the side showing less crouch gait during barefoot walking. The improvement was between 9° and 39° with a similar mean value of 17° (SD = 9°) as the side with more crouch gait. Except for knee extension strength, the same three parameters were also significantly different between GR and NR groups. The intercorrelations among these three parameters showed the same results with slightly lower correlation coefficients (p < 0.05, R > 0.43). The results of the predictor analysis are shown in Table 4. Compared to the more crouched side, the order of the prediction was reversed with ankle dorsiflexion strength being the best predictor. Since both sides showed similar outcome, both legs were pooled together, revealing foot progression as the best predictor with slightly decreased predictive value compared to the more crouched side only.
Stepwise included best models for predicting improvement in knee extension by AFO.
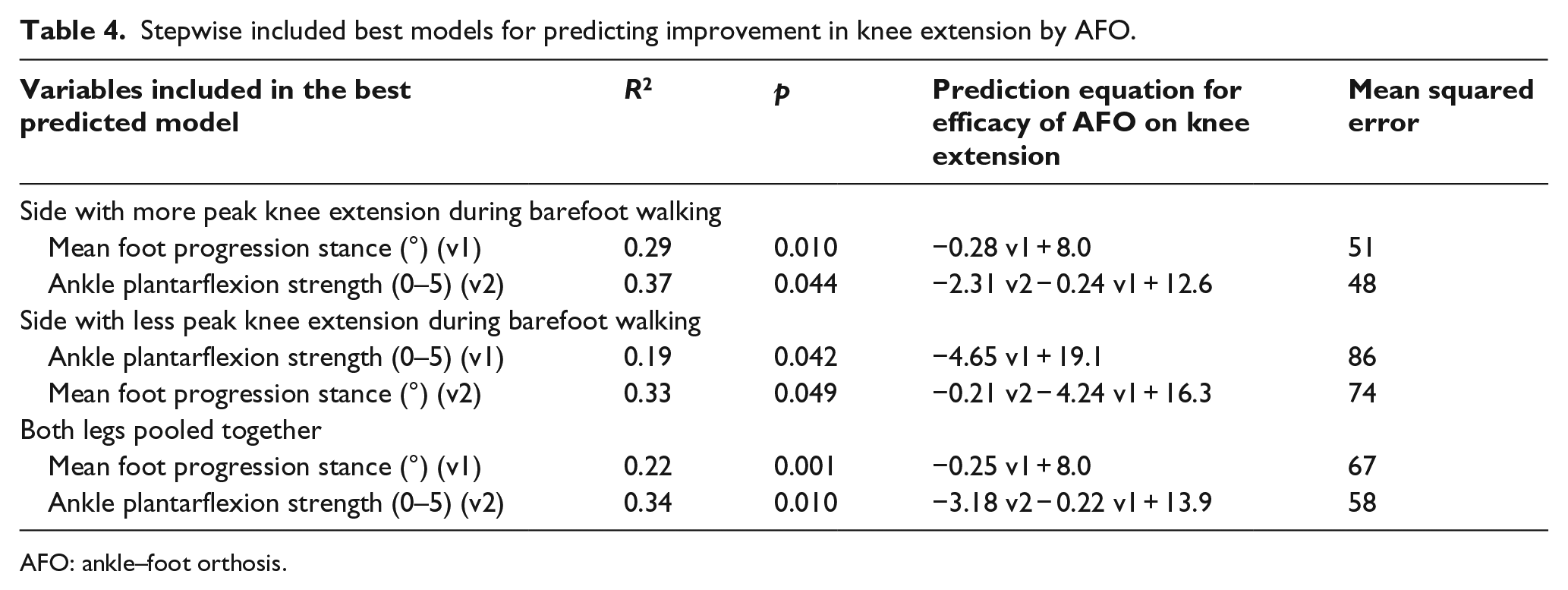
AFO: ankle–foot orthosis.
Discussion
With the appropriate patient selection, an improvement of crouch gait by FRAFOs between 10° and 28° can be expected. In agreement with the hypotheses, patients with a low functional status (GMFCS III and IV) profited most from the orthoses. These GR were characterized by a slow walking speed, weak knee extensors, and ankle plantarflexors.
In disagreement with the hypotheses, knee, hip, and ankle contractures or rotational malalignments were no contraindications. On the contrary, excessive foot external progression angle was the best predictor for improvement of knee extension. Foot progression angle together with weak ankle plantarflexion strength explained 37% of the variance in improvement of knee extension during walking.
