
Abstract
The validity of the diagnoses for psychosis is currently under debate in connection to the development of the revisions of international diagnostic systems for mental disorders [1,2]. Several diagnostic subtypes have been described for schizophrenia and other non-affective psychoses in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) [3], and the International Statistical Classification of Disorders, tenth revision (ICD-10) [4] with the goal to differentiate between patients with regard to symptomatology, duration, illness severity, and course. The extent to which this has been confirmed is inconclusive.
The DSM-IV provides several diagnostic subtypes (paranoid, undifferentiated, residual, catatonic and disorganized) to characterize patients with schizophrenia. These subtypes are diagnosed when certain symptoms at the time of evaluation are present or were most recently present. The addition of a subtype to a diagnosis should therefore be seen as an indication of the symptoms at a given moment in time. In the paranoid subtype, being the most prevalent schizophrenia diagnosis, positive symptoms dominate. In disorganized schizophrenia, a more severely socially disrupting subtype, behavioural and emotional disturbances characterize the disease [5]. A third type, undifferentiated schizophrenia, does not have a specific profile of symptoms. Differences between these diagnostic subtypes have not been well reported [6], and the extent to which such categorical distinctions have concurrent validity is a matter of debate. The DSM-V task force proposes to disregard these subtypes.
The validity of schizophrenia and other non-affective psychotic disorders diagnoses remain controversial as well. Some researchers claim that a distinction between schizophrenia and schizoaffective disorder exists based on neurophysiological [7] and premorbid functioning levels [8]. Others claim that schizoaffective disorder is not a distinct diagnosis [9–11]. The distinction between schizophrenia on the one hand, and brief psychotic disorder and psychosis not otherwise specified (NOS) on the other hand, is less debated. Patients with brief psychotic disorder and psychosis NOS have different characteristics with regard to severity of psychopathology and social functioning [12].
Most studies on differences between schizophrenia spectrum diagnostic categories have been based on small sample sizes coming from single clinical settings. This may have resulted in biased conclusions on possible differences between several diagnostic categories. It may also have led to study results that are difficult to generalize between different clinical settings.
The Genetic Risk and Outcome of Psychosis (GROUP) project has been designed to study genetic and environmental vulnerability and resilience factors for variation in the expression and course of recent onset non-affective psychotic disorders in a national cohort study. For an overview of the GROUP structure, data flow, quality control, recruitment and sample characteristics of the studied patients we refer to Korver et al. [13]. The purpose of the current report is to investigate the validity of the diagnostic categories and subtypes of the included patients in the GROUP project, using DSM-IV as diagnostic tool, demographic and clinical characteristics, severity of psychopathology, social functioning and indicators of quality of life.
Methods
Participants
Participants were all part of the GROUP project (For an overview of the GROUP structure, data flow, quality control, recruitment and sample characteristics of the studied patients we refer to Korver et al. [13]). Participants were identified through clinicians working in regional psychosis departments or academic centres, covering 75% of the Netherlands and a part of the Dutch speaking part of Belgium, whose caseload was screened for inclusion criteria. Subsequently, consecutively encountered outpatients and inpatients were recruited for the study.
Demographic and clinical characteristics of the participants are provided in Table 1. Inclusion criteria were: (i) age range of 16 to 50 years (extremes included), (ii) a diagnosis of non-affective psychotic disorder according to the DSM-IV criteria [3], (iii) good command of the Dutch language, (iv) able and willing to give written informed consent, and (v) maximal duration of 10 years after first mental health care contact.
