
Abstract
The benefits of physical activity on mental well-being, as well as physical well-being, are widely recognized although mechanisms remain unclear. Research with clinical populations has shown that physical activity is effective in alleviating depression and anxiety [1,2]. The inverse relationship between regular physical activity and depression [3–9] and the recognition of physical inactivity as a risk factor for depression [10] support the notion of a protective nature of the relationship between physical activity and mood. Physical activity programmes have also been shown to have beneficial effects on positive emotion [11–13], which independently promotes good physical health [14]. Physical activity may additionally decrease the risk of developing depression [9,15].
Negative affect includes feelings that reflect unpleasant engagement, such as distress, anger, disgust, fear and shame [14,16,17]. By contrast, positive affect embraces pleasurable feelings and includes happiness, interest, joy, excitement, enthusiasm, contentment and alertness. It is unclear whether these two elements are polar extremes on the same scale, or whether they represent separate orthogonal factors [14]. This is of relevance as there is a large literature of the relation of negative affect to various disorders, including mental health. In particular, if the two constructs exist on a continuum, the benefits of positive affect may reflect absence of negative affect. However, if they are independent, positive affect could provide therapeutic benefits that are independent of negative affect.
The mood literature has tended to focus on depression as a unitary phenomenon; however, there are increasing data suggesting that positive and negative affect are independent, albeit related, constructs. The school of positive psychology has developed around the modulation of positive affect as a means of preventing depression [18]. However, while there is a theoretical basis for research underpinning positive psychology, it remains unclear if mood-modulating strategies operate via positive or negative affect, or have non-specific effects on both. We therefore aimed to examine the association between habitual physical activity, and both positive and negative affect.
Methods
Subjects
This analysis was conducted as part of the Geelong Osteoporosis Study (GOS), a study originally designed to investigate the epidemiology of osteoporosis in Australia but later expanded to study mental health. A cohort of 1494 women was selected at random from electoral rolls for the Barwon Statistical Division in south-eastern Australia, and enrolled in the GOS in the period 1994–1997, with a response of 77.1% [19]. This analysis focuses on the 304 women who completed questionnaires as part of their 8 year follow up assessment. Twenty-eight women were excluded because their questionnaire data pertaining to affect were incomplete; thus, data for 276 women were included. The Barwon Health Human Research Ethics Committee approved the study and all participants provided informed, written consent. Participant anonymity has been preserved in this report.
Data
Data collected at the 8 year assessment were used to investigate cross-sectional associations between habitual physical activity and self-rated affect. Self-rated affect was derived from two 10 item scales that comprise the Positive and Negative Affect Schedule (PANAS) that recorded feelings and emotions over the few days prior to assessment [17]. The exposure of interest was habitual physical activity level categorized as ‘very active’ if the subject ‘moves, walks and works energetically; participates in vigorous exercise’; ‘moderately active’ if the subject ‘walks at brisk pace, does normal housework or other work; engages in light exercise’; otherwise they were described as ‘sedentary’. Body weight and height were measured and body mass index (BMI) calculated as weight/height2 (kg/m2) and categorized as normal if BMI < 25.0 kg/m2, overweight if BMI was in the range 25.0–29.9 kg/m2, and obese if BMI > 30.0 kg/m2 [20]. Tobacco smoking was recognized if smoking was practised regularly at the time of assessment; exposure to medications and diseases were self-reported; alcohol consumption was estimated (as average grams of ethanol per day) from a food frequency questionnaire [21] designed and validated by the Cancer Council of Australia (Victoria) [22]. Self-reported current use of prescription medications was recorded and classified as up to two, and three or more. Socioeconomic status (SES) was ascertained using the Socio-Economic Index for Areas (SEIFA) values based on 2001 census data from the Australian Bureau of Statistics. SEIFA values were used to derive an Index of Occupation and Education (IOE), which was categorized into quintiles according to cut-points for the Barwon Statistical Division.