The average effects of FRAFOs on improvement in peak knee extension during stance phase reported in the literature were 3°, 14 5°,7,8 and 11° 6 and therefore considerably lower than 17° (SD = 5°) reported in this study. One explanation may be the higher functional status of their patients, demonstrated by walking speeds in FRAFOs of 1.06 m/s, 14 1.07 m/s, 7 and 0.83 m/s 6 that were considerably higher than 0.38 m/s for the GR in this study. Sorting all studies with respect to the effect in knee extension, a linear decrease in the corresponding walking speed can be noticed. This further supports the hypothesis that patients with lower functional status mostly improve gait when using FRAFOs. 11
Contrary to the study of Rogozinski et al., 6 that reported no effects of FRAFOs on gait for knee and hip contractures greater than 15°, considerable flexion contractures of up to 25° in the hip, and 35° in the knee, were observed for the GR in this study. Possible reasons may be that barefoot peak knee extension during walking in the study of Rogozinski et al. 6 was with an average of 29° (SD = 14°) considerably lower than 40° (SD = 13°) in this study. Consequently, in the study of Rogozinski et al., 6 25% of legs reached the knee extension using FRAFOs within 1 SD of typically developed controls, whereas in this study, it were only 14%. Therefore, in this study, the gain in knee extension may not have interfered with the range of knee contractures. Regarding ankle contractures, there was no significant difference in passive ankle dorsiflexion or peak ankle dorsiflexion during walking between GR and NR groups, suggesting that ankle pathology is of minor importance. A notable difference in ankle dorsiflexion about 15° between the passive clinical test and gait analysis in patients, but not in controls, indicates that excessive midfoot bending during walking may contribute to the calculation of ankle dorsiflexion using the Plug-in Gait model. 22 Excessive midfoot bending is typically associated with a planovalgus foot deformity that is frequently observed in CP patients. 23 This combination of heel equinus, talonavicular subluxation, midfoot break, and external tibial torsion also contributes to crouch gait as part of lever arm dysfunction. 23 The use of FRAFOs may increase and stabilize the lever arm of the foot to provide a rigid lever that is required for an effective plantarflexion–knee extension couple. The stable base of support may be particularly important for patients with low-level motor function who have less abilities to compensate their distal lever arm dysfunction using their proximal muscles.
The rotational malalignment in knee rotation (rotation of the femoral axis with respect to the malleolar axis) and foot progression was particular high in the GR group. In the NR group, the foot is pointing 1.1° internal and in GR, 18.6° external to the walking direction. The reason for the external foot progression angle was mainly due to an increased external knee rotation angle during walking, which showed a trend to significance (p = 0.052) between GR and NR groups. The AFO corrects the foot progression angle internally in both groups about 4° that was consistent to the reports in the literature 24 and may reflect the correction of foot abduction. Most of the changes in hip and knee rotation occurred in the GR group. However, these changes must be treated with caution since markers were placed on the ankle hinge centers of the FRAFO and may not reflect the anatomical rotation of the leg within the orthotics. Nevertheless, realigning the axes was leading to a good response of FRAFOs when there was an excessive external foot progression observed.
According to the best practice reporting guidelines, 25 the comparison of the effect of FRAFOs was done between the shoed conditions (not barefoot) to avoid attributing the effects of footwear to the FRAFOs. Whether the FRAFO condition was compared to the shoed or barefoot condition, the results were similar, except for the change in ankle dorsiflexion. In the shoed condition, the ankle peak dorsiflexion showed a shift about 10° more dorsiflexion in both groups. The reason may be due to equinus deformity and toe gait, in which the heel cannot be fixed in the commercially available shoes of the patients. Furthermore, one may expect a higher walking speed in shoes or FRAFOs. However, the differences between the three conditions were not statistically significant. In conclusion, gait analysis typically done under barefoot conditions would be sufficient to evaluate the effect of orthotics in this study. Shoed condition may even lead to misinterpretation through movement of the foot within the shoe.
There may be three limitations in this study. First, kinetic information could not be presented. Second, the shoes were no orthotic shoes, and third, the FRAFO construction was different to those used in other studies.6–8,14 The first limitation is due to the functional status that 17 of 22 patients have to use walking aids such as walkers, crutches, or sticks for ambulation where joint moments cannot be determined. However, for patients with lower level of ambulation, FRAFOs were most effective so that investigations are most relevant for this group. The second limitation was that the shoed condition was measured using their own commercially available shoes, that patients used when wearing no orthotics. This is difficult to compare with orthotic footwear that was combined with the FRAFOs because it was too wide to be worn without orthotics. Therefore, specific orthotic footwear with a stable sole and shaft may have more effect on walking speed. However, the effect on knee extension would likely be the same, and it is most relevant since patients use these shoes when wearing no orthotics. The third limitation was that the orthoses were different to those used in the literature. They were a customized two-piece solid-hinged FRAFO with a ventral shell and a circular locking for the hindfoot. Compared to full thermoplastic constructions used in other studies, they were individually fabricated to provide best fit for stabilizing the foot and ankle in its physiological position. The well-defined hinge ankle joint axis may be superior in realigning the transverse plane axes, and the fixation by a circular foot locking construction may provide a better fixation of the hindfoot within the orthotics. Both, the different orthotic construction and the lower functional status of patients, may explain the superior effects in knee extension observed in this study.
Conclusion
With appropriate patient selection, a mean improvement of crouch gait with FRAFOs of 17° (SD = 5°) can be expected. Patients with low functional status (GMFCS III and IV), weak plantarflexion strength, and external foot progression profit most. Contractures of hip, knee, and ankle were no contraindications.
Although orthoses showed considerable effects on knee extension, the reference value of typical developed controls was only achieved in 14% of legs.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.