Demographic and clinical characteristics of patients in the GROUP study, means (SD) and absolute numbers (%) for schizophrenia, schizoaffective disorder, schizophreniform disorder, psychotic disorder NOS and brief psychotic disorder
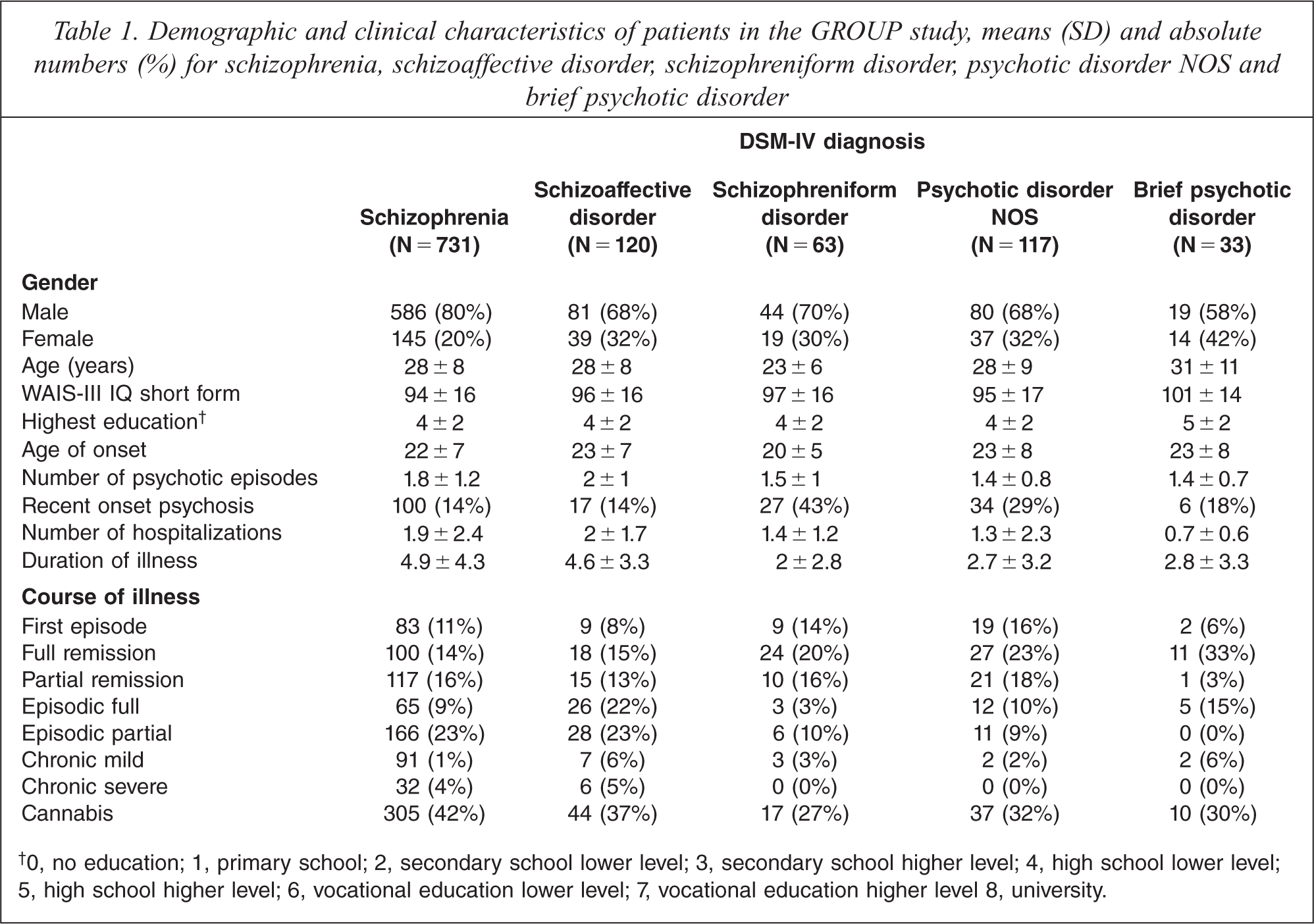
0, no education; 1, primary school; 2, secondary school lower level; 3, secondary school higher level; 4, high school lower level; 5, high school higher level; 6, vocational education lower level; 7, vocational education higher level 8, university.