Statistics
Characteristics for women categorized by level of physical activity were compared using analysis of variance (ANOVA) for parametric continuous variables, Kruskall-Wallis for non-parametric continuous variables, and the χ2 test for discrete variables. Odds ratios (OR), with 95% confidence intervals (CI), were determined using logistic regression models to investigate associations between physical activity (the exposure of interest expressed as very active, moderately active and sedentary) and the likelihood of having a high positive or negative affect score (highest tertile compared to mid and low tertiles combined). Age, body composition, smoking, alcohol use, SES and exposure to medications were investigated as confounders and effect modifiers. Statistical analyses were performed using STATA (release 9.0, StataCorp, College Station, TX) and MINITAB (version 15, State College, PA).
Results
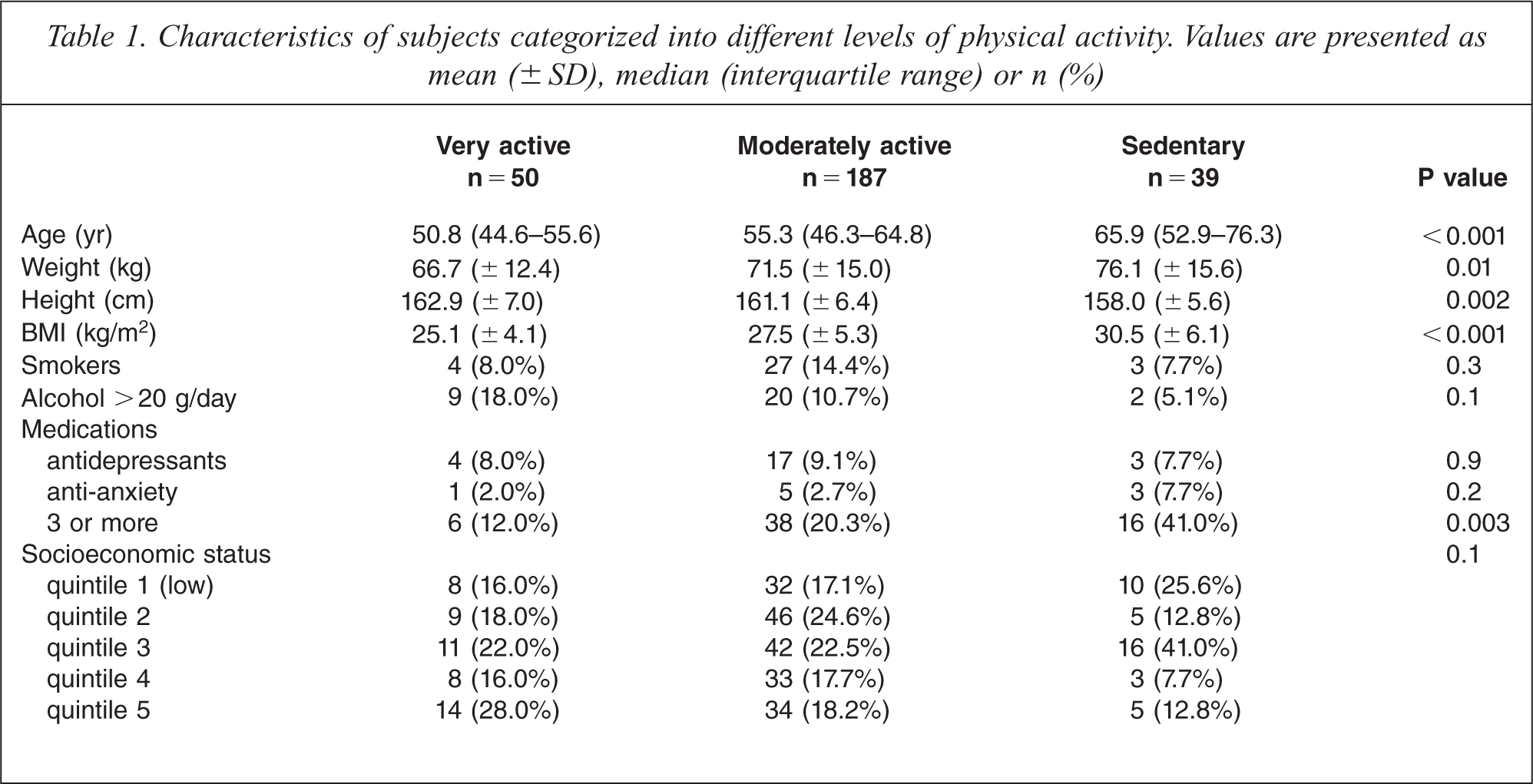