Interviewers conducting assessments consisted of research assistants, psychologists, psychiatrists, nurses and PhD students who were all well trained in assessing interviews, rating and scoring (for detailed information on training procedures we refer to Korver et al. [13]).
Materials
Demographic and clinical characteristics
The Life Chart Schedule (LCS) [14] was used to assess clinical characteristics with respect to course of symptoms, current residence status and current work status. The interview was also used to collect demographic data. General course of symptoms was divided into first episode, recurrent, and chronic course. Course of negative symptoms was scored ordinally (0 = no symptoms, 1 = one or two symptoms mildly present, 2 = one or two symptoms clearly present, 3 = more than two symptoms mildly present, 4 = more than two symptoms clearly present). During the LCS interview, assessed by trained raters, details were elicited on changes in course. The reliability was fair to excellent for LCS ratings of duration of experience (ICC ranged from 0.53 to 0.99), quality of experience (kappa ranged from 0.46 to 0. 92) and long-term time trends (kappa ranged from 0.66 to 0.94).
An estimation of IQ score was calculated after assessing the short version of the Wechsler Adult Intelligence Scale, third edition (WAIS-III), that included tasks on processing speed, world knowledge, working memory, and reasoning and problem solving [15].
Diagnostic assessment
To assess DSM-IV diagnosis two structured diagnostic instruments were used: the Comprehensive Assessment of Symptoms and History (CASH) [16] and Schedules for Clinical Assessment for Neuropsychiatry (SCAN) [17]. The CASH includes the Scale for the Assessment of Positive Symptoms (SAPS), with 34 items measured on an ordinal scale ranging from 0 (absent) to 5 (severe) [18] and the Scale for the Assessment of Negative Symptoms (SANS), with 21 items [19].
The SCAN is the successor of the PSE-9 [20], which was the World Health Organization (WHO) standard instrument for psychotic disorder from 1974 till 1992. It is a semi-structured computer-based interview to assess psychiatric symptoms, using DSM-IV and ICD-10 compatible algorithms, constructed by the WHO-SCAN Advisory Committee [17]. The SCAN covers Axis I disorders. Interrater reliability of the diagnostic classification according to DSM-IV was evaluated by assessing the concordance between the diagnosis assessed by the interviewers and by the treating clinician. A randomly selected comparison of 65 subjects with a psychotic disorder revealed a difference in diagnosis in one case: schizoaffective disorder versus schizophrenia undifferentiated type.
Assessment of severity of psychopathology
The Positive and Negative Syndrome Scale (PANSS) [21] is currently the most widely used scale to assess the severity of a variety of symptoms in patients with schizophrenia It consists of 30 items, each item ranging on a 7-point scale of severity from 1 (absent) to 7 (extreme). Interrater reliability of the PANSS assessment in the GROUP study was evaluated with interclass correlation coefficient (ICC). Positive subscale score was 0.957 (95% confidence interval 0.808 to 0.997), ICC of PANSS negative subscale score 0.911 (95% confidence interval 0.606 to 0.994), ICC of PANSS total score 0.946 (95% confidence interval 0.758 to 0.996).
Assessment of premorbid and current functioning
The Premorbid Adjustment Scale (PAS) [22] is designed to evaluate the degree of achievement of developmental goals at each of several periods of a subject's life before the onset of schizophrenia (age epochs: <12, 12–16, and 16–19 years old). Interrater reliability and internal consistency have been found to be high [22]. Current functioning was measured by the Global Assessment of Functioning (GAF) scale [3]; the scores were split into symptom scores (GAF-S) and function scores (GAF-F) to improve psychometric properties.
Indicators of quality of life and needs
The World Health Organization Quality of Life – Bref [23], contains four major domains: physical, psychological, social relationships and environment.
The Camberwell Assessment scale of Need Short Appraisal Schedule (CANSAS) [24] has 22 individual domains of clinical and social needs (e.g. psychotic symptoms, physical health, accommodation, and intimate relationships) which are scored on a 3-point scale (no need, met need, and unmet need). The interrater reliability of the CANSAS was assessed under routine conditions. Agreement on the identification of an area of need was high, higher on patient ratings than on staff ratings [25].
Statistical analyses
One way analyses of variance (ANOVAs) were conducted to investigate differences between groups. Chi-square analyses were used for categorical variables. To investigate group differences, analyses were performed with two-tailed hypothesis testing with α = 0.01. For differences between groups, Bonferroni post hoc tests were performed. The statistical analyses were performed using SPSS 16.0.
Firstly, analyses were restricted to the subtypes of schizophrenia. Subtypes consisting of less than 30 participants were excluded from analysis. Thereby, our analyses were based on comparisons between paranoid, disorganized, and undifferentiated types of schizophrenia. Next, analyses were conducted to investigate significant differences between the patient groups with different non-affective psychotic disorders (schizophrenia, schizoaffective disorder, schizophreniform disorder and brief psychotic disorder/psychotic disorder NOS). The latter two were combined to enlarge the group sample size. Analyses of covariance (ANCOVA) were performed in order to control for age, gender and age of illness onset. Other demographic and clinical variables were not controlled for, since these were considered to be potentially specifically related to diagnosis or subtype.
Results
1064 patients were included in the present study out of the 1120 GROUP participants. The diagnosis of schizophrenia was most frequent (69%), followed by schizoaffective disorder (11%), psychotic disorder NOS (11%) schizophreniform disorder (6%) and brief psychotic disorder (3%). The majority of the schizophrenia sample were diagnosed with the paranoid subtype (82%), followed by undifferentiated subtype (9%), disorganized subtype (6%) and residual type (3%). A large part of the population consisted of Caucasian (74%) male (76%) participants. The origins of non-Caucasians were from a great variety of countries and cultures, including Morocco, Turkey, Surinam and several Asian countries. The mean age of the total population was 28, which is 5 to 6 years older than the mean age at onset of psychosis. About 18% of the patients had duration of illness of less than 1 year. The mean total IQ score was 95 and there were no differences found between the groups.
Schizophrenia subtypes
Demographic and clinical characteristics
No significant differences were found with regard to demographic and clinical characteristics.
Severity of psychopathology
A very marginal significant difference was found on the disorganization factor of the PANSS (F2,653 = 2.581; p = 0.077). Patients of the paranoid subtype reported less disorganization, as compared to disorganized patients (p = 0.077). The difference became more apparent after controlling for highest educational degree (p = 0.002 and p = 0.009, respectively).
Current and premorbid functioning and indicators of quality of life
No significant differences were found either with regard to social functioning or indicators of quality of life.
Non-affective psychosis diagnostic categories
Table 2 shows the mean and standard deviation of the severity of psychopathology, the level of premorbid and current functioning and quality of life scores.
Severity of psychopathology, level of social functioning, quality of life, mean scores (M) and standard deviations (SD) for patients with a diagnosis of non-affective psychosis: Schizophrenia, schizoaffective disorder, schizophreniform disorder, psychotic disorder NOS and brief psychotic disorder
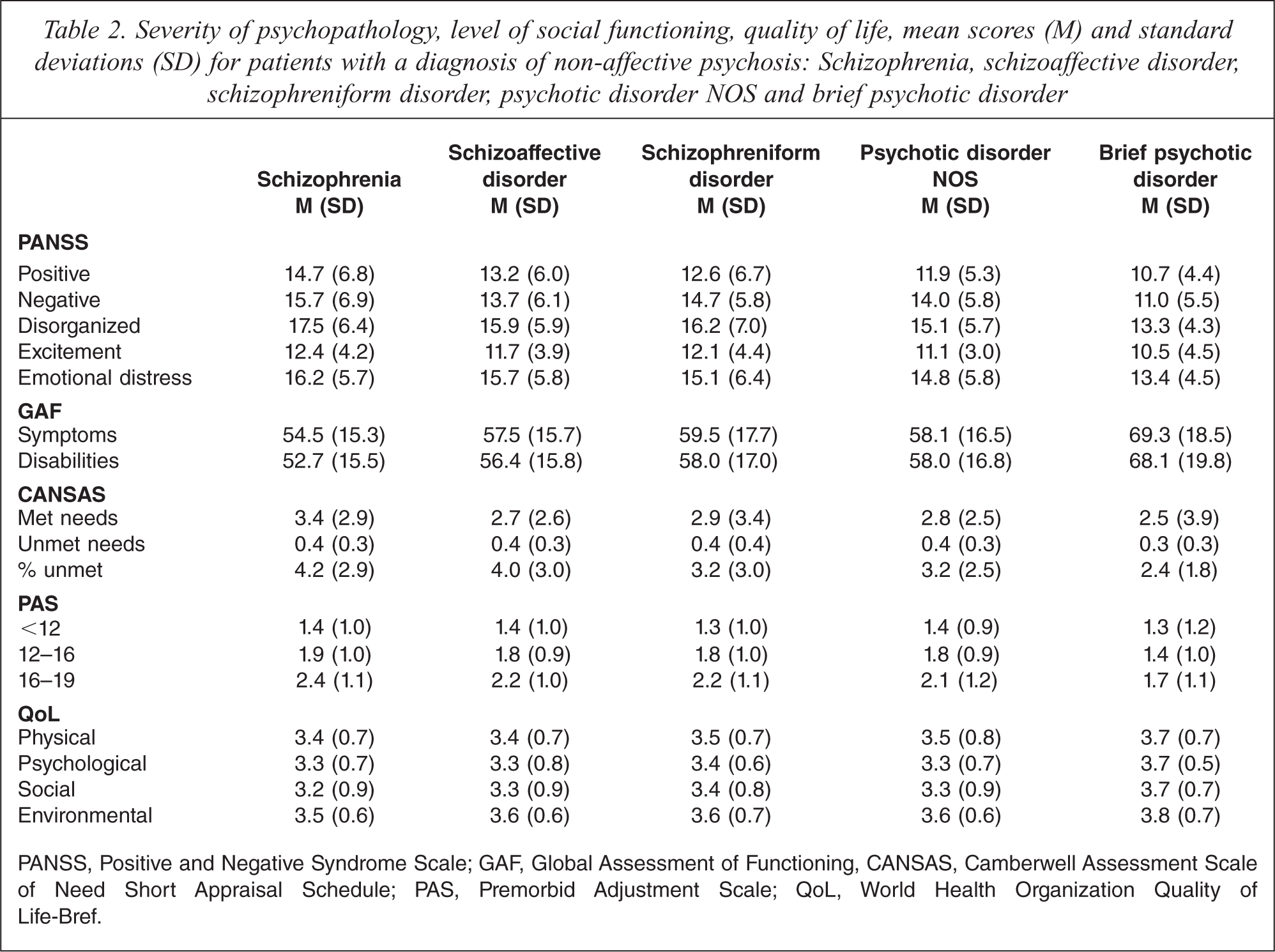
PANSS, Positive and Negative Syndrome Scale; GAF, Global Assessment of Functioning, CANSAS, Camberwell Assessment Scale of Need Short Appraisal Schedule; PAS, Premorbid Adjustment Scale; QoL, World Health Organization Quality of Life-Bref.
Demographic and clinical characteristics
The four diagnostic groups (schizophrenia, schizoaffective disorder, schizophreniform disorder and brief psychotic disorder/psychotic disorder NOS) differed in age (F3,1063 = 6.80; p < 0.001), gender (X2 (2) = 21.31; p < 0.001), recent onset psychosis (X2 (3) = 56.66; p < 0.0001), course of illness (X2 (6) = 58.97; p < 0.001) and course of negative symptoms during remission or chronic psychosis (X2 (12) = 41.44; p < 0.001), number of psychotic episodes (F3,1025 = 6.12; p < 0.001), duration of illness (F3,989 = 17.76; p < 0.001), number of hospitalisations (F3,823 = 6.35; p < 0.001).
Post hoc analyses revealed that patients with a schizophreniform disorder were significantly younger as compared to the schizophrenia (p < 0.001), schizoaffective (p < 0.001) and the brief/NOS (p < 0.001) populations. Brief/NOS patients had a significantly lower number of psychotic episodes as compared to patients with schizophrenia (p = 0.002) and schizoaffective disorder (p = 0.001).
The schizophrenia sample experienced significantly longer duration of illness than patients with brief/NOS (p < 0.001) and schizophreniform disorder (p < 0.001). The same was found for the schizoaffective sample compared to patients with a brief/NOS (p = 0.001) and schizophreniform disorder (p < 0.001). Compared to the sample with brief/NOS, patients with schizophrenia (p = 0.001) had experienced significantly more hospitalizations.
Severity of psychopathology
As assessed with the PANSS, significant differences were found with regard to positive (F3,976 = 9.03; p < 0.001) and negative symptoms (F3,965 = 6.15; p < 0.001), disorganization (F3,969 = 7.96; p < 0.001), excitement (F3,988 = 4.40; p = 0.004). Post hoc analyses revealed that patients with schizophrenia had significantly more severe positive (p < 0.001) and negative symptoms (p = 0.003), disorganization (p < 0.001), excitement (p = 0.004) as compared to brief/NOS patients. These differences remained significant after controlling for covariates except for excitement (p < 0.001, p = 0.005, p = 0.001 respectively).
Premorbid and current functioning
Significant differences were found between diagnostic categories with regard to GAF symptoms (F3,950 = 5.88; p = 0.001) and GAF disabilities (F3,950 = 8.31; p < 0.001). Concerning premorbid adjustment as assessed with the PAS, significant differences were found only for the age category 16–19 years old (F3,873 = 4.45; p = 0.004). Post-hoc analyses revealed significantly worse GAF symptom (p = 0.003) and disability scores (p < 0.001) for the schizophrenia population as compared to the brief/NOS. The same applied to the difference in GAF disability scores between schizophrenia and schizophreniform disorder, but only after controlling for covariates (p = 0.009). Furthermore, the schizophrenia population had a significantly lower PAS score considering the age category 16–19 years old (p = 0.006), as compared to the brief/NOS population, even after controlling for covariates (p = 0.011). No other significant differences were found.
Indicators of quality of life
As assessed with the CAN, a significant difference was found for number of met needs (F3,952 = 6.26; p < 0.001). A post-hoc analysis revealed that the schizophrenia patients had significantly more met needs (p = 0.001) as compared to the brief/NOS patients. This remained significant after controlling for covariates (p = 0.001). No significant differences were found with regard to quality of life.
Discussion
In this study we focused on the concurrent validity of the diagnostic subtypes and categories in a large sample of patients with a non-affective psychotic disorder participating in the GROUP project. Differences within patient groups between schizophrenia subtypes and between diagnostic categories were studied on demographic and clinical characteristics, course of illness, severity of psychopathology, premorbid and current functioning, and quality of life.
Overall, we found no support for a distinction between different schizophrenia subtypes. Apart from the disorganized group who experienced more disorganization symptoms (although not statistically significant), we did not find any meaningful distinction between any of the subtypes on demographic or clinical characteristics, course of illness, severity of psychopathology, social functioning, or quality of life. Our findings are in contrast with a recent study by Suvisaari et al. [26] who found support for the descriptive and predictive validity of the disorganized subtype as compared to undifferentiated and paranoid subtypes. However, the fact that this subgroup differed may be attributable to a small population of studied patients, who were relatively old. The present findings indicate that the schizophrenia subtypes are not valid, which may fuel the ongoing discussion in the DSM-V psychosis workgroup currently questioning the concurrent validity of these subtypes [1,6]. Although the findings are based on DSM-IV diagnoses, they may also be relevant in light of the development of the ICD eleventh revision, especially after the very recent ‘Global Survey Study of Psychiatrists’ Attitudes toward Mental Health Disorder Classification' [27], from which the World Health Organization uses the results for the ICD revision process. In this survey, psychiatrists around the world (44 countries) show their support for working with dramatically fewer categories, which are described as having poor utility in clinical practice.
Our findings concerning differences between schizophrenia spectrum diagnostic categories can be summarized as follows. In patients with a diagnosis of schizophrenia or schizoaffective disorder, clinical characteristics were more severe as compared to patients with other non-affective psychoses. Compared to brief/NOS patients, patients with schizophrenia had worse scores across three out of five symptom dimensions [28,29] and measures of social functioning. Patients with schizophreniform disorder were younger as compared to the brief/NOS group. This finding is unsurprising since patients with a schizophreniform disorder have by definition a shorter duration of the disorder. The present study supports a distinction between schizophrenia and other diagnostic categories of non-affective psychosis, such as brief psychotic disorder and psychotic disorder NOS. The latter groups, which encompassed approximately 12% of the included patient population, were found to be less severely disturbed, and full remission after one psychotic episode was highly prevalent in this population. There was no convincing evidence in favour of a distinction between schizophrenia and schizoaffective disorder. Malhi et al. [11] suggest that schizoaffective disorder should be removed from the DSM-V. The current findings give some support to this suggestion. In addition, the fact that no differences were found between all other non-affective psychotic disorders, besides schizophrenia, could be a suggestion for removing these entities in DSM-V as well, although this should be interpreted with caution because of the relatively small sample sizes of these diagnostic groups compared with schizophrenia.
Although some differences between diagnostic groups were found, most of the current study results support the idea that the current DSM-IV diagnoses for psychotic illness may lack validity. These findings may also be useful to consider in reference to the ICD-11 revision. Rather than comparing groups categorically, it may be more useful to study categorical representations in combination with dimensional representations [30]. This may lead to better utility in terms of conveying clinical information of psychosis. Thereby, psychosis is not perceived as an illness that is either present or absent, but as a syndrome with a need for care in case symptoms reach a certain threshold [31,32]. Van Os proposed three sub-categories to describe the combinations of dimensional psychopathology: affective expression (high in depression/mania), developmental expression (high in developmental cognitive deficit/negative symptoms), and not otherwise specified (high in disorganization/positive symptoms). However, the validity of this approach needs evaluation.
Some limitations of the current GROUP study are worth mentioning. Firstly, selection bias: participants willing to participate in a demanding study protocol may be different from participants in other schizophrenia studies that are less demanding, or from subjects refusing participation in research. Unfortunately, the response rate of the subjects approached was not evaluated. Secondly, despite massive investment, inter-rater reliability remains a vulnerability of large collaborations. Thirdly, we did not have enough patients diagnosed with schizophrenia residual type for inclusion in our analyses, although this may also be interpreted as evidence supporting the idea that this subtype is not prevalent in clinical samples, or at least is not diagnosed frequently. Fourthly, since the GROUP project was designed to study patients with a relatively recent onset of psychosis our sample was young of age and therefore not representative of schizophrenia as a whole. In addition, the majority of the cases with a diagnosis of schizophrenia had received a paranoid subtype, which led to an unequal amount of cases between the subtypes groups. Finally, we decided not to differentiate between brief psychotic disorder and psychotic disorder NOS diagnoses which may have limited concurrent validity themselves.
The current paper mainly focused on differences and similarities between diagnostic groups within a sample of patients with varied psychotic disorders. In light of the actual DSM-V and ICD-11 discussion regarding a categorical versus dimensional approach, our findings can be of value. In the coming years of follow up of our sample, we will address the research questions of the current paper longitudinally.