Among the 276 subjects, 50 (18.1%) were classified as very active, 187 (67.8%) as moderately active and 39 (14.1%) as sedentary (Table 1). Women in the very active group were the youngest, they had the lowest body mass index and fewer used 3 + prescription medications. No differences were detected for other lifestyle exposures. There was a pattern of lower positive affect scores for lower levels of physical activity (p = 0.001, Figure 1). With the very active group set as the reference, the odds for having a high positive affect score was sequentially reduced for those who were moderately active (OR = 0.53, 95%CI 0.28–1.01, p = 0.05) and sedentary (OR = 0.28, 95%CI 0.10–0.75, p = 0.01). These associations were sustained after adjusting for the confounding variables, body mass index and use of 3 + prescription medications: OR = 0.50 (95%CI 0.26–0.96), p = 0.04; and OR = 0.25 (95%CI 0.09–0.72), p = 0.01, respectively (Figure 2). This association was not explained by differences in age, negative affect score or any of the other lifestyle exposures listed in Table 1. There was no association detected between physical activity and negative affect scores. With the very active group set as the reference, the adjusted odds for having a high negative affect score did not differ for those who were moderately active (OR = 0.67, 95%CI 0.34–1.31, p = 0.2) or sedentary (OR = 1.14, 95%CI 0.46–2.85, p = 0.8).
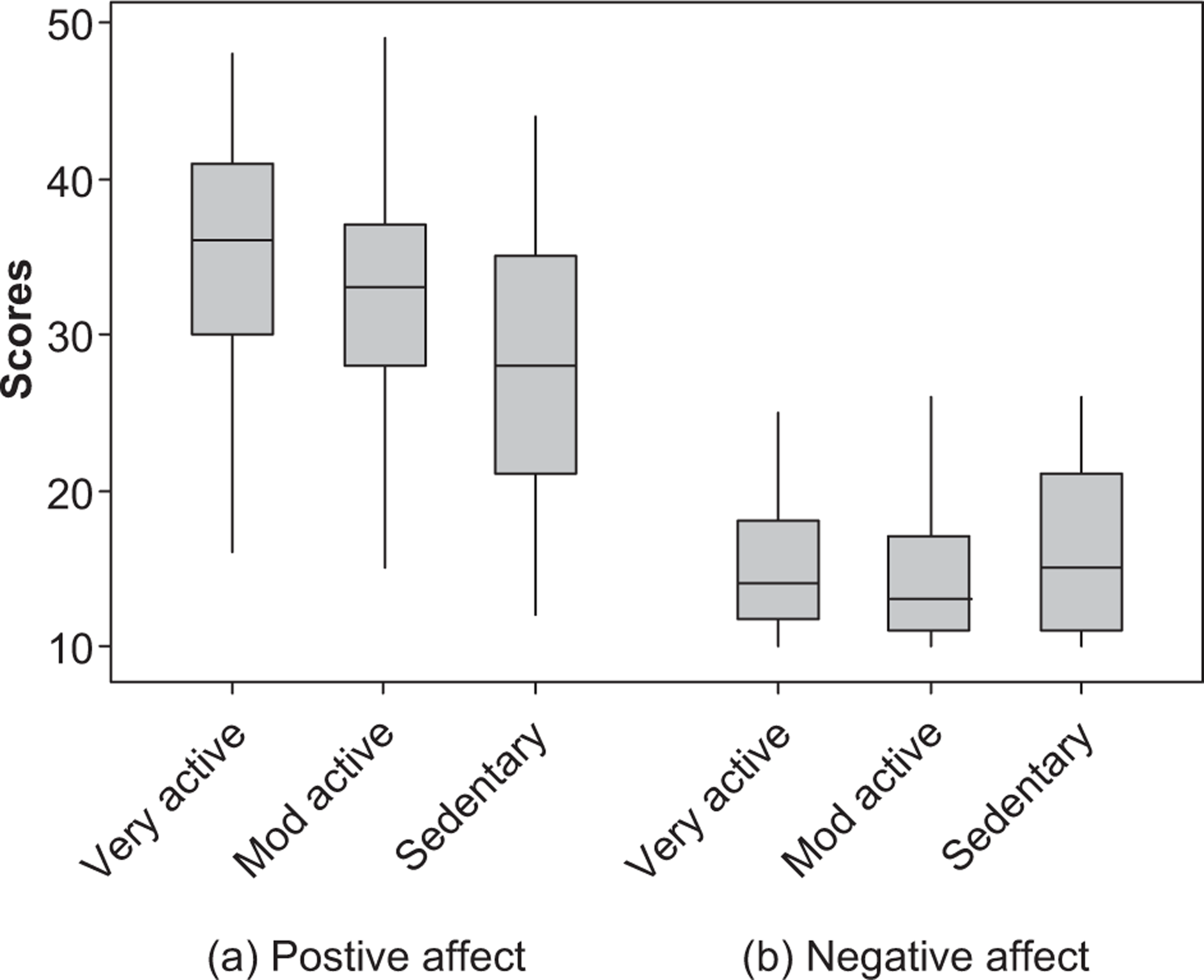
Boxplot showing scores for (a) positive affect and (b) negative affect according to physical activity levels: very active, moderately active (mod active) and sedentary (Kruskall-Wallis test, p = 0.001 and 0.3, for positive and negative affect scores, respectively). The median score and interquartile range is represented in each box, together with an indication of the range of values for each category of physical activity.
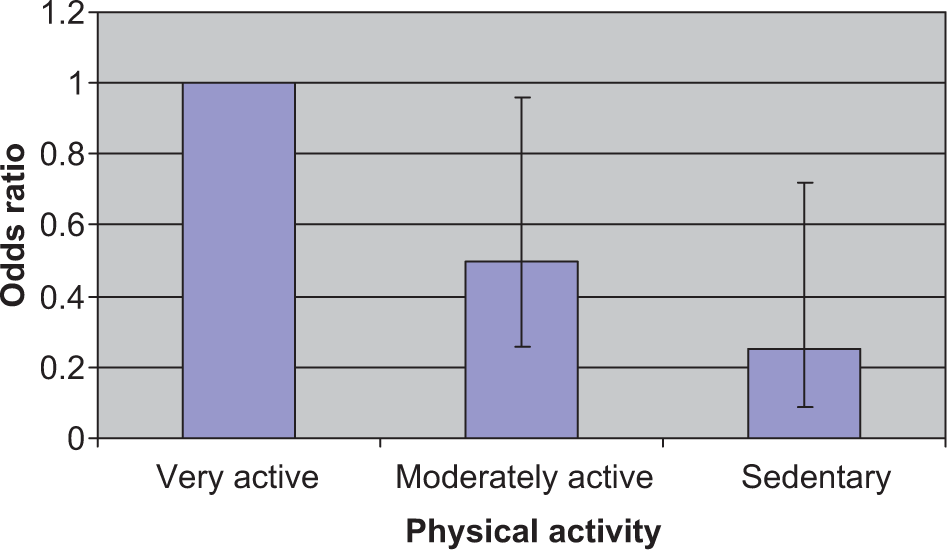
Histogram showing the likelihood for positive affect score in the highest tertile according to physical activity levels, after adjusting for body mass index and use of three or more prescription medications (error bars represent the 95% confidence intervals). The very active group is the reference.