Acknowledgements
GROUP contributors
Amsterdam
Academic Medical Centre: S.E. van den Berg, C.L.A. Schroeder, R. van der Valk, N. Dekker, C.J. Meijer, N. Korver, L.N. Boyette, J. Meijer, D. van Dam; GGZ Ingeest: I. de Rijke, S. Huinink, R.J. de Vries, M. Jansen, D. Bos; Arkin: W.P. Hoen, E.M. te West, S.H.J. Groeneveld, E.M. Vergunst, M. Swets, S. Vothknecht, I. Poleacov; Dijk en Duin: D. van Dijk, S. de Metz, M.T. Hasty, G. Geertsa, P.M. de Baaij, A. Metzger; Erasmus University Medical Centre: N.J.M. van Beveren, M. Baldini; GGZ INgeest: F.D. Grimbergen, M.A.M. Boerma, C. Agsteribbe; GGZ Noord Holland Noord: H.P. Wisman, M.A.H. Monden, M.M. Bosman, M. van Dijk; Rivierduinen: R. Klaassen, T. van der Tang, B. Luteijn, H. Winkel, H. Weisz, A.C.P. Strater, A. Landman, M. Vorstenbosch.
Maastricht
D. Op ‘t Eijnde, K. Lenders, S. Loyen, R. Roberts, K. Sweers, H. Gielen, N. Soons, A. Hintzen, V. Habets, I. Riské, C. Vossen, E. Martens, S. Apers, L. Wijnhoven, E. Konings, T. Lataster, M. Lardinois, D. Versmissen, C. Simons, M. van der Werf, P. Habets, S. Pfeifer, E. de Loore, M. Heins, M. Oorschot, M. Meys, M. Dietvorst, C. van Zelst, I. Crolla, R. Mengelers, F. van Goethem, W. Beuken, D. Byniam, T. Driesen, M. Marcelis, G. Driessen, A. Shazad, R. van Winkel, C. Henquet, G. Kenis, P. Delespaul.
Utrecht
Academic Medical Centre: P. Anema, E.M.J. van Baaren, S.C. Bakker, H.B.M. Boos, E. Caspers, E.M. Derks, S. van Hemert, A. Hemkes, R. Hijman, M. van Leeuwen, J.E.H. Machielsen, R.A. Ophoff, M. Rais, M. Salden, H. van Someren, E. Strengman, M. Vleesschouwer; Symfora: M. van Beek, P.N. van Harten, J.P.F. Koning, W. Schep; Meerkanten: M.G. Vollema, P. Prins, T. Viester; Altrecht: A. Akdeniz, K. Verweij, N. Kaymaz; RIAGG Amersfoort: F. v.d. Heuvel, B. v.d. Goot; Delta: J.E. Hovens, A.J.M. Loonen.
Groningen
UMCG Groningen: J. Bous, M. Veenstra, E. van ‘t Hag, P.J. Quee, F.J. Nienhuis, H.G.O.M. Smid, E. Veermans, A.A. Bartels; Lentis: F. Duijndam, T. Lugtenberg, H. Knegtering; GGZ Friesland: W. Blaauw, A. Wunderink; GGZ Drenthe: K.P. Touw, J. Arends, C.J. Slooff; Dimence: J. Brilman, M. Schomaker, M van Wijk, A. Wessels; Mediant GGZ Twente: E. Vroom, K. Meijerink; GGNet: I. Bogert, W. Janssen, H. de Berk, E.O. Noorthoorn; Parnassia: H. Ising, J.D. Blom, M. van der Gaag; De Grote Rivieren: G. Mensen, R. van der Snoek, R. Smit, G. Faber.
The GROUP project was supported by a grant from the Netherlands Organization for Health Research and Development (ZonMw), within the Mental Health Program (project number: 10.000.1001). ZonMw had no further role in study design, in the collection, analysis and interpretation of data, in the writing of the report, and in the decision to submit the paper for publication. All other authors declare that they have no conflicts of interest. The authors alone are responsible for the content and writing of the paper.