Characteristics of subjects categorized into different levels of physical activity. Values are presented as mean (± SD), median (interquartile range) or n (%)
Discussion
The data presented in this study support a relationship between higher levels of physical activity and better mood states as measured by positive affect scores. In this group of women we found that positive affect scores diminished with lower levels of physical activity. This association was independent of body mass index and medication use, and was not explained by age, smoking, alcohol intake, SES or negative affect scores. No association was found between physical activity and negative affect. Habitual physical activity is thus associated with emotions such as interest, excitement, enthusiasm and alertness, as they are indicative of high positive affect [16, 17].
Many previous studies have linked physical activity with mental well-being. Physical activity interventions have been shown to reduce depressive symptomatology [23] and alleviate symptoms with a magnitude of effect equivalent to that of antidepressant medication [24]. There are reports of enhanced positive affect following physical activity sessions in some [11–13, 25–27], but not all [28], investigations. In studies of college-age students, higher levels of total physical activity [26] and involvement in taekwondo exercises [13] were both reported to induce positive mood state changes. Improvements in affect have been reported in middle-aged individuals following aerobic line dancing [11] and maximal exertion through walking exercises has also been shown to elicit acute mood response in women by increasing self-esteem [12]. A randomized controlled trial among seniors residing in intermediate care and self-care retirement facilities demonstrated that programmes involving resistance and balance training on the one hand, and flexibility and relaxation techniques on the other, both resulted in improvements in positive affect scores [27]. The influences of self-initiated habitual physical activity on affect have been reported in a case-control study involving cases with major depressive disorder and controls who had never been depressed: in response to physical activity, both groups reported higher positive affect scores whereas negative affect scores remained unchanged [25].
There are several psychosocial advantages to being physically active. Scheduling exercise into a productive routine has been shown to be useful in the management of mood [29]. Exercise increases one's sense of self-efficacy. It also is frequently associated with social engagement, and this has clear benefits in modifying mood [30]. Outdoor activities may also increase exposure to sunlight, guarding against vitamin D deficiency that is particularly common in affective disorders [31,32].
There are also several neurobiological sequelae to physical activity that are consistent with positive effects on mood. Regular exercise increases the availability of the monamine neurotransmitters, serotonin [33] and noradrenaline [34], attenuates the hypothalamic–pituitary–adrenal axis response to stress [35], increases the levels of neurotrophins such as brain-derived neurotrophic factor [36], reduces inflammation, which is well documented in depression [37] and reduces oxidative stress, which has similarly been shown to be present in depression [38,39].
Limitations of our study include the accuracy of self-reported physical activity, with the possibility of differential recall influenced by mood and well-being. Multi-prescription use served as a surrogate for comorbid disease, which was not directly addressed. It is possible that other components of physical activity such as social engagement may have contributed to the beneficial effects of exercise. Robust measures of depression and anxiety were not employed in this study; such measures would have been useful in elucidating links between physical activity, positive and negative affect, and mental health well-being. As this is a cross-sectional study, directional causality cannot be addressed. However, we found some agreement between the level of physical activity utilized in this analysis, and those reported by study participants approximately two years earlier (κ = 0.3, data not shown). Habitual physical activity thus remains reasonably stable over time, supporting the posited notion that physical activity influences mood.
This study supports the concept that the impact of physical activity on mood is associated with changes in positive affect rather than negative affect. Although causality cannot be claimed, these results warrant further investigations into the mechanistic interplay between neurobiological and psychosocial factors that might underlie this association. The findings add further support to our previous work [9,40–42] demonstrating that lifestyle plays a role in common mental disorders. Our findings add to extant literature suggesting that positive and negative affect are independent constructs and support the tenet that mood-modulating strategies might operate via positive affect. Further studies are needed to identify which aspects of positive and negative affect are influenced by physical activity and to quantify dose– response relationships to clarify how much physical activity and what type is required to optimize mood